
Abstract
Background and Aims:
Hemiarthroplasty is a common method of treating displaced femoral neck fractures, especially among elderly non-active patients with frailty syndrome. Complications arising from the use of a modern, modular hemiendoprosthesis via a posterior approach have been poorly reported in this population. The aim of this study was to evaluate complications and mortality associated with the use of Lubinus sp II cemented, unipolar hemiarthroplasty prosthesis and posterior approach during a 9-year follow-up.
Material and Methods:
All patients (244) who received hemiarthroplasty due to an acute fracture of the femoral neck in Central Finland Hospital, Jyvaskyla, Finland, during 2007 and 2008 were included. Patient records were retrospectively reviewed for intraoperative and postoperative complications.
Results and Conclusion:
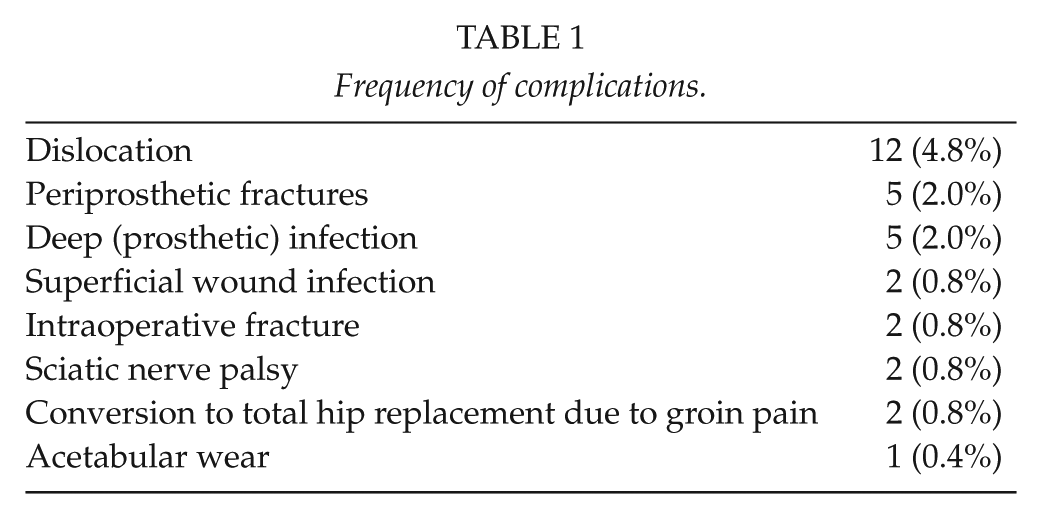
Women composed 70% (n = 171) of the study population. Mean age was 83 years for women and 80 years for men. A total of 31 (12%) complications were found in 30 patients. These were 12 dislocations (5% of all patients), 5 (2%) periprosthetic fractures, 2 (0.8%) superficial and 5 (2%) deep infections, 1 (0.4%) protrusion of the prosthesis, 2 (0.8%) intraoperative fractures, and 2 (0.8%) partial sciatic nerve palsies. Conversion to total hip replacement was performed in 9 cases (4%) and a reoperation was required in 15 (6%) cases. Mortality rate at 9 years was 78% (95% confidence interval = 72%–83%). The overall rate of complications was acceptable although mortality was high in this comorbid patient population. The need for conversion to total hip arthroplasty and reoperation is low.
Keywords
Introduction
Femoral neck fracture in the elderly is associated with high immediate and long-term postoperative mortality (1, 2). Management poses a challenge to the orthopedic community, since most of these patients are fragile with several comorbidities, such as cardiovascular diseases, cognitive impairment, and poor prefracture mobility (2, 3). Arthroplasty is the gold standard in the treatment of displaced femoral neck fractures. The relative superiority of hemiarthroplasty (HA) versus total hip replacement (THR) remains controversial. The external validity of the previous studies is limited, since a significant proportion of the true population undergoing surgery for femoral neck fracture, namely those with cognitive impairment and poor prefracture mobility, has been excluded from these studies (4, 5).
In Finland, HA is the most common method of treating displaced femoral neck fractures (6, 7). Much of the literature on the outcomes of HA concerns the uncemented Austin-Moore or cemented Thompson’s monoblock prostheses (Stryker UK Ltd, Newbury, United Kingdom). The literature (8–10) on complications using a modern, modular, cemented, unipolar hemiendoprosthesis via a posterior approach is sparse. Most of the literature (11–15) on complications with modern hemiendoprosthesis uses the Hardinge approach or does not differentiate between approaches.
