
Abstract
Background and Aims:
To prevent severe prosthetic joint infections, a dental examination is usually recommended prior to arthroplasty, even sometimes regarded resource- and time-consuming. The aim of this study was to determine whether a risk factor-based algorithm could be created to send only selected patients for dental clearance.
Materials and Methods:
A prospective study of 952 patients scheduled for elective arthroplasty was performed. Patients filled out a questionnaire regarding potential risk factors for dental infections, and dentists documented patients’ oral health and interventions performed (data available for 731 patients).
Results:
Of the patients, 215 (29.4%) failed dental clearance; a total of 432 teeth were extracted, 32 patients (4.4%) required root canal treatment, and 37 patients (5.1%) had severe periodontitis. Independent risk factors for failure were history of root canal treatment (odds ratio: 2.282, 95% confidence interval: 1.346–3.869, p = 0.020), use of tobacco products (odds ratio: 1.704, 95% confidence interval: 1.033–2.810, p = 0.037), dental visit indicated by oral symptoms within 3 months (odds ratio: 1.828, 95% confidence interval: 1.183–2.827, p = 0.007), or visit to a dentist within 6 months (odds ratio: 1.538, 95% confidence interval: 1.063–2.224, p = 0.022). Regular dental examination was a preventive factor (odds ratio: 0.519, 95% confidence interval: 0.349–0.773, p = 0.001). However, based on the examined risk factors, no sufficiently large group of patients at lesser risk for dental infections could be identified.
Conclusion:
Because of the high need for dental care revealed by our unselected patient population, the inspection and treatment of dental pathology of all patients are important interventions prior to elective arthroplasty.
Keywords
Introduction
Periprosthetic joint infection (PJI) is a devastating complication of prosthetic hip or knee surgery, causing significant morbidity and mortality: reoperations, extensive antimicrobial treatments, and prolonged hospital stays (1). The incidence of acute PJI following hip or knee arthroplasty is estimated to be 1%–2% (1), and incidence of late hematogenous infections is 0.05%–0.07% per prosthesis-year (2). Perioperative acute or chronic infection at any site is of great importance and elimination of these infections is a valuable step to lower the risk for a PJI (3) and is likely to benefit the patient. Oral bacteria cause 6%–13% of PJIs (1, 4). Poor dental health is considered a modifiable factor to improve the success of joint arthroplasty (5), and it is common practice to screen patients for oral infections and treat infections before an elective arthroplasty operation (6). A recent study discovered 31% lower incidence of PJI if the patients’ teeth were scaled regularly (7).
Only a few studies have examined dental pathology in patients planning to have a hip or knee arthroplasty. These studies have found that 23% of patients required treatment for dental infection or caries (8), 12% had an infection requiring root canal treatment or tooth extraction (9), and 29% had clinically significant periodontal disease (10). Periodontal health has been shown to affect the incidence of daily oral bacteremia, and infection incorporating the entire periodontium is equivalent to a wound area of 20 cm2 (11, 12).
A promising approach of selective dental clearance based on risk factors has been published from the United States with a sample size of 300 patients; the patients with no tobacco or narcotic use and who have visited a dentist within the past 12 months were shown to be at significantly lower risk for dental infections than were other patients (6% vs 37%) (9). Screening all the patients for an active oral infection at least with a risk factor-based questionnaire has been recommended by the International Consensus on Periprosthetic Joint Infection (13). The dental clearance of all patients is also under discussion in Finland: the common practice is to inspect the teeth of all patients before an elective hip or knee arthroplasty to diagnose and, if needed, treat dental infections before the operation. This study was performed to determine whether a risk factor-based algorithm could be created to safely send only selected patients for dental clearance.
Material and Methods
This prospective study included 952 patients scheduled for an elective hip or knee arthroplasty in the Hospital District of Helsinki and Uusimaa, Peijas Hospital, a public tertiary-care hospital in Finland, from January 2015 to March 2016. In this hospital district, all patients scheduled for an elective arthroplasty are required to have a dental examination and, if needed, treatment for dental infections. All study patients filled out a questionnaire on potential risk factors for dental infections. At the dental examination, the dentists filled out and signed a questionnaire with details about the actual clinical status of the patients’ oral health with relevance for possible bacteremia (e.g. gingival and periodontal health, mucosal health) and the interventions performed. In addition to thorough clinical examination, a panoramic tomography (PTG) was taken from each patient unless a recent PTG was available. When needed, other radiological imaging methods were used in addition.
