
Abstract
Background:
Despite guidelines on blood transfusion (TF) thresholds, there seems to be great variation in transfusion policies between hospitals and surgeons. In order to improve and unify blood transfusion policies, the Finnish Red Cross Blood Service carried out a project concerning the optimal use of blood products (Verivalmisteiden optimaalinen käyttö) between 2002 and 2011. In this study, we determined the blood transfusion trends in major pancreatic surgery in Finland.
Methods:
Initially, 1337 patients who underwent major pancreatic resections between 2002 and 2011 were classified into the TF+ or TF− groups. Centers were divided into high-, medium-, and low-volume centers. The blood transfusion trends and the trigger points for blood transfusions in these patients were determined.
Results:
There were no differences between high-, medium- and low-volume centers in blood usage, trigger points or the use of reserved blood units after pancreatoduodenectomy or total pancreatectomy. However, the trigger points were lowered significantly during the study period at high-volume centers (p = 0.003), and a better use of reserved blood units was found in high- (p < 0.001) and medium-volume (p = 0.043) centers. In addition, a better use of reserved blood units was found in high-volume centers after distal pancreatectomy (p = 0.020)
Conclusion:
Although only minor changes in blood transfusion trends after pancreatoduodenectomy or total pancreatectomy were found generally, the lowering of the transfusion trigger point and the best use of reserved blood units during the study period occurred in high-volume centers.
Introduction
Various studies have shown a negative impact of perioperative blood transfusions in cancer patients (1–3). Although these studies may entail a bias known as confounding by indication (4), blood is a limited resource, and a risk of disease transmission still exists, especially in the developing countries. New guidelines on transfusion thresholds suggest a restrictive approach to blood transfusions (5). Despite these guidelines, there seems to be great variation in transfusion policies between hospitals and surgeons (6–8).
The Finnish Red Cross Blood Service (FRCBS) carried out a project concerning the optimal use of blood products entitled Verivalmisteiden optimaalinen käyttö (VOK) between 2002 and 2011. The underlying cause for carrying out the VOK project was a previous finding (9) that Finnish transfusion thresholds in all operations were liberal compared to recent international recommendations. In addition, significant interhospital variations in transfusion policies were detected between Finnish hospitals (10). The idea of the VOK project was to compare the use of blood transfusions between different hospitals and to form a national consensus on blood transfusion policies in Finland. The patient data came from pre-existing electronic medical registers. Each hospital district had contact personnel with whom a systematic audit of the data was performed. The hospital contact persons shared information on VOK data and attempted to influence the blood transfusion usage in their hospitals.
The VOK registry includes data on surgical procedures, diagnoses, laboratory results, and blood products. Based on this database, we determined the perioperative Hb levels, the use of blood transfusions, and the percentage of blood units used out of reserved blood units for 1337 patients who underwent major pancreatic resection.
In a recently published study by Ahola et al. (11), a better short- and long-term survival was found in patients who were operated on at high-volume centers. In addition, patients operated on at high-volume centers had reduced 90-day mortality (12).
The primary hypothesis was that the VOK project has lowered the Hb threshold levels that serve as the trigger point for blood transfusions and decreased the use of red blood cells while increasing the percentage of blood units used out of the reserved blood units. A secondary hypothesis was that high-volume hospitals are using less blood, have lower thresholds for transfusion, and use a higher percentage of the reserved blood units.
Materials and Methods
DATA
The FRCBS is the nationwide blood service provider in Finland. In 2002, the FRCBS established a joint registry (VOK) with Finnish hospital districts to collect blood usage data from potentially transfused inpatients. Eventually, five central and five university hospital districts submitted data to the registry. The registry was updated continuously between 2002 and 2011, but it was permanently dissolved in 2012 due to financial reasons. Hence, adding new data to the registry is not possible, although the collected registry data are still available for research purposes.
All patients with certain surgical procedure or diagnosis codes and all patients for whom a preoperative blood bank order was made were gathered into the database. The information in the database consists of patient characteristics, diagnoses, laboratory results, as well as statistics on surgical operations and blood products. The registry covered roughly 63% of all inpatient episodes and approximately 68% of all blood product usage in Finland. The data collection, the transfusion regimens, and the Hb measurement methods have been described previously (13).
For this study, we acquired the VOK registry data from the hospital districts. We queried the VOK registry for all patients who underwent pancreatoduodenectomy (PD), total pancreatectomy (TP), or distal pancreatectomy (DP) between 2002 and 2011. PDs and TPs were handled as one group based on the similar characters of the procedures.
