
Abstract
Purpose:
The study aims to analyze the demographics and microbiological profiles of hip and knee prosthetic joint infection (PJI) and to compare the microbiological differences between hip and knee PJI.
Methods:
We performed a retrospective study of all PJI cases between January 2006 and December 2014 at a referral medical center in Taiwan.
Results:
A total of 294 PJI cases were collected: 159 were identified as hip PJI and 135 as knee PJI. The most common causative pathogen was Staphylococcus aureus (78 cases, 27%), followed by coagulase-negative staphylococci (CoNS, 42 cases, 14%). Methicillin-resistant staphylococci (MRS) accounted for 21% of all PJI cases. Fungus and mycobacterium were only involved in 12 cases (4.1%) of all PJI cases. Polymicrobial pathogens, anaerobes, and enteric gram-negative bacilli (GNB) were more likely to occur in hip joint prostheses than in knee joint prostheses (22 vs. 6 cases, p = 0.006; 11 vs. 0 cases; p = 0.002; 20 vs. 6 cases; p = 0.014, respectively).
Conclusion:
The prevalence of polymicrobial pathogens, anaerobes, and enteric GNB was higher in the prosthetic hip infection than in the prosthetic knee infection. The high prevalence of MRS, including Methicillin-resistant (MR) S. aureus and MR-CoNS in PJI, may warrant the need for empiric antibiotic therapy with broader coverage while pending the culture result of PJI. Although fungal and mycobacterial PJI cases are rare, the incidence of these infections is relatively high in Taiwan. Fungus and mycobacterium should also be taken into consideration whenever a persistent PJI case is encountered.
Introduction
Prosthetic joint infection (PJI) is a devastating complication of joint arthroplasty, posing therapeutic challenges and causing enormous socioeconomic burden. 1 The incidence of PJI after hip or knee replacement is around 1–2%. 1,2 The number of primary and revision total joint arthroplasty is rapidly increasing in the aging population, and therefore, the number of PJI cases is expected to increase. 3
Different causative pathogens of PJI affect surgical outcomes. 4 –6 For example, methicillin-resistant Staphylococcus aureus (MRSA) PJI showed a higher risk of treatment failure and poorer prognosis. 4 In addition, a microbiological profile may vary among different geographical areas. 7 –9 Also, there are notable microbiological differences with regard to joint locations. 10 –12 For example, anaerobic microorganisms account for only 3–6% of all the PJIs, 13 but Propionibacterium acnes causes nearly a quarter of shoulder arthroplasty infections. 14 Furthermore, anaerobic bacteria are more commonly involved in hip PJI than in knee PJI. 11
To determine the appropriate empirical antibiotics and therapeutic strategies, it is important to understand the common microbiological causes of PJI. However, information on the comparison of different microorganisms involved in hip and knee PJI is limited. The aim of our study was to analyze the demographics and microbiological profile of PJI and to further compare the microbiological differences between hip and knee PJI.
Patients and methods
This is a retrospective cohort study of all cases of surgically treated hip and knee PJI at a referral medical center in Taiwan between January 2006 and December 2014. After approval by the institutional review board, the hospital electronic database was searched retrospectively for patients with the “International Classification of Diseases, Ninth Revision, Clinical Modification” code 996.66. Two independent researchers reviewed the extracted data and excluded patients with an infection after open reduction and internal fixation or primary septic arthritis.
PJI was defined by fulfilling one of the following criteria: (1) a sinus tract communicating with the prosthesis; (2) isolation of the same microorganism from two or more cultures obtained from an infected prosthetic joint; and (3) isolation in one intraoperative culture of microorganisms, plus evidence of infection at the site of hip or knee prosthesis (presence of purulence in an affected joint, elevated serum erythrocyte sedimentation rate and serum C-reactive protein level, elevated synovial white blood cell count and synovial neutrophil percentage or positive histological examination). 15
We recorded patient demographics, comorbidities, site of arthroplasty, time of infection, and causative pathogens. Based on the time to infection, PJI can be classified as early onset (occurring within 3 months after surgery), delayed onset (occurring from 3 months to 2 years after surgery), and late onset (occurring 2 years after surgery). 16 During the study, when there was more than one infection episode on the same joint, only the first episode was recorded. Polymicrobial PJI was defined as more than one microorganism isolated from one or more cultures of periprosthetic tissue or synovial fluid. The microbiological profile of all the infection cases was analyzed. In addition, the differences in the proportion of causative pathogens between hip PJI and knee PJI were compared.