The Lubinus sp II (Link, Hamburg, Germany) is a modular stem. It is possible to combine stems with different neck off-sets and angles for different head sizes. Modularity allows conversion to THR without stem removal. These properties are potential benefits when compared to monoblock prostheses. Superior results with modern modular hemiarthroplasties have been found when comparing with monoblock designs (11, 12). Modular stem design is hypothesized to reduce the risk of prosthetic dislocation.
The aim of this study was to review the complications and mortality associated with the use of the Lubinus sp II cemented, unipolar HA prosthesis via the posterior approach in the treatment of femoral neck fractures in non-selected, consecutive series of patients.
Materials and Methods
This study was performed in Central Finland Hospital (CFH), Jyväskylä, Finland. CFH is a public hospital providing traumatological treatment to a population of 250,000, which is approximately 5% of the country’s population. A retrospective review of all patients who underwent HA due to an acute fracture of the femoral neck in CFH between 1 January 2007 and 31 December 2008 was conducted.
In CFH, the treatment of acute intracapsular femoral neck fractures is based on the patient’s age, walking ability, comorbidities, and life expectancy. Young patients with minimally displaced fracture and high physical activity undergo closed reduction and internal fixation with cannulated screws. Elderly patients are more likely to undergo arthroplasty to mitigate the elevated risks in this population of fixation failure, nonunion, and avascular necrosis after reduction and internal fixation (16). Elderly patients with multiple medical comorbidities, physiologic compromise, cognitive impairment, and decreased functional demands are usually treated with HA. The Lubinus sp II prosthesis has been the primary fracture prosthesis in CFH since 2004. Younger patients with cognitive impairment or substance abuse may also be treated with HA to minimize the possibility of postoperative complications. Total hip arthroplasty (THA) is used in younger, healthy, active elderly persons with long life expectancy and no cognitive impairment or substance abuse.
All operations were performed using a cemented, modular, unipolar Lubinus sp II prosthesis and a third-generation cementing technique (washing the bone with pulsed lavage, use of an intra-medullary plug and retrograde insertion of the cement). All the hemiarthroplasties were planned with preoperative planning software. Patients were positioned in the lateral decubitus position and all operations were performed via the posterior approach. Cefuroxime (3 g intravenously) or, if cefuroxime was contraindicated, clindamycin (600 mg i.v.) was used as a single-dose antibacterial prophylaxis 30–60 min prior to incision. Tranexamic acid was used if preferred. The posterior capsule was repaired and the short external rotators were reattached. Subcutaneous injection of low-molecular-weight heparin (enoxaparin 40 mg once a day, started 6 h after the operation) was administered for antithrombotic prophylaxis in all patients for 4 weeks after surgery. Alternatively, previous warfarin treatment was continued as early as possible. Postoperatively, mobilization and weight bearing as tolerated were allowed immediately. Postoperative radiographs were taken on the first postoperative day.
Our electronic patient record system (Effica, Tieto corporation, Helsinki, Finland) was searched using a combination of the femoral neck fracture diagnosis code (ICD-10: S72.0) and surgical procedure code for cemented hemiendoprosthesis (NOMESCO code, Finnish version, NFB20). Patient files were reviewed in May 2016 in a search for intraoperative and postoperative complications (dislocation, periprosthetic fracture, superficial wound infection, prosthetic infection, acetabular wear, intraoperative fracture, sciatic nerve palsy, conversion to THR). All dislocations were diagnosed with a radiograph before and after closed reduction. Infection was classified as a deep infection if it required revision in OR. Sciatic nerve palsies were verified with an electromyoneurography (EMNG). Patient mortality data were obtained from the Population Register Centre. To obtain reference values for the mortality for this elder and fragile patient population, we retrieved mortality data for a reference cohort. The average age of the male patients was 80 years. Because our study period started in January 2007, we chose men born in 1927 and women born in 1924 as the reference cohorts. Statistics Finland (17) publishes statistics on the number of people living in Finland annually on December stratified by birth year. These data enabled us to calculate the overall mortality rate in the reference groups.
The mortality rate was analyzed using the Kaplan–Meier survival estimates. Survival estimates were reported for a minimum number of 20 at-risk patients. The cumulative incidence method with death as a competing risk was used to assess the revision-free survival estimates (18). Estimates were reported for a minimum of 20 at-risk patients. 95% confidence intervals (CIs) for the cumulative incidence estimates were based on the reported estimate ± 1.96 times the standard error obtained from the cumulative incidence function. Analyses were done using R statistical package v3.2.1 with the mstate and survival libraries (R foundation, Vienna, Austria).
