
Abstract
Background and Aims:
The risk of synchronous and metachronous colorectal cancer is influenced by heritable and environmental factors. As a basis for comparative studies, we provide population-based estimates of synchronous and metachronous colorectal cancer with a focus on non-heritable cases.
Material and Methods:
Based on data from national Danish cancer registers, we estimated the proportion of synchronous colorectal cancer and the incidence rates and risks for metachronous colorectal cancer in 28,504 individuals, who developed 577 metachronous colorectal cancer above age 50.
Results:
Synchronous colorectal cancer was diagnosed in 1.3% of the cases. The risk of metachronous colorectal cancer was associated with sex, tumor location, and age with the strongest influence from the latter. The incidence rate ratios for metachronous colorectal cancer ranged from above 6 in patients below age 65 to <1–3.2 in patients above age 65. The absolute risk of metachronous colorectal cancer was ⩾10% in patients below age 65 and 1.0%–8.0% in patients above age 65.
Conclusion:
Individuals who develop sporadic, non-inherited colorectal cancer above age 50 are at a significantly increased risk of metachronous colorectal cancer with risk estimates that are strongly affected by age. This observation underscores the need for development of targeted surveillance in the most common clinical subset of colorectal cancer.
Keywords
Introduction
Growing populations, increasing life expectancy, and influences from lifestyle factors contribute to an increasing disease burden from colorectal cancer (CRC) with a current estimate of 1.4 million patients diagnosed annually worldwide. Screening and surveillance contribute to decreasing rates in the United States and New Zealand, whereas increasing incidences are experienced in Eastern Europe, Asia, and Latin America (1). Following development of CRC, an increased risk of metachronous colorectal cancer (MCRC) has consistently been demonstrated with standardized incidence ratios of 1.4–2.2 (2–9). Genetic predisposition and environmental factors such as inflammation and exposure to tobacco and alcohol are the major risk factors, although their individual contribution is uncertain (9, 10).
Multiple primary tumors represent a characteristic of hereditary cancer syndromes and a standardized incidence ratio of 1.9 for the development of MCRC has been identified in individuals with a family history of CRC (9). Early age at onset and defective mismatch-repair, both of which are hallmarks of heredity, have consequently been associated with an increased risk of MCRC (2, 5, 11–13). Among the hereditary subsets, an increased risk of MCRC has been documented in Lynch syndrome, in familial adenomatous polyposis (FAP) and in the serrated adenoma syndrome with cumulative risk estimates of 19%–50% at 10–20 years (11). Risk estimates of MCRC are generally based on mixed cohorts, which imply a contribution from early-onset cases and familial and hereditary predispositions. In order to provide robust risk estimates for the most common clinical subset, that is, sporadic cases diagnosed above age 50, we determine incidence rates (IRs), incidence rate ratios (IRRs), and absolute risks of first CRC and MCRC in this cohort using population-based data from Denmark.
Materials And Methods
Data Sources
In Denmark, unique personal identification numbers allow for linkage between different population-based registers since 1968. The Central Population Registry (CPR) contains 99.7% complete data on birth, death, and emigration (14). The population-based Danish National Cancer Register (DNCR) contains data on all malignancies diagnosed since 1943 based on ICD7/ICD10 codes with 98% completeness (15). According to Danish guidelines, carcinomas in situ are not classified as malignancies and thus neither reported to the DNCR nor included in the study. The National Patient Register (NPR) contains information on diagnoses and treatments since 1977 at hospitals in Denmark. The Danish hereditary CRC registers, that is, the hereditary non-polyposis colorectal cancer (HNPCC) register and the FAP register, were established in 1991 and 1971, respectively, and contain national data on all identified individuals suspected or verified to be at risk of hereditary CRC based on family history and/or genetic diagnostics (16, 17). At the time of the study, the HNPCC register contained 4198 families (50,630 individuals) and the FAP register contained 218 families (691 individuals).
Patients
The study design with included and excluded patient subsets is presented in a Lexis diagram (Fig. 1). Herein, area A represents the study period, area B shows the time used to discriminate first CRC from MCRC, area C includes all patients diagnosed with CRC before age 50, areas D-E include birth-cohorts without time at risk, area F is right-censoring of individuals above age 90, and area G represents a period with lack of data. All CRCs diagnosed in Denmark between 1943 and 2012 were retrieved from the DNCR. Data from 1943 to 2007 were used for exclusion and to classify events as first CRC or MCRC. Data from 2008 to 2012 were used for risk calculations in patients aged 50–89 during the time period (Fig. 1, area A). Individuals with CRC diagnosed before age 50 were excluded as were individuals with suspected or verified hereditary predisposition based on the HNPCC register and the FAP register. Population size and mortality rates retrieved from Statistics Denmark were used to calculate the IR of first CRC and the absolute risk of first CRC and MCRC. Person years at risk (PYRS) were calculated from 1 year after diagnosis of the first CRC until death, end of study, proctocolectomy, first MCRC, or loss to follow-up, whichever came first. Vital status and date of death, emigration, or loss to follow-up was retrieved from the CPR.
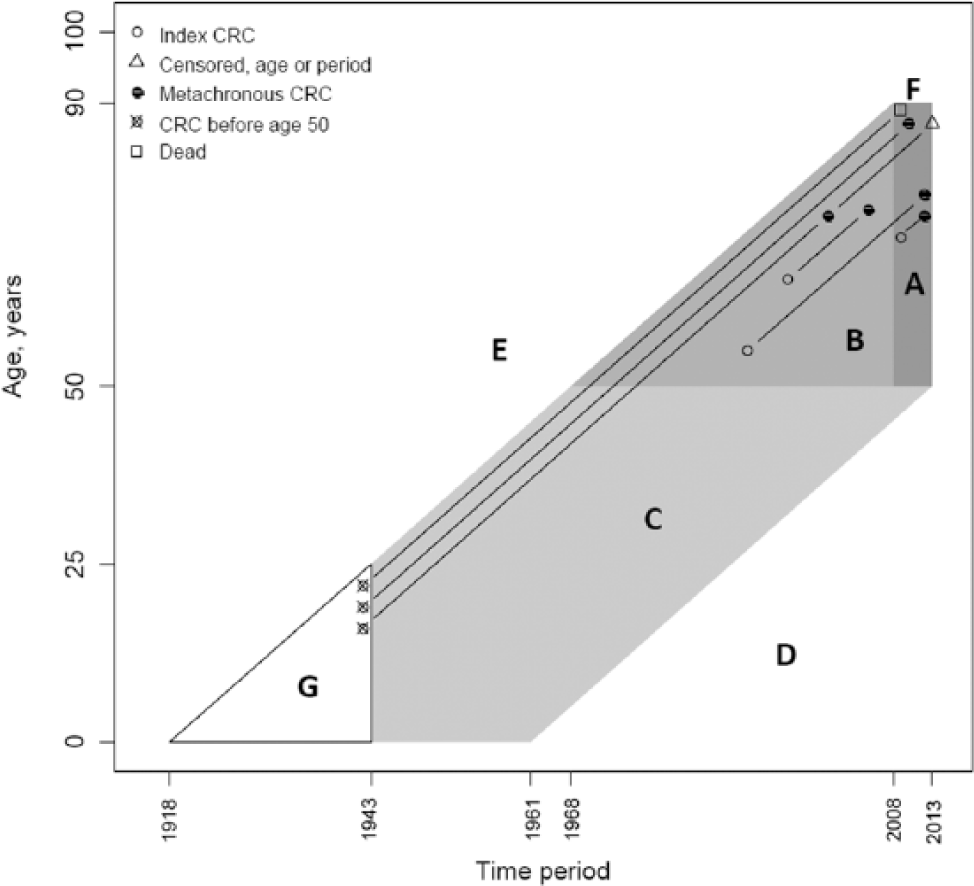
Lexis diagram describing study design. Area A represents the study period and ages. Area B was used to discriminate first colorectal cancer (CRC) from metachronous (MCRC) and to exclude patients without risk of first MCRC in area A. Area C was used to exclude patients diagnosed with CRC before age 50. Areas D and E were used to exclude patients from birth-cohorts without time at risk in area A. Area F was used to right-censor individuals who reached age 90. Area G represents individuals where lack of data could cause misclassification of first CRC versus MCRC. In total, patients (n = 190,005) with CRCs (n = 193,599) were retrieved. We excluded synchronous first CRCs (n = 1034) and patients (n = 7988) who were at risk of hereditary cancer and who had developed (n = 8331) CRCs. Area A—Patients (n = 17,473) aged 50–89 with their first CRC. Of these, n = 10,372 patients became at risk of MCRC. In total, 7101 individuals were excluded from calculations regarding MCRC because of proctocolectomy (n = 94) or <1-year follow-up due to death (n = 3931), emigration (n = 4), or end of study (n = 3072). A total of 28,504 patients were at risk of MCRC (consisting of 10,372 individuals from area A and 18,132 patients from area B). Herein, a total of 577 MCRC were diagnosed, 7355 patients died, and 20,572 were censored (because of age ⩾90 years (n = 1566), emigration (n = 23), loss to follow-up (n = 2), or end of study (n = 18,981)). Follow-up was stopped at the time of an event, thus censoring n = 10 second MCRCs. Area B—Patients (n = 52,811) with CRCs (n = 53,319). Exclusion was based on patients with MCRC before the study period (n = 501 patients with n = 1015 CRCs), proctocolectomy (n = 196), death (n = 33,607), emigration (n = 38), loss to follow-up (n = 2), and observation time <1 year (n = 335). The remaining patients (n = 18,132) continued to area A in risk of MCRC. Area C—Patients (n = 5622) with CRCs (n = 5758) excluded because of diagnosis <50 years of age. Of these, n = 25 patients were diagnosed <25 years of age (0.03% of patients in area A, B, and C). Area D—Patients (n = 1028) with CRC (n = 1038) not at risk because of low age. Area E—Patients (n = 104,046) with CRC (n = 104,970) not at risk in area A because of high age. Area F—Cases with first CRCs (n = 979) and MCRC (n = 45) diagnosed ⩾90 years of age. Area G represents lack of data with a potential inclusion only if the patients had survived a first CRC by >65 years and not excluded in any of other areas.
Synchronous first CRCs were defined as a new CRC diagnosed within 1 year after the first CRC and were, together with patients with a suspected or verified hereditary predisposition, excluded from the study. Furthermore, patients not at risk during the study period (Fig. 1, areas B, C, and F) and patients from birth-cohorts outside of the target age, that is, <50 or > 90 years during the study period (Fig. 1, areas D and E) were excluded. Tumor location was classified as cecum, ascending colon, hepatic flexure, transverse colon, splenic flexure, descending colon, sigmoid colon, and rectum. MCRCs were defined as new primary CRCs more than 1 year after the first CRC. Data on the type of surgery were obtained from the NPR from 1977 to 2012. Segmental resections were classified according to segment. Type of surgery was, if not otherwise specified, assumed to be segmental resection and patients, who had undergone proctocolectomy, were considered not to be at risk of MCRC. In the affected population, our estimate can be interpreted as the risk of MCRC from an attained age given the patient is cured of the first CRC.
Statistics
The IRs for first CRC and MCRC were calculated in the general population and IRRs were calculated in groups defined by age and sex. Furthermore, IRs for MCRC were stratified by the site of the first CRC and were analyzed using Poisson regression that included time at risk for each stratum as an offset. The absolute risks of first CRC and MCRC were estimated in relation to sex and attained age with death as a competing risk using general population mortality rates. Probabilities for each of the three outcomes death, CRC/MCRC, or entering the next age group were calculated for each 5-year age group from 50 to 89 years of age. Probabilities were calculated from incidence and mortality rates using standard formulas for the Poisson distribution. In the general population, absolute risks for attained ages were calculated backward through age using actuarial principles to estimate the risk of CRC before age 90 or death. Data management was performed using SAS 9.4 and all analyses were made in R-3.3.3 (18).
Results
The study period was defined as 2008–2012. In order to classify cases that occurred herein as first CRC or MCRC, all 193,599 CRCs diagnosed in 190,005 patients during 1943–2012 were retrieved (Fig. 1). During the study period (Fig. 1, area A), 17,473 individuals developed a first CRC of which 10,372 contributed with time at risk of MCRC (following 1 year of follow-up). In addition, 18,132 patients developed a first CRC prior to the study period and remained at risk during the study period (Fig. 1, area B). Hence, 28,504 individuals were at risk, of whom 577 developed MCRC, 7355 died, and 20,572 were censored because of age, emigration, loss to follow-up, or end of study.
Events, PYRS, IRs, IRRs, and absolute risks are presented in Table 1. IRs and IRRs for first CRC and MCRC are shown in Fig. 2. The IRs for first CRC increased with age and were significantly higher in men compared to women in the age groups 65–89 years (0.0001 < p < 0.005). Sex had a minor impact on the IR of MCRC, which was higher in men than in women only in the youngest age group (p = 0.049). The overall IRRs of MCRC compared to first CRC were 3.49 in men and 3.92 in women with a strong and inverse correlation with age with IRRs >6 for both sexes below age 65 (Table 1). The absolute risk estimates of MCRC ranged from 0.8% to 22.2% and were inversely correlated with age (Fig. 3).
Incidence rates and relative risks of primary and metachronous colorectal cancer in relation to sex and age, respectively.