Statistics
Fisher’s exact test was used to analyze categorical data. A p value less than 0.05 was considered statistically significant. All statistics were two-sided, and statistical analysis was performed using SPSS version 23.
Results
Demographics
A total of 294 first-time infection cases (159 hip PJIs and 135 knee PJIs) were included in the retrospective study from January 2006 to December 2014. The demographic characteristics of all patients are presented in Table 1. Four patients with hip PJI and three with knee PJI experienced bilateral joint infection. There were 108 male patients with hip PJI (70%) and 61 with knee PJI (46%). The hip PJI group had a higher male to female ratio of 2.3:1 and younger mean age of 60.8 years, whereas the knee PJI group had a male to female ratio of 0.86:1 and a mean age of 68.6 years (p < 0.001).
Demographics of hip and knee prosthetic joint infections.

aA p value of <0.05 was considered to be statistically significant.
The proportion of hypertension was higher in patients with knee PJI than those with hip PJI (65% vs. 43%; p < 0.001). By contrast, the incidence of alcoholism was higher in patients with hip PJI than those with knee PJI (14% vs. 5%; p = 0.01). There was no difference in the overall proportion of patients with hip PJI and knee PJI with regard to smoking, diabetes mellitus, hepatitis, chronic kidney disease, cirrhosis, or malignancy. More patients with hip PJI developed early-onset infections than those with knee PJI (27% vs. 16%; p = 0.03).
Microbiology
As shown in Table 2, a wide spectrum of causative microorganisms was identified in the 9-year study. The most common causative pathogen was S. aureus (78 cases, 26.5%), followed by coagulase-negative staphylococci (CoNS, 42 cases, 14.3%). Staphylococci had a high resistance rate to methicillin or oxacillin (Table 3). MRSA was isolated in 31 cases (10.5%) and methicillin-resistant CoNS (MR-CoNS) were isolated in 32 cases (10.9%). Up to 40% of S. aureus and 76% of CoNS were MR. Methicillin-resistant staphylococci (MRS) accounted for 21% of all PJIs.
Microorganisms in hip and knee PJI.

aA p value of <0.05 was considered to be statistically significant.
Methicillin resistance of staphylococcal PJI.
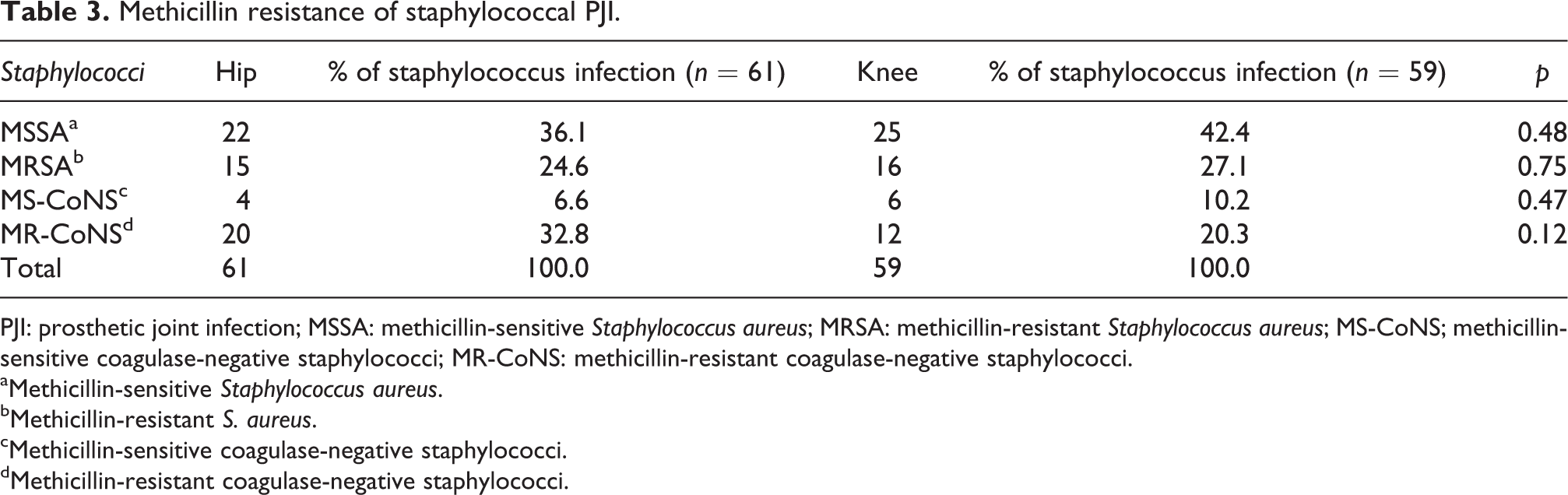
PJI: prosthetic joint infection; MSSA: methicillin-sensitive Staphylococcus aureus; MRSA: methicillin-resistant Staphylococcus aureus; MS-CoNS; methicillin-sensitive coagulase-negative staphylococci; MR-CoNS: methicillin-resistant coagulase-negative staphylococci.
aMethicillin-sensitive Staphylococcus aureus.
bMethicillin-resistant S. aureus.