Research permission was obtained from the healthcare district; no ethical permit was required.
Results
General Data and Demographics
In total, 244 patients with 250 hemiarthroplasties were identified. Median follow-up time in the patients who were alive on May 2016 was 8 years 6 months (7 years 5 months–9 years 5 months). There were 171 (70%) females with an average age of 83 years (47–101 years) and 73 (30%) males with an average age of 80 years (46–95 years). The operations were performed by 28 different surgeons. Residents performed 163 (65%) of the operations and orthopedic specialists 87 (35%). Median delay from hospitalization to surgery was 1 day (0–8 days).
Mortality
Ten (4%) patients died during the primary treatment period. According to the autopsies, four of these patients died of a pulmonary embolus. There were no verified fat-embolic events. Mortality rate at 9 years was 78% (95% CI, 72%–83%) (Fig. 1). After the increase in mortality during the immediate 30-day postoperative period, it leveled off and remained constant through the follow-up period. Fig. 2 shows mortality by gender compared to the reference population. After the immediate postoperative period, overall mortality did not differ from that in the reference population.
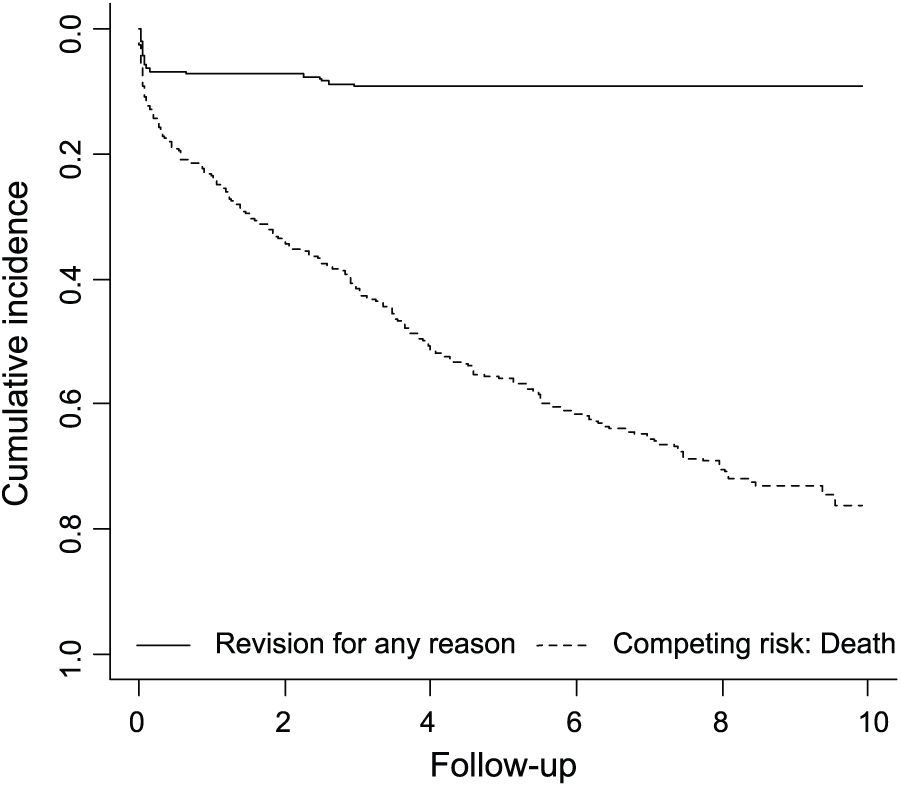
Cumulative incidence of revision for any reason and death as competing risk.