The data were further categorized into patients who had been given at least one red blood cell transfusion during their inpatient episode (TF+) and those who received no transfusions (TF−). Data on the patients’ sex, age, and American Society of Anesthesiologists (ASA) class, as well as the status of the operation (emergency/elective), the length of the operation, the number of operations during the inpatient episode, the length of the hospital stay, the number of transfused blood units per patient, and the percentage of blood units used out of the reserved blood units, were collected. The trigger point for transfusion was defined as the lowest Hb value of the episode.
We divided the hospitals into high- (>20 PDs per year), medium- (6–19 PDs per year), and low-volume (<6 PDs per year) centers and compared blood usage between these centers. Only patients operated electively were included in these analyses.
Statistical Analyses
The Mann–Whitney U test and binomial test, when appropriate, were used for comparing measurements between TF+ and TF− patients (Tables 1 and 2) and to assess the effect of splenectomy with DP on blood transfusions.
Baseline demographic characteristics and surgical data for the study groups of patients who underwent total pancreatectomy or pancreatoduodenectomy.
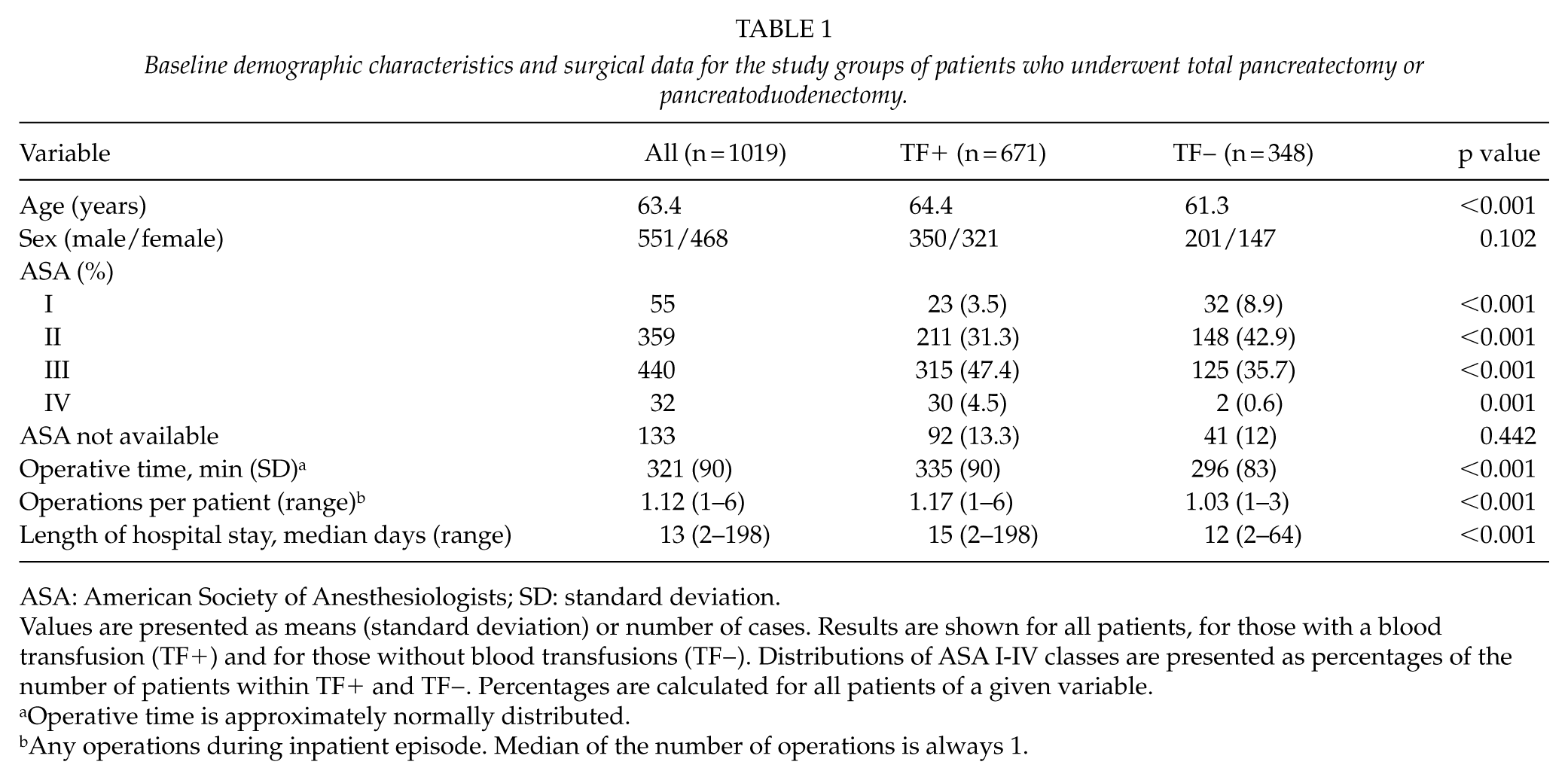
ASA: American Society of Anesthesiologists; SD: standard deviation.