cMethicillin-sensitive coagulase-negative staphylococci.
dMethicillin-resistant coagulase-negative staphylococci.
The distribution of causative microorganisms in hip and knee PJI revealed that in hip PJI, 43% were aerobic gram-positive, 7% anaerobes, 9% gram-negative, 2% fungus, 14% polymicrobial, and 25% negative culture; in knee PJI, 53% were aerobic gram-positive, 7% gram-negative, 2% fungus, 4% mycobacterium, 4% polymicrobial, and 30% negative culture. The proportion of causative microorganisms in hip PJI was higher than that in knee PJI (anaerobes: 11 vs. 0 cases, p = 0.002; polymicrobial pathogens: 22 vs. 6 cases, p = 0.01), while the proportion of mycobacterium in knee PJI was higher than that in hip PJI (0 vs. 5 cases; p = 0.01). The distribution of gram-positive, gram-negative, fungus, and negative culture between hip and knee PJI was not statistically different.
The causative microorganisms found in the polymicrobial infections are presented in Table 4. In hip polymicrobial PJIs, there were 17 cases (17/22, 77.2%) with 2 causative microorganisms, 1 case (1/22, 4.5%) with 3, 2 cases (2/22, 9.0%) with 4, and 2 cases (2/22, 9.0%) with 5. In knee polymicrobial PJIs, there were six cases (6/6, 100%) with two causative microorganisms. The most common combination of hip polymicrobial PJI was S. aureus with anaerobes including Peptostreptococcus sp., and enteric gram-negative bacilli (GNB) including Escherichia coli, Klebsiella pneumoniae, and Enterobacter species (7/22, 31.8%). Staphylococcus aureus with enterococcus or Corynebacterium species in knee polymicrobial PJIs accounted for two cases (2/6, 33.3%). Polymicrobial pathogens were more common in hip prostheses than in knee prosthesis (22 vs. 6 cases, p = 0.006).
Causative microorganisms in 28 cases of first-episode polymicrobial hip and knee PJI.

aA p value of <0.05 was considered to be statistically significant.
Anaerobic pathogens, including Propionibacterium species, Peptostreptococcus species, Prevotella species, and Parvimonas micra, were isolated in 11 cases (3.4%) in monomicrobial PJI (Table 2). In addition, as one of the causative microorganisms in polymicrobial PJI, anaerobic pathogens accounted for 10 isolates in 6 cases (2%), which was 27.3% (6 of 22) of the polymicrobial PJI (Table 4). All the above anaerobic pathogens were isolated in hip PJI. No anaerobic pathogens were found in knee PJI during the study. Anaerobic pathogens were more likely to involve in the hips than the knees in both monomicrobial infections (11 vs. 0 cases; p = 0.002) and polymicrobial infections (6 vs. 0 cases; p = 0.02).