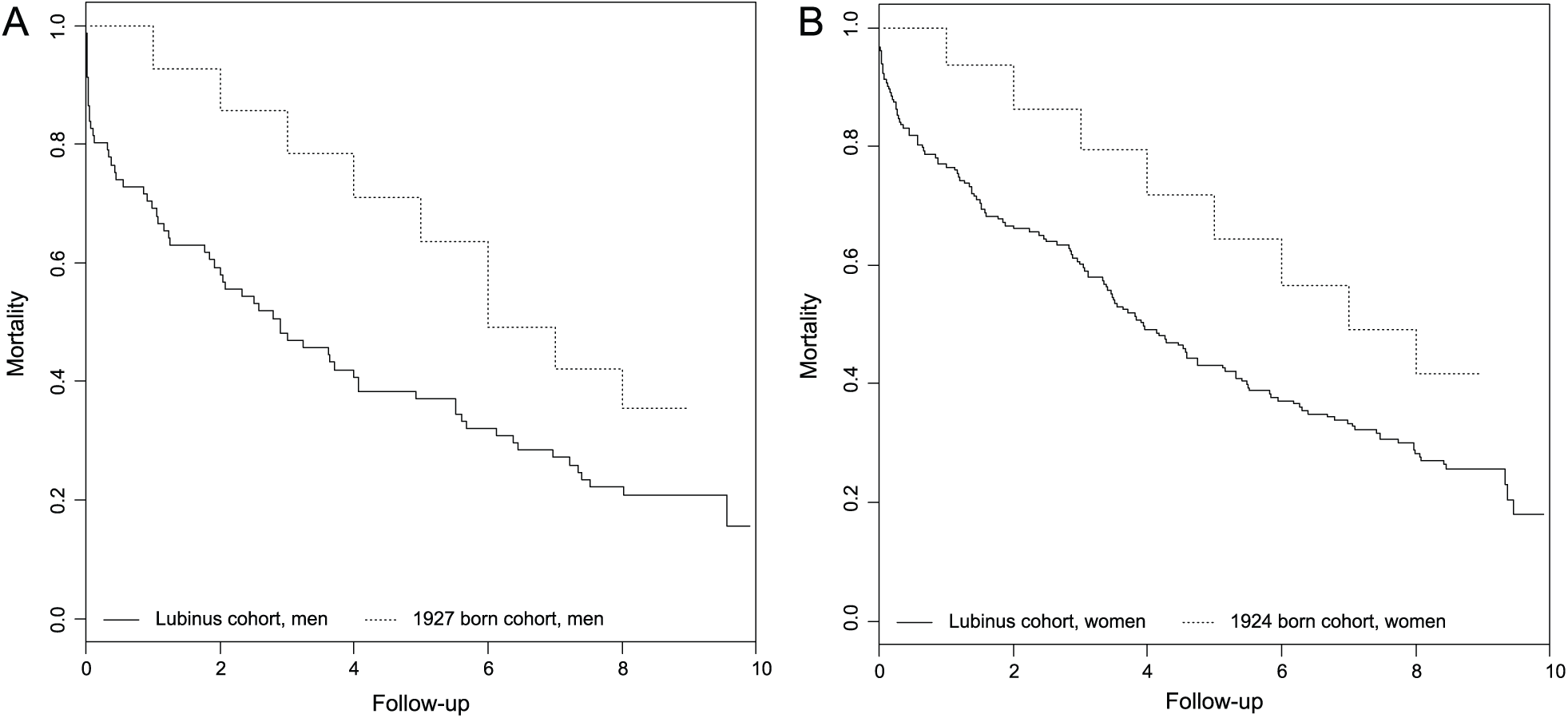
Comparison of mortality between our cohort and reference population stratified by gender: A) males and B) females.
Complications
During the first 9 years postoperatively, we found 31 (12%) complications in 30 patients (Table 1, Fig. 3). One patient first sustained a periprosthetic fracture (isolated greater trochanter fracture, Vancouver A) and subsequently a dislocation of the same hip. The mean age of the patients suffering complications was 76 years (range, 47–93 years; standard deviation (SD), 12).
Frequency of complications.