Dentists filled out a questionnaire reporting patients’ actual oral health, including diagnosed oral pathologies regarded as possible oral infections or source for bacteremia, such as mucosal ulcers or other mucosal diseases, gingivitis, periodontitis (at least one tooth with ⩾4 mm periodontal probing depth (PD)), or severe periodontitis (attachment loss ⩾5 mm in ⩾30% of the remaining teeth) (14). In addition, the number of tooth extractions and root canal treatments performed following the examination were reported. The main endpoints for this study were diagnosis of severe periodontitis and tooth extraction or root canal treatment performed at the dental clearance.
Of the 952 scheduled patients, 830 were actually operated. A total of 731 patients (88.1% of the operated patients) returned the dentist-completed questionnaires at the time of preoperative visit or on the day of surgery. In total, 122 patients (12.8%) underwent surgery but did not return the questionnaires (although their teeth were screened by a dentist before the surgery), 75 patients were still waiting for the surgery, 18 surgeries were canceled because of diminished symptoms, and 6 patients died before the operation. Patients who did not return the dentist-completed questionnaire were excluded from the analysis (n = 221, 23.2%). Of the questionnaires filled in by patients, 65 (8.9%) were incomplete; of the questionnaires filled in by dentists, 31 (4.2%) were incomplete. Data from these questionnaires were included in the analysis to the extent that they were complete.
Data Collection and Endpoints
A questionnaire from a recent study was used as the basis for our questionnaire (9). Some questions were added, including whether all teeth had been extracted, or if the patient had a fixed dental implant, had been diagnosed with periodontitis, or had any dental health-related symptoms within the last 3 months.
Statistics
Univariate analyses were conducted with the chi-square test or Fisher exact test, as appropriate, for categorical variables, and with the Mann–Whitney U test for continuous variables. The potential risk factors with p-values below 0.2 in univariate analysis with confounding factors such as gender and age were selected for the multivariate analysis. The multivariate analysis was performed with a logistic regression model with a forward selection process. A p-value less than 0.05 was considered statistically significant. The analyses were performed with SPSS for Windows, version 23.0.
Ethics
Ethical approval was obtained from the Ethics Committee of the Department of Surgery, Helsinki University Hospital (no. 360/2014). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Results
Altogether 215 patients (29.4%) did not pass the dental inspection without coincidental treatment, or they were diagnosed with severe periodontitis and referred for special care. A total of 432 teeth were extracted from 187 patients (25.7%). Root canal treatment was performed on 32 patients (4.4%), and severe periodontitis was diagnosed in 37 patients (5.1%). In addition, 461 patients (63.3%) were diagnosed with gingivitis, 34 (4.7%) with mucosal ulcers or other mucosal disease, and 249 (34.3%) with at least one deepened periodontal pocket (PD ⩾ 4 mm). Of the 37 patients with no teeth, 10.8% were diagnosed with mucosal ulcers or other mucosal disease. Nearly half of all patients (359, 49.1%) visited a public healthcare dentist; the rest visited a private dentist, with no significant difference between these two groups in the number of dental pathologies requiring treatment (p = 0.104).
Among all studied risk factors, potential factors predisposing to oral infections are presented in Table 1. In multivariate analysis, the independent risk factors were history of root canal treatment, dental visits indicated by oral symptoms, use of tobacco products, and last visit to a dentist within 6 months (Table 2). Visiting a dentist regularly was a protective factor.
Potential risk factors predisposing to oral infection, determined by univariate analysis.