Values are presented as means (standard deviation) or number of cases. Results are shown for all patients, for those with a blood transfusion (TF+) and for those without blood transfusions (TF−). Distributions of ASA I-IV classes are presented as percentages of the number of patients within TF+ and TF−. Percentages are calculated for all patients of a given variable.
Operative time is approximately normally distributed.
Any operations during inpatient episode. Median of the number of operations is always 1.
Baseline demographic characteristics and surgical data for the study groups of patients who underwent distal pancreatectomy.
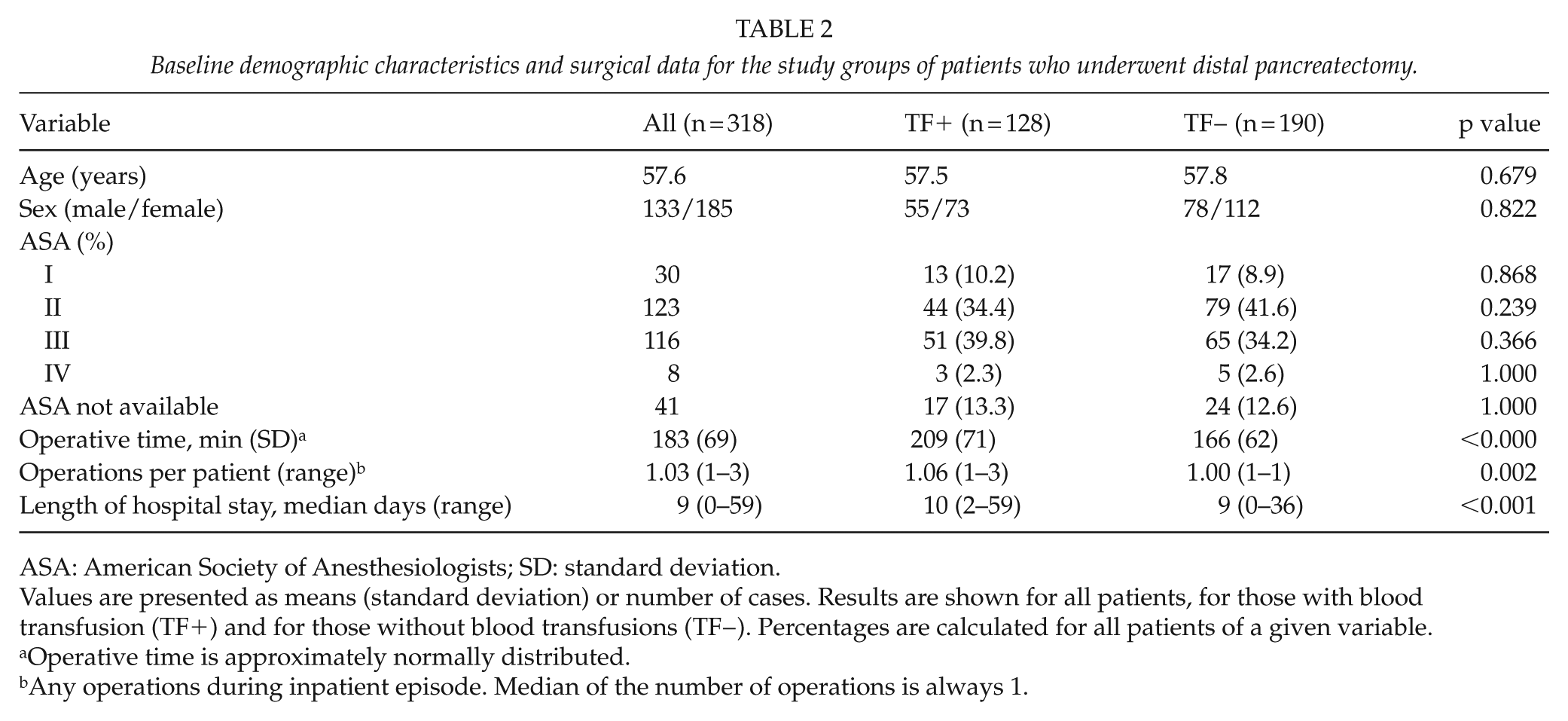
ASA: American Society of Anesthesiologists; SD: standard deviation.