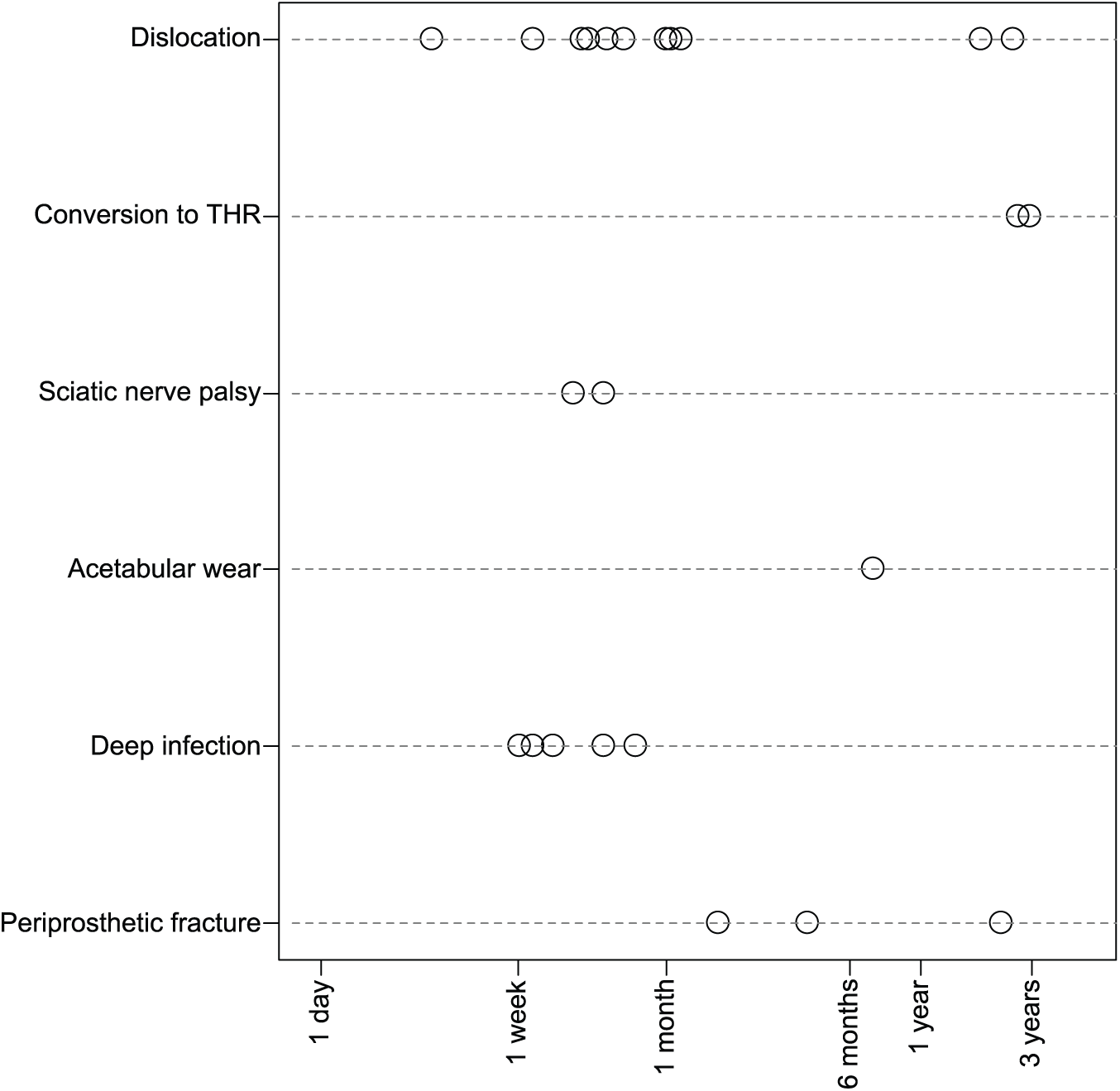
Time to complications during the 9-year follow-up, excluding intraoperative fractures and superficial infections.
A total of 12 patients (5%) had sustained a dislocation by the end of the follow-up period. The primary operating surgeon was a consultant in six of these cases and a surgical resident in the other six. No differences in prevalence (4% vs 7%, p = 0.3) were observed. Median time to the first dislocation was 19 days (range, 3 days–30 months 9 days). Closed reduction was successful in all cases. Of these 12 patients, five (2%) had recurrent dislocation of the same hip, on average 7 days after the first dislocation and had to undergo a reoperation (conversion to THR) due to recurrent dislocations. Late dislocation was rare. Dislocation-free survival remained constant after the immediate postoperative period (95% at 9 years, 95% CI: 93%–98%).
An intraoperative fracture occurred in two cases (0.8%): one patient had a fracture of the greater trochanter and was treated with osteosynthesis, and the other a fracture of the diaphysis of the femur, also treated with osteosynthesis. Up to the end of the follow-up period, postoperative periprosthetic fractures were observed in five patients (2%). Median time to fracture was 27 months (2 months–4 years 6 months). Two patients had a supracondylar fracture on the distal femur (Vancouver C) and both received locking plate surgery. Three patients had Vancouver A fractures (two greater trochanter fractures and one calcar fracture) and were treated non-operatively. All fractures were attributed to a fall.
Two patients (0.8%) had a superficial wound infection (11 and 38 days postoperatively). Both were treated successfully with peroral antibiotics with no need for reoperations.
A deep prosthetic infection occurred in five cases (2%). In these cases, senior consultants performed two and surgical residents three of the operations (2% vs 2%, p = 0.4). Median time to infection after the operation was 10 days (7–23 days). All five cases required revision surgery, and ultimately one was converted to THR using a two-stage revision strategy.