Enteric GNB, including E. coli, Serratia marcens, K. pneumoniae, Enterobacter species, and Morganella morganii, were isolated as a single causative pathogen in 12 cases (7.5%) in hip PJIs and 5 cases (3.7%) in knee PJIs (12 vs. 5 cases; p = 0.16) (Table 5). Enteric GNB (including E. coli, K. pneumoniae, Enterobacter species, and Proteus vulgaris) were found frequently in polymicrobial infections, especially in the hip joint. It accounted for eight cases in hip polymicrobial PJIs (8 of 22, 36.4%) and one case in knee polymicrobial PJIs (1 of 6, 16.7%) (p = 0.03). Considering the total number of both monomicrobial and polymicrobial infections, enteric GNB were more commonly identified in hip PJI than in knee PJI (20 vs. 6 cases; p = 0.01).
Enteric gram-negative bacilli in 26 cases of first episode hip and knee PJI with single or multiple microorganisms.
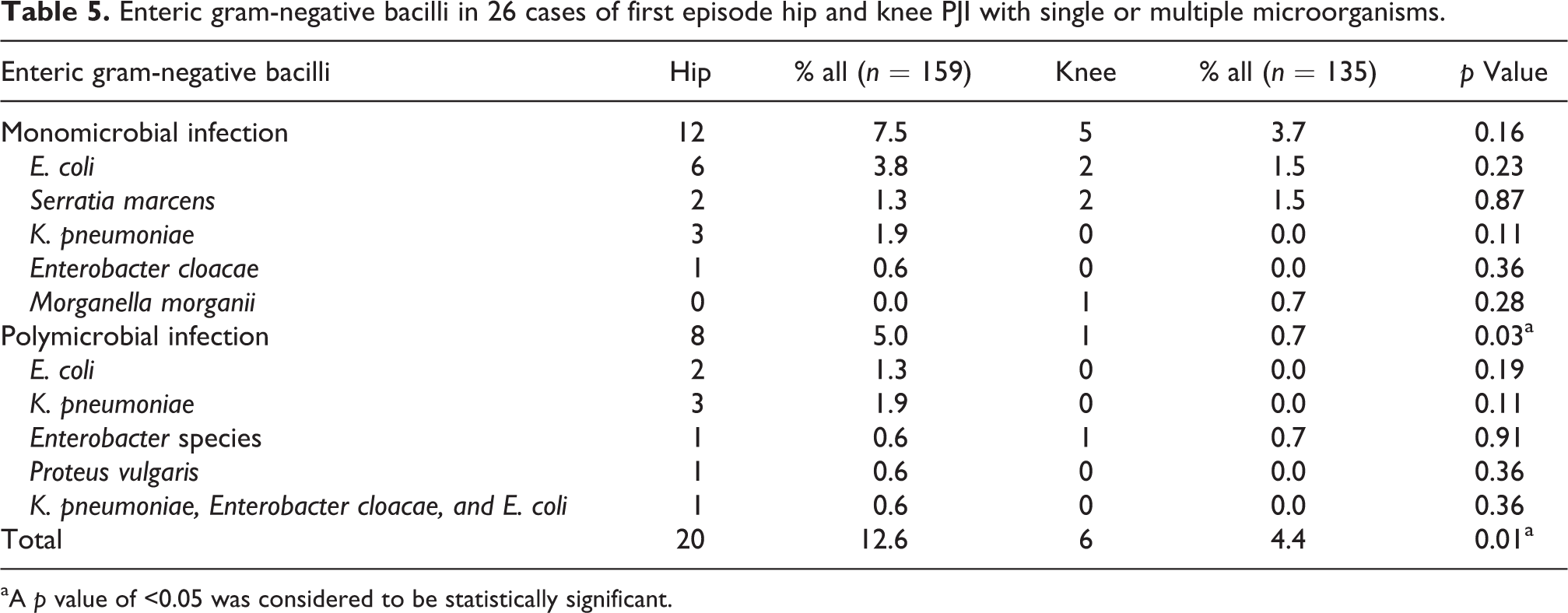
aA p value of <0.05 was considered to be statistically significant.