Values are presented as means (standard deviation) or number of cases. Results are shown for all patients, for those with blood transfusion (TF+) and for those without blood transfusions (TF−). Percentages are calculated for all patients of a given variable.
Operative time is approximately normally distributed.
Any operations during inpatient episode. Median of the number of operations is always 1.
The linear trend tests presented in Tables 3 to 5 were performed using linear regression fitted to the yearly averaged data, with the year as a continuous predictor.
Mean red blood transfusion (RBT) units/patient between 2002 and 2011 among patients with total pancreatectomy (TP) or pancreatoduodenectomy (PD) and distal pancreatectomy (DP) in high-, medium-, and low-volume centers.
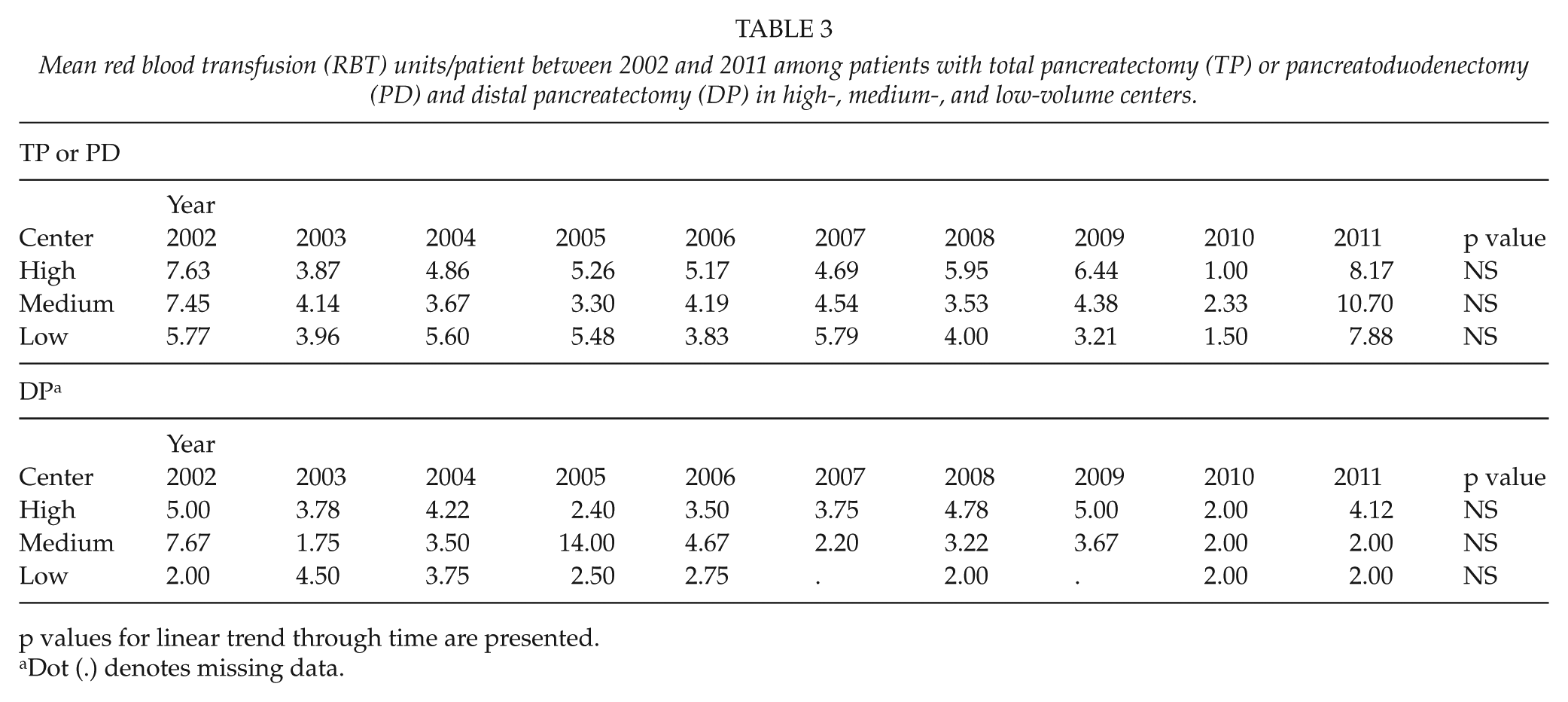
p values for linear trend through time are presented.