One case (0.4%) of acetabular wear (protrusion of the head of the prosthesis) was observed 7 months postoperatively and converted to THR. A further two patients (0.8%) complained of groin pain postoperatively. Both patients underwent conversion to THR. Partial sciatic nerve palsy (drop-foot) occurred in two cases (0.8%), observed 12 and 16 days postoperatively. Both cases of partial sciatic nerve palsies and both cases of intraoperative iatrogenic fractures occurred in cases operated by a surgical resident.
Conversion to THR after HA due to an acute fracture of the femoral neck had been performed in nine (4%) cases by the end of the follow-up period. A reoperation for any reason occurred in 15 cases (6%) during this time.
Overall Survival
Survival for 9 years with revision for any reason as end point was 95% (95% CI, 92%–98%). No late revision occurred after 3 years postoperatively (Figs 1 and 2).
Discussion
In this study, we report the complications associated with the use of cemented, modular, unipolar HA (Lubinus sp II) and the posterior approach for femoral neck fractures over 8-year follow-up. Given the challenges presented by the patient material, our level of complications is comparable with previous studies (8–10, 13–15, 19).
Displaced femoral neck fractures are a significant resource burden on the healthcare system and are associated with increased rates of morbidity and mortality (20). The reported incidence of hip fractures in Finland is approximately 131 per 100,000 person-years (21). In Finland, HA is the primary choice of treatment for a displaced femoral neck fracture in elderly patients, although THR may be considered in healthy and active patients. Approximately 2400 cemented hemiarthroplasties, which means an incidence of approximately 44 per 100,000 person-years, are performed annually to treat displaced femoral neck fractures (22). A large proportion of these operations are performed by young residents who do not yet have highly developed expertise in arthroplasty.
In the United Kingdom, the guidelines issued by the National Institute for Health and Care Excellence (NICE) recommend implant cementing over uncemented HA in displaced intracapsular femoral neck fracture (23). There is evidence that cementing the prosthesis in place reduces postoperative pain and leads to better mobility (24), and some evidence that cementing decreases the risk for reoperations when compared to uncemented HA (25). Lower incidence of intraoperative fractures with cemented HA has also been reported when compared to uncemented implants (26–28). The Hardinge approach is associated with less dislocation than the posterior approach (8, 14, 15). However, the Hardinge approach may be associated with a higher risk of damaging the superior gluteal nerve and limping (29–31). A study performed by Kristensen et al. (31) found less pain, better patient satisfaction, and better quality of life in patients operated with HA using the posterior approach than those operated using the Hardinge approach. However, superiority of the posterior and Hardinge approach regarding functional outcomes remains inconclusive (19, 29, 32, 33). Our study was limited by the fact that we did not quantify the subjective outcome.
In our study population, the most common complication was dislocation of the hemiendoprosthesis (4.8%). If the patient sustained more than one dislocation, it led to conversion to THR in all cases. In a study by Hedbeck et al., all the operating surgeons were orthopedic consultants and all operations were performed using the Hardinge approach. They reported a dislocation rate of 3.2% during 1-year follow-up after insertion of a modern, monopolar prosthesis. Patients with cognitive impairment were excluded, a criterion which is likely to reduce the risk for dislocation (14). This may be the smallest dislocation rate that can be achieved in optimal conditions. Our dislocation rate, in turn, is below average when compared to other studies using the posterior approach. In a study by Madanat et al. (10), using a LPP-EcoFit hemiendoprosthesis (cemented, modular, unipolar), all operations were performed using the posterior approach and the dislocation rate was 5.6%. Ninh et al. (8) found a dislocation rate of 5.7% when using the Hardinge approach and 6.4% with the posterior approach. The prosthesis used was Conquest FX Hip System (cemented, modular, unipolar). Yli-Kyyny et al. (15 and personal communication from Yli-Kyyny) found the dislocation rate of the Lubinus sp II hemiendoprosthesis (cemented, modular, unipolar) to be 9.0% using the posterior approach and 3.0% using the Hardinge approach. Similarly, Mukka et al. (19) found a dislocation rate of 8.4% with Lubinus sp II hemiendoprosthesis (cemented, modular, unipolar) when using the posterior approach. Kanto et al. (9) reported a 6.8% dislocation rate following insertion of the Lubinus sp II hemiendoprosthesis (cemented, modular, unipolar) using the posterior approach. In our study population, all the dislocations occurred during the first 3 postoperative years and especially during the first postoperative month. After the first 3 years, no dislocations occurred. This can partially be explained by the increasing mortality of this patient population during the long-term follow-up (Fig. 4).