Fungal infections were found in four hip PJI cases (2.5%) and three knee PJI cases (2.2%) (p = 0.869). Among them, Candida species including Candida albicans, Candida parapsilosis, and Candida pelliculosa were found in five cases, accounting for 71% of all fungal infections. Two cases (0.7%) had a yeast-like fungal pathogen and no other specific species were identified.
Five cases (1.7%) of mycobacterial infections were found in the knee PJIs, including Mycobacterium tuberculosis, M. tuberculosis complex, and Mycobacterium fortuitum. Mycobacterium was not found in the hip PJIs (5 vs. 0 cases; p = 0.014).
Discussion
To our best knowledge, this study is the largest cohort study in the current literature to compare the microbiological differences between hip and knee PJI. 8,11,17 We found that MRS was prevalent in both the hip and knee PJI cases. The prevalence of causative microorganisms is different regarding the infected joint location. 10 Polymicrobial pathogens, anaerobes, and enteric GNB were more likely to occur in the hip prosthetic joint than in the knee prosthetic joint.
In the present study, S. aureus is the most common causative microorganism of PJI, which accounts for 26.5% of all cultures. The number of MRS in our study was high in which 40% of S. aureus and 76% of CoNS were MR. In total, they accounted for around one-fifth of all PJI cases. This was consistent with the generally high prevalence of MRSA and MR-CoNS in Taiwan. 18 Stefánsdóttir et al. also reported that the methicillin resistance among CoNS increased yearly, 7 and it was possibly due to the adaptive capability of CoNS. 19 Besides, MRSA PJI showed a higher risk of treatment failure. 4 Owing to the high prevalence of MRS, the finding reminds the treating physicians to select empiric antibiotics with broader coverage while awaiting the culture result of PJI.
The incidence of polymicrobial infections in the hip prostheses was statistically significant compared to that in the knee prostheses (22 vs. 6 cases, p = 0.006). This finding is consistent with previous literature. 11 Polymicrobial infections were most common among the early-onset infections. In this study, the incidence of polymicrobial infections involved in early-onset hip PJIs was up to 20.9%. Cobo et al. reported that the incidence of polymicrobial infections is as high as 32% in the early-onset infections 20 ; also, early-onset infections treated with debridement, antibiotics, irrigation, and retention have a higher success rate. However, polymicrobial PJI has been shown to be a prognostic factor for failure. 6 The frequency of gram-negative organisms was higher in polymicrobial PJI than that in monomicrobial PJI (50.0% vs. 8.2%). Gram-negative PJI resulted in a high rate of treatment failure, 5 which may explain why polymicrobial PJI led to poor outcomes. In the treatment of early-onset infections, especially in hip prostheses, a high incidence of polymicrobial infections should be considered.
Anaerobes and enteric GNB were found to be more common in hip PJI than in knee PJI. The incidence of anaerobic pathogens, including Propionibacterium species and Peptostreptococcus species, involving in hip PJI and knee PJI were 11 and 0 cases (p = 0.002). This finding is consistent with previous literature. 10 Propionibacterium acnes is also one of the most common causative pathogens in shoulder arthroplasty, and its proximity to the axilla is believed to be the reason. 14 The groin is rich in sebaceous glands as is the axilla, 21 hence, P. acnes tends to involve in hip PJI. Besides, Propionibacterium species and Peptostreptococcus species are part of the normal human gastrointestinal flora and, therefore, may easily cause direct contamination of the wound from the anogenital area during the hip arthroplasty surgery. 22,23 The unique features of the hip joint, including abundant sebaceous glands and proximity to the anogenital tract, may explain why anaerobe infections occur more frequently in hip prostheses than in knee prostheses.