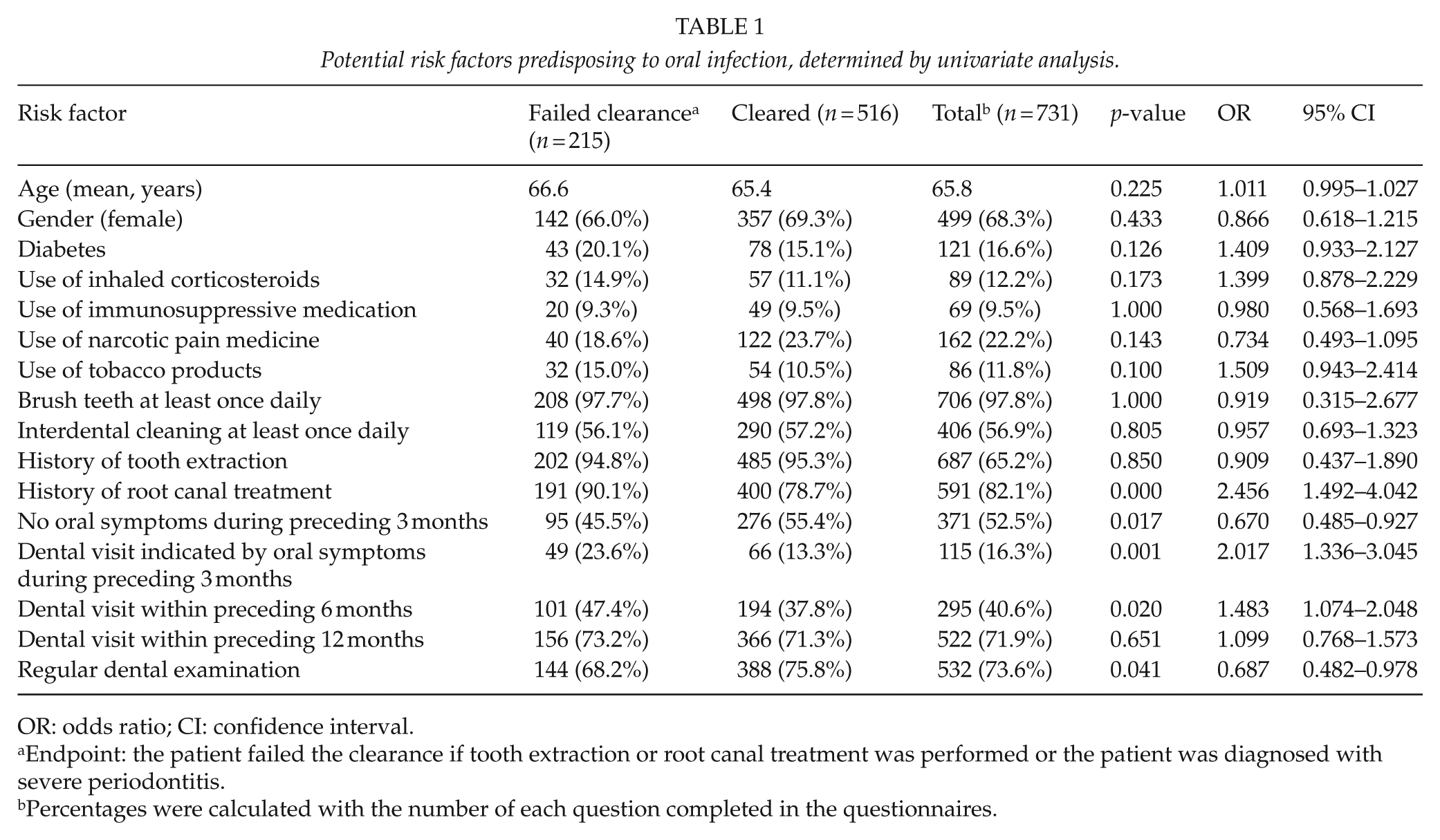
OR: odds ratio; CI: confidence interval.
Endpoint: the patient failed the clearance if tooth extraction or root canal treatment was performed or the patient was diagnosed with severe periodontitis.
Percentages were calculated with the number of each question completed in the questionnaires.
Independent risk factors predisposing to oral infection and causing failure at dental inspection, determined by multivariate analysis.