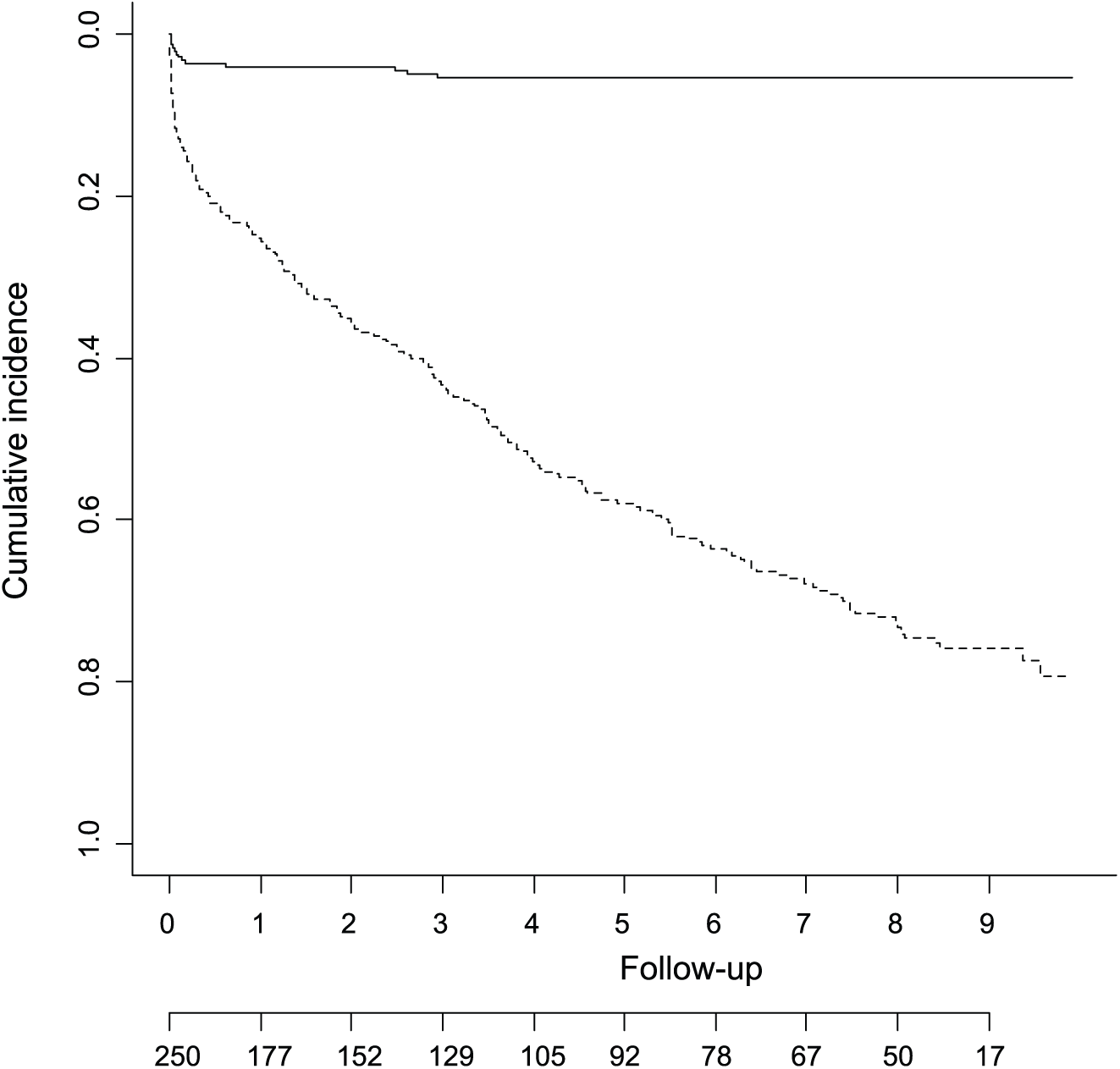
Cumulative incidence of dislocations (continuous line) with number of patients at risk reported and death as competing risk (dashed line).
In our study, superficial wound infections were very rare. This may be due to the fragility of these patients and due to the fact that minor complications like superficial infections are treated in primary healthcare centers, with only major complications being referred to specialized care. The number of deep (prosthetic) infections was acceptable (13, 15, 19). However, it is possible that late infections are underestimated because the most fragile patients may have been determined unfit for reoperation by a general practitioner and treated with suppression antibiotics in the healthcare centers without orthopedic consultation.