For monomicrobial infections, we isolated enteric GNB including E. coli, Serratia marcens, K. pneumoniae, Enterobacter species, and Morganella morganii in 7.5% of the hip PJIs and 3.7% of the knee PJIs, respectively. Enteric GNB plays an important role in polymicrobial infections as well, especially in hip joints. 11 Our data showed that they were isolated in 36.4% of the hip polymicrobial PJIs but only 16.7% of the knee polymicrobial PJIs. The reason that enteric GNB is more common in hip PJI may be due to its proximity to the gastrointestinal tract with the colonization of enteric microorganisms around the hip and inguinal area. 17 A better prophylactic strategy such as using iodine-impregnated adhesive drape to prevent enteric GNB from entering surgical filed may help reduce enteric GNB PJI, especially in hip surgery. 24
Mycobacterium and fungus were the rare pathogens for PJI. Mycobacterial PJIs were only found in knee arthroplasties (5 vs. 0 cases, p = 0.02). Our study may result in a statistical error due to the small number of cases. Kofteridis et al. reported that 30 cases of mycobacterial PJI were found in English literature from 1966 to 2013. 25 Among them, 16 cases (53.3%) were total hip replacements and 14 cases (46.7%) were total knee arthroplasty. We also found mycobacterial PJI had a higher prevalence (1.7%) in our study than in the literature. Berbari et al. reported that PJI caused by M. tuberculosis in the developed countries was rare, accounting for only 0.3% of the 2116 PJI cases in a 22-year study. 26 Diagnosis of mycobacterial PJI may be delayed or even missed because of its infrequency. It is important to take mycobacterium into consideration whenever a persistent PJI case is encountered. 27 Fungal PJI occurred in seven cases (2.4%) of all PJI cases. Candida species were isolated in 71% of all fungal cases. The finding is consistent with prior studies that most fungal PJIs are caused by Candida species. The fungus is a rare pathogen for PJI and accounts for only approximately 1% of all PJIs. 28 The incidence of fungal PJI in this study was relatively high compared with those in previous studies. Kuiper et al. reported that in 21% of the patients with fungal PJI, the fungal culture results were incorrectly considered to be contamination. Therefore, if fungal species are cultured, they should always be treated as a pathogen. 29
This study has several limitations. Owing to its retrospective design, there is a certain collection bias. The medical treatment only cases were not included so data on patients infected by low-virulent pathogens may be missing. Only the causative microorganisms of the first episode were included. Additionally, the study was conducted at a single referral hospital, which may cause selection bias. Some patients underwent initial arthroplasty at outside institutions and received partial treatment for PJI there. Those who have undergone primary procedures at our hospital may have treatment for PJI elsewhere. The establishment of a national joint arthroplasty registry is necessary. Countries like Norway, Sweden, Australia, England, and New Zealand already have registries that help to conduct prospective and retrospective studies of PJI. 30 –33 Furthermore, the total negative culture rate was as high as 27.2% in this study. The main reason was the administration of antibiotic prior to obtaining culture samples. Most referral patients from outside institutions had received antibiotic treatment already and the antibiotics were not held for at least 2 weeks when the culture samples were obtained. Another reason was the limited culture samples, which were obtained at the time of surgery. In the early years of the study period, some cases might only have one swab culture sample. According to the current protocol at our department, we now collect a minimum of three tissue culture samples. We also aspirate the synovial fluid and inject it into the blood culture bottles. All the above strategies are used to improve the culture yield rate at our department. 34
Conclusion
We found that the prevalence of polymicrobial pathogens, anaerobe, and enteric GNB was higher in the prosthetic hip infection than in the prosthetic knee infection. The high prevalence of MRS, including MRSA and MR-CoNS in PJI, may warrant the need for empiric antibiotic therapy with broader coverage while pending the culture result of PJI. Although to our knowledge, fungal and mycobacterial PJI cases are rare, the incidence of these infections is relatively high in Taiwan. Fungus and mycobacterium should also be taken into consideration whenever a persistent PJI case is encountered.
Supplemental Material
supplementary - Different microbiological profiles between hip and knee prosthetic joint infections
supplementary for Different microbiological profiles between hip and knee prosthetic joint infections by Yifang Tsai, Chih-Hsiang Chang, Yu-Chih Lin, Sheng-Hsun Lee, Pang-Hsin Hsieh and Yuhan Chang in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.