Dot (.) denotes missing data.
The mean trigger point (Trig) for blood transfusion between 2002 and 2011 among patients with total pancreatectomy or pancreatoduodenectomy (PD) and in distal pancreatectomy (DP) in high-, medium-, and low-volume centers.
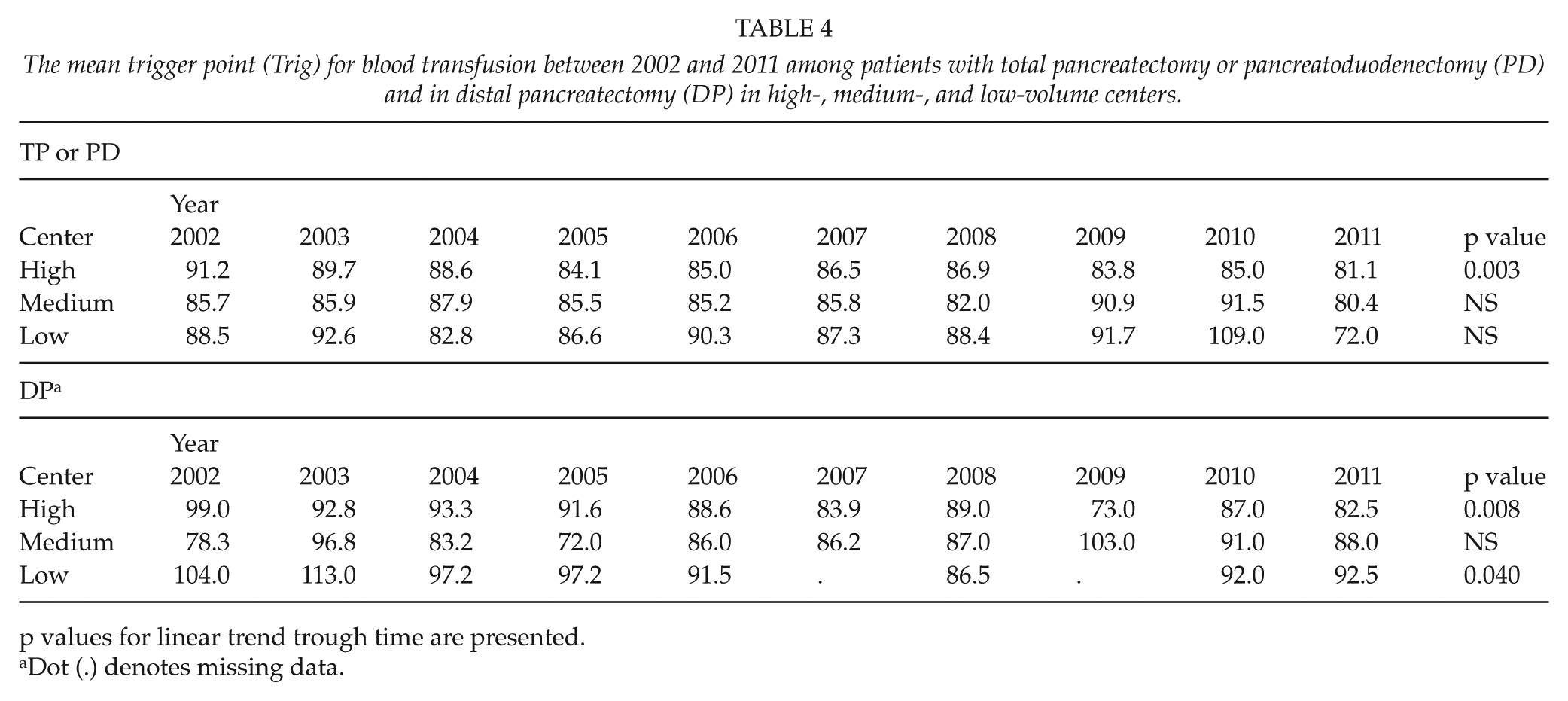
p values for linear trend trough time are presented.
Dot (.) denotes missing data.
The mean percentage of used red blood cell units out of reserved units (Res) between 2002 and 2011 among patients with total pancreatectomy or pancreatoduodenectomy (PD) and distal pancreatectomy (DP) in high-, medium-, and low-volume centers.
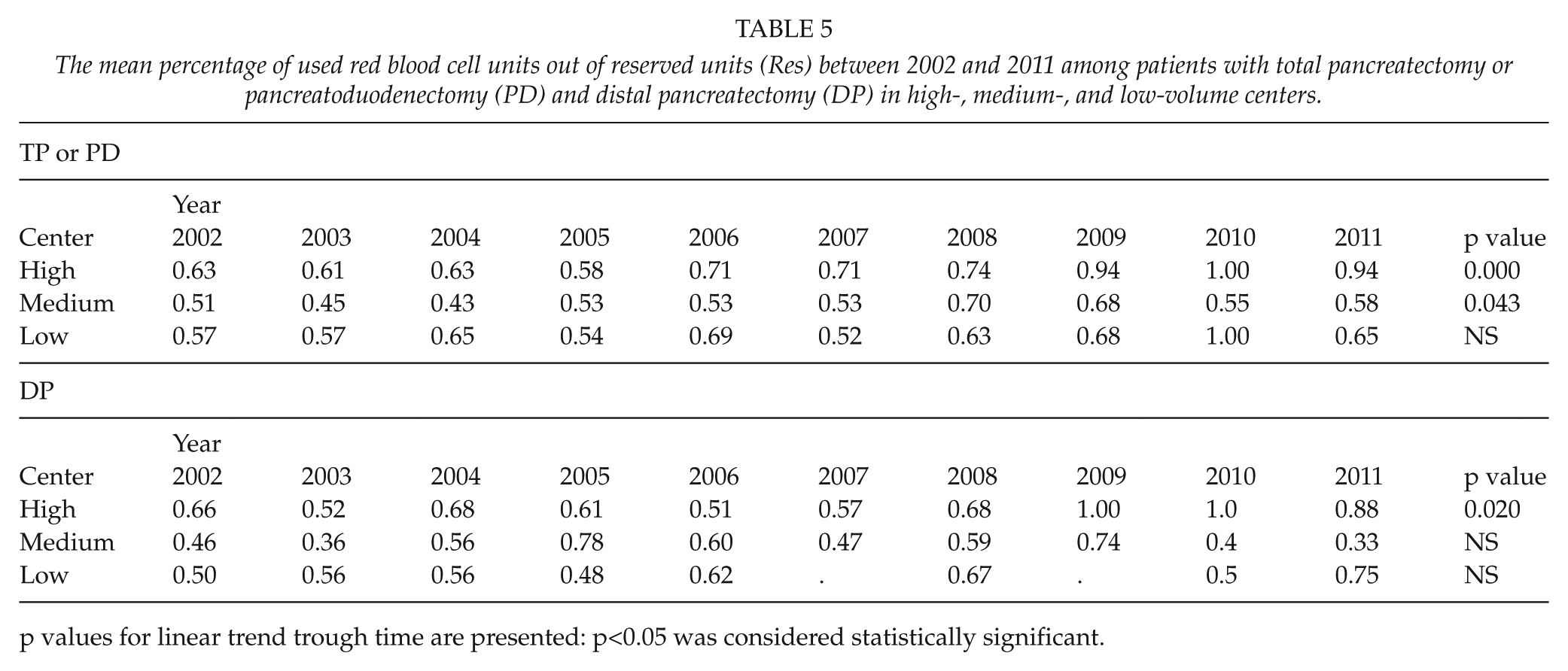
p values for linear trend trough time are presented: p<0.05 was considered statistically significant.
All statistical analyses were carried out using R software, version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria). The linear mixed models were fitted using the nlme add-on package in R (R package version 3.1-128). A level of p < 0.05 was considered statistically significant.
Ethics
The right to use the VOK registry in this study was acquired from the individual hospital districts that own the data, and from the national authority for health-related registry research (National Institute for Health and Welfare). In Finland, solely registry-based studies do not require a review by an (institutional) ethics committee. However, this study was approved by the ethics committee of Kuopio University Hospital.
Results
TP and PD
Our study cohort comprised 1043 TP and PD patients. Among 24 of the cases the operation was performed as an emergency setting and these were therefore excluded. The baseline demographic characteristics and surgical data of these 1019 patients are shown in Table 1. In brief, 671 (65.9%) of these patients received a TF. The TF+ patients were slightly older and had a higher ASA classification than the TF− patients. In addition, the operative times and inpatient episodes were longer among the TF+ patients. The TF+ patients underwent a higher number of operations during the inpatient episodes.
The mean number of red blood transfusion units was 5.22/patient (1.9–8.76). The mean trigger point for blood transfusion was an Hb level of 86.5 g/L (range 78.5–89.9). The mean percentage of blood units used out of the reserved red blood was 63.4% (56%–80%).
The comparison of blood usage between high-, medium-, and low-volume centers is shown in Tables 3 to 6.
The mean percentage of those patients who received TF between 2002 and 2011 among patients with total pancreatectomy or pancreatoduodenectomy (PD) and distal pancreatectomy (DP) in high-, medium-, and low-volume centers.
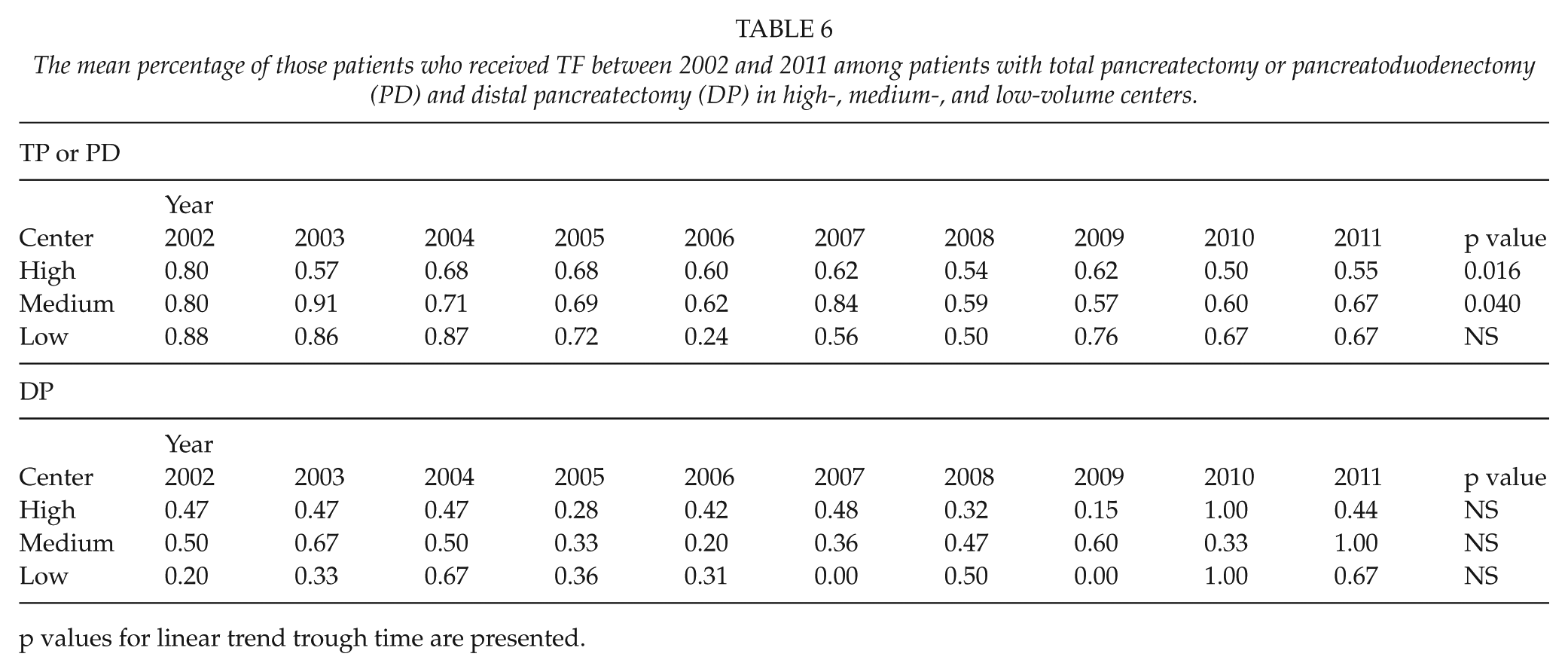
p values for linear trend trough time are presented.
Using the same criteria as a previously reported study (11), two of our study hospitals were high-, four medium-, and four low-volume centers.
There were no differences between high-, medium-, and low-volume centers in blood transfusion usage, trigger points, or the use of reserved blood units after PD or TP. However, the trigger point was lowered significantly during the study period at high-volume centers (p = 0.003), and a trend toward a better use of reserved blood units was found in high- (p < 0.001) and medium-volume (p = 0.04) centers. In addition, the percentage of those patients who received a TF decreased in high- (p = 0.016) and medium-volume centers (p = 0.0).
DP
Out of the 361 DP patients, 158 (43.8%) were transfused. Of the DP procedures, 43 were performed in an emergency setting and were therefore excluded. In one case, the type of procedure was not available. Out of these 318 electively operated patients, 128 (40.3%) received blood transfusions. The operative time and the duration of the inpatient episode were longer in the TF+ group (Table 2).
The mean number of red blood transfusion units was 3.7/patient (3.5–10). The mean trigger point for blood transfusion was an Hb level of 89.6 g/L (82.5–92.8). The mean percentage of blood that was used out of the reserved blood was 60.3% (53%–81%) (Table 3).
Out of the 318 DP patients, splenectomy was also performed on 98 patients (31%). There were no differences in the number of blood transfusions between these patients. All DPs during the study period were performed with an open technique.
The comparison of blood usage between high-, medium-, and low-volume centers is shown in Tables 2 to 5.
According to a previously reported study (11), two of our study hospitals were high-, four medium-, and four low-volume centers.
A better use of reserved blood units after DP was found in high-volume (p = 0.020) centers.
Discussion
In contrast to our primary hypothesis, only minor changes were found in TF policies in Finland during the study period. The trigger point for TF after PD or TP was lowered only in high-volume centers, and the percentage of blood used out of the reserved blood increased more in high-volume centers than in medium-volume centers. In low-volume centers, no changes were found in the TF processes after PD or TP. Our findings support the secondary hypothesis that the TF process is functioning better in high-volume centers, although no differences were found in the number of blood units transfused between different centers.
In Finland, the transfusion thresholds in common elective surgical procedures were liberal compared to international recommendations (9), and the largely inappropriate thresholds were reflected in the high transfusion rates. Previously, the introduction of a new hospital policy for red cell transfusions, including an Hb concentration trigger point of <80 g/L, diminished the proportion of patients transfused in coronary artery bypass graft and total hip replacement operations, but not in colectomies (14). Tinmouth et al. (15) reviewed behavioral interventions and found them to be effective in changing physicians’ transfusion practices and reducing blood utilization. In this review, a variety of techniques were used, including guidelines, an audit with feedback, an audit with approval, a new transfusion form, and education. All of these interventions, used either as a single method or in combination with each other, were found to be effective.
In the VOK project, the method of intervention mostly used was education. Due to the retrospective nature of this study, it is difficult to determine whether the changes observed are related to the VOK or whether they are due to international influence among surgeons who have attended various international courses and meetings. Most of the changes observed in the VOK project were found in high-volume centers, supporting the role of international influence in these changes. During this study period, the centralization of PD or TP procedures had not been implemented in Finland. However, the centralization of major pancreatic surgery is currently in progress, which may diminish the need for TFs. Other possible solutions for a better use of blood products in major pancreatic resections are a new transfusion form and national education, which have previously been effective methods in diminishing the use of blood products (15). Finally, the type and screen method, with the aid of which blood is received in a much shorter time than previously, can decrease the use of blood products. During this study period, the type and screen method was not used in the study hospitals.
Previously, it has been found that Hb levels employed to trigger a TF varied for different reasons, and especially older patients and patients with multiple comorbidities were at an increased risk of an intraoperative blood transfusion (16). This is partly in accordance with our results, since we found that TF+ patients transfused after PD and TP were older and had a higher ASA classification.
New guidelines (17) suggest a restrictive approach to TF. A restrictive TF trigger does not carry an increased risk of complications in major gastrointestinal surgery (18, 19). We found a longer hospital stay among TF+ patients in all patient groups. However, as stated before, our results, including the longer hospital stay after a TF, may carry a bias known as confounding by indication (4). Our study was not designed to establish differences in complications between TF− and TF+ patients. Our TF figures are quite high, reflecting a liberal transfusion policy in Finland, as has been stated before (13).
The main limitation of our study is that the registry-based setting does not allow us to analyze all possible interesting aspects. For example, the assessment of the patient’s condition before the operation is rather limited, mainly consisting of the ASA classification only. In addition, any possible neoadjuvant chemoradiation therapy and the use of any medication affecting Hb could not be checked. Furthermore, adding new data to the registry is not possible because the registry was formally dissolved “as is.” However, we have a good coverage of the surgical procedures performed in Finland, and we also have suitably detailed information about the blood transfusions.
In conclusion, only minor general changes in blood transfusion trends after PD or TP were found. However, Hb levels used as transfusion trigger points decreased and the best use of reserved blood units during the study period occurred in high-volume centers.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the research foundation of Kuopio University Hospital and the EVO funding of the Hospital District of South Ostrobothnia.