The number of periprosthetic fractures (2%) was also small and in line with a previous study reporting a periprosthetic fracture rate of 1.6% (15) using the same prosthesis. Kanto et al. (9), however, found no periprosthetic fractures when using the same prosthesis during an 8-year follow-up. The anatomical stem design of the Lubinus sp II stem is reported to have less periprosthetic fractures than wedge-type stems when using cemented hemiendoprosthesis in femoral neck fracture patients (34). The present rate of intraoperative fractures of 0.8% resembled the rates reported in previous studies (range, 0.8–3.7%) (13, 15, 35). Some of these studies performed both cemented and uncemented hemiarthroplasties, which may in part explain the higher rate of iatrogenic fractures. Cemented hemiendoprostheses have been found to have a lower risk of iatrogenic fracture than uncemented hemiendoprostheses (23, 26–28).
Although most of the present hemiarthroplasties were performed by surgical residents, their experience in performing this operation remains limited. The relatively low rate of complications found in this study could likely be further reduced through more structured education. A Danish study showed that in hip fracture surgery a systematic selection protocol and operations performed together with an orthopedic consultant reduced the revision rate from 18% to12%, but had no effect on the dislocation rate (36). In our hospital, preoperative planning software has been used in all operations since 2006. This potentially reduces the complication rate in particular the dislocation rate by helping surgeons to better restore an anatomic length and off-set. A study by Bjorgul et al. (37) demonstrated that residents reached the mean operating time of orthopedic surgeons after performing over 25 hemiarthroplasties. In our study, none of the residents performed this number of hemiarthroplasties during the 2-year study period. We found no difference in the dislocation rate or in the postoperative infection rate according to the surgical experience of the operating surgeon. Earlier studies have shown similar results for dislocation (10, 38, 39). In our study, all the intraoperative fractures and partial sciatic nerve palsies occurred during surgery performed by surgical residents. Three of these occurred during surgery by the same resident. These complications may result from technical errors by individual resident surgeons. In general, intraoperative fractures may be associated with the learning curve of the surgeon. An Australian study reported a 1.8% intraoperative iatrogenic fracture rate using a Thompson hemiendoprosthesis, with all the fractures occurring during surgery by surgical residents (35). The Lubinus sp II hemiendoprosthesis has an inbuilt anteversion; we speculate that this inbuilt anteversion could reduce the risk of dislocation and help an inexperienced surgeon in the correct positioning of the prosthesis. Considering the dislocation rate it might be safer for an inexperienced surgical resident to use the Hardinge approach.
The strengths of our study are that, according to our knowledge, no earlier study has reported on the complications of a modern, cemented, modular, unipolar HA performed via the posterior approach in an unselected patient population. Another strength is that all patients treated with hemiendoprosthesis for a femoral neck fracture in our hospital district catchment area were included. The operations were performed, using the same approach and stem, by a large number of different surgeons. This reflects normal clinical practice, and thus there is no inclusion bias. Our hospital is the only unit in our catchment area performing hip fracture surgery, and therefore it is unlikely that a significant number of complications would have been referred elsewhere. For these reasons, we believe that our study presents the true incidence of major complications especially those requiring surgical interference such as dislocations and periprosthetic fractures. In Finland, all deaths and causes of death are reliably recorded by Statistics Finland (40). The main weakness of the study is the retrospective setting. Acetabular wear may be underestimated in this study because apart from the immediate postoperative x-rays, no routine control x-rays were later obtained.
Conclusion
The complication rate (dislocations, periprosthetic and intraoperative fractures) of HA using a modern, modular, cemented stem via the posterior approach appeared to be at an acceptable level among a typical patient population with femoral neck fracture, namely elderly, non-active patients with frailty syndrome. The dislocation rate in our study, comprising of unselected patient material, is below average when compared to other studies using the posterior approach but higher than in studies using the Hardinge approach (33). The posterior approach is commonly used in Finland and considered acceptable according to the national Current Care Guideline for treatment of hip fractures (7). Our results on the complication rate must be, however, interpreted in light of the high mortality rate of 78% at 9 years. The risk for complications could potentially be further reduced by improving perioperative and postoperative care and rehabilitation of patients who sustain a fracture of the femoral neck. More systematic training of resident surgeons in HA could further reduce the complication risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.