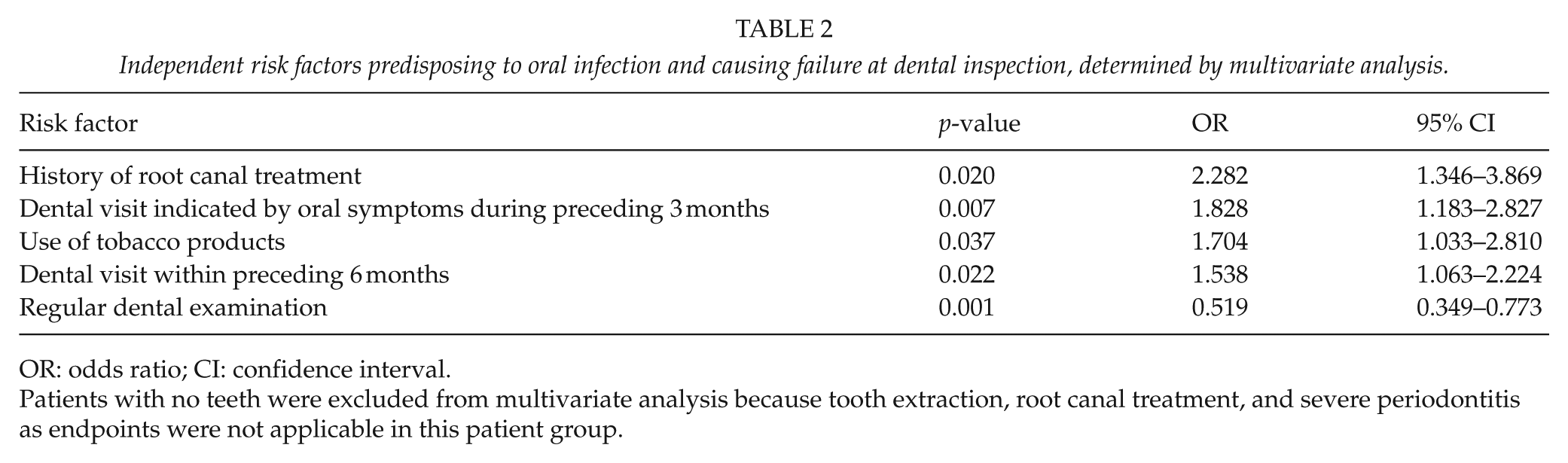
OR: odds ratio; CI: confidence interval.
Patients with no teeth were excluded from multivariate analysis because tooth extraction, root canal treatment, and severe periodontitis as endpoints were not applicable in this patient group.
A group with none of the independent risk factors was significantly less likely to fail the clearance than were the rest of the patients (8.1% vs 30.7% failed clearance, odds ratio (OR): 0.200, 95% confidence interval (CI): 0.061–0.657, p = 0.003), but comprised only 37 patients (5.1%). By experimentally combining groups, we were able to find one group (those with no history of root canal treatment and having frequent dental examinations) that was at 50% lower risk of falling into the treatment group at dental inspection than were the rest of the patients (15.0% vs 31.0% failed clearance, OR: 0.393, 95% CI: 0.208–0.744, p = 0.003), but only 80 patients (11.2%) belonged to this group.
The group of patients (no tobacco use, no narcotics, and dental examination within 12 months) found to be at lower risk for dental infections in the study by Tokarski et al. (9) constituted 69% of patients in our study. However, this group did not turn out to be less likely to fail clearance than were the rest of our study patients (30.2% vs 27.4% failed clearance, OR: 1.151, 95% CI: 0.810–1.636, p = 0.479).
Discussion
This study was performed to determine whether an algorithm could be created to send only selected patients to pre-surgery dental clearance based on their risk factors. The results showed that the need for dental care was high in the patient population, and it was not possible to find a sufficiently large group of patients at lower risk for dental infections that could safely bypass the dental examination.
The national status of dental health is important to consider when determining the strategy for preoperative dental screening. Finland’s national reports have indicated poor dental health in the adult population (15), which was also discovered in this study: almost 30% of the patients had a dental condition requiring treatment prior surgery. This proportion is clearly higher than that in previous studies performed in the United States (9%–23%) (8, 9, 16). However, our results are in line with an earlier published Finnish national report (15) in which 27% of patients were radiographically diagnosed with dental periapical lesions. Such periapical findings are likely the cause of the high number of extractions and root canal treatments in this study. This study did not ascertain whether dentists could have followed some of the diagnosed periapical lesions without immediate interventions, if no arthroplasty operation had been planned.
Severe periodontitis was diagnosed in 5% of the patients, which is significantly less frequent than the reported 21% in the national health survey (15). This difference may be partly explained by the different criteria applied for severe periodontitis. The prevalence of moderate gingivitis (34%) was similar to that detected prior to arthroplasty in Poland (29%) (10). Gingivitis and periodontitis are important oral pathologies to detect because they can be addressed by improving oral hygiene and by professional dental care.
With the endpoints used, none of the 37 patients who had all their teeth extracted required treatment for oral infections and thus they may not need to visit a dentist. It would, however, be advisable to check the oral cavity of patients wearing a full set of dentures to inspect the mucosa because a moderate portion of them were diagnosed with mucosal disease. The amount (11%) of mucosal ulcers or other mucosal diseases in our study was significantly smaller than expected based on the 51% recorded in the national report (15).
Previously published risk factors for failing dental clearance were narcotic and tobacco use, not having visited a dentist within 12 months, a history of pulled teeth, using interdental cleaner less than once daily, and older age (9). Of these, we found that only tobacco use had an impact on failure in dental clearance. The prevalence of most of the above-mentioned risk factors were similar in our study: narcotic use (22% of patients in our study vs 19% in the study by Tokarski et al. (9)), tobacco use (12% vs 11%), and using interdental cleaner less than once daily (44% vs 36%). However, in correlation with the poorer dental health in our population, more patients had last visited a dentist more than 12 months earlier (28% vs 13%) and almost twice as many patients had a history of tooth extraction (95% vs 55%). In our study, the age did not correlate with oral status as the mean age was similar in both groups (clearance or failure at dental examination). In the national health survey, the youngest age group of 34 years or younger had over half of the teeth healthy, but in the age group of 65 or over the proportion of healthy teeth was dropped to one-third only (15). However, the youngest age group rarely is a target for an arthroplasty operation.
Contrary to the previous study from the United States (9), we did not find a sufficiently large group of patients at lower risk of failing the dental clearance. Two groups of patients were at significantly lower risk of falling into the treatment group, but these groups were of insignificant size, representing only 5%–12% of the patients. Moreover, the group of patients suggested to be safely omitted from dental clearance in the previous study from the United States (9) did not prove to be so in this study in the Finnish population.
A study of 5004 patients discovered that patients were at 31% lower risk of having PJI if their teeth were scaled regularly (twice a year) during the 3-year period (7). All confounding factors could not be reliably ruled out, but the finding was nevertheless promising. Visiting a dentist regularly proved to be a protecting factor from failing dental clearance in our study. However, patients who had visited a dentist within the preceding 6 months were in a bit of higher risk of failure. This could be explained by patients’ need to be treated by a dentist because of symptoms and the treatments not having been completed by the time of the actual dental clearance. Seeking help for dental symptoms may partly reflect poor oral health or non-adherence to regular dental check-ups and treatment.
Strengths of this study lie in its large study population with a patient population not selected based on economic or insurance status. The weakness is shared by other questionnaire studies; the data of risk factors rely on patients’ self-reporting, and thus, the possibility of inaccurate answers exists. However, if dental clearance would be selected based on data reported by patients, the same risk of inaccurate answers would also exist in that situation.
Conclusion
Because of the high need for dental care revealed by our unselected patient population, we consider that thorough oral examination and treatment of dental pathology are important interventions prior to elective arthroplasty except for those patients who have all teeth extracted. When the need for dental treatment is high, dental clearance may not only protect from acute postoperative infections, but probably the inspection and the instructions given may also have an impact on the incidence of late hematogenous infections.
Footnotes
Acknowledgements
The authors thank Carol Ann Pelli from the Language Centre of University of Helsinki for her detailed reviewing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was obtained from the Ethics Committee of the Department of Surgery, Helsinki University Hospital (no. 360/2014).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author MV has received research support funding from the Finnish Orthopedic Association.
Informed Consent
Informed consent was obtained from all individual participants included in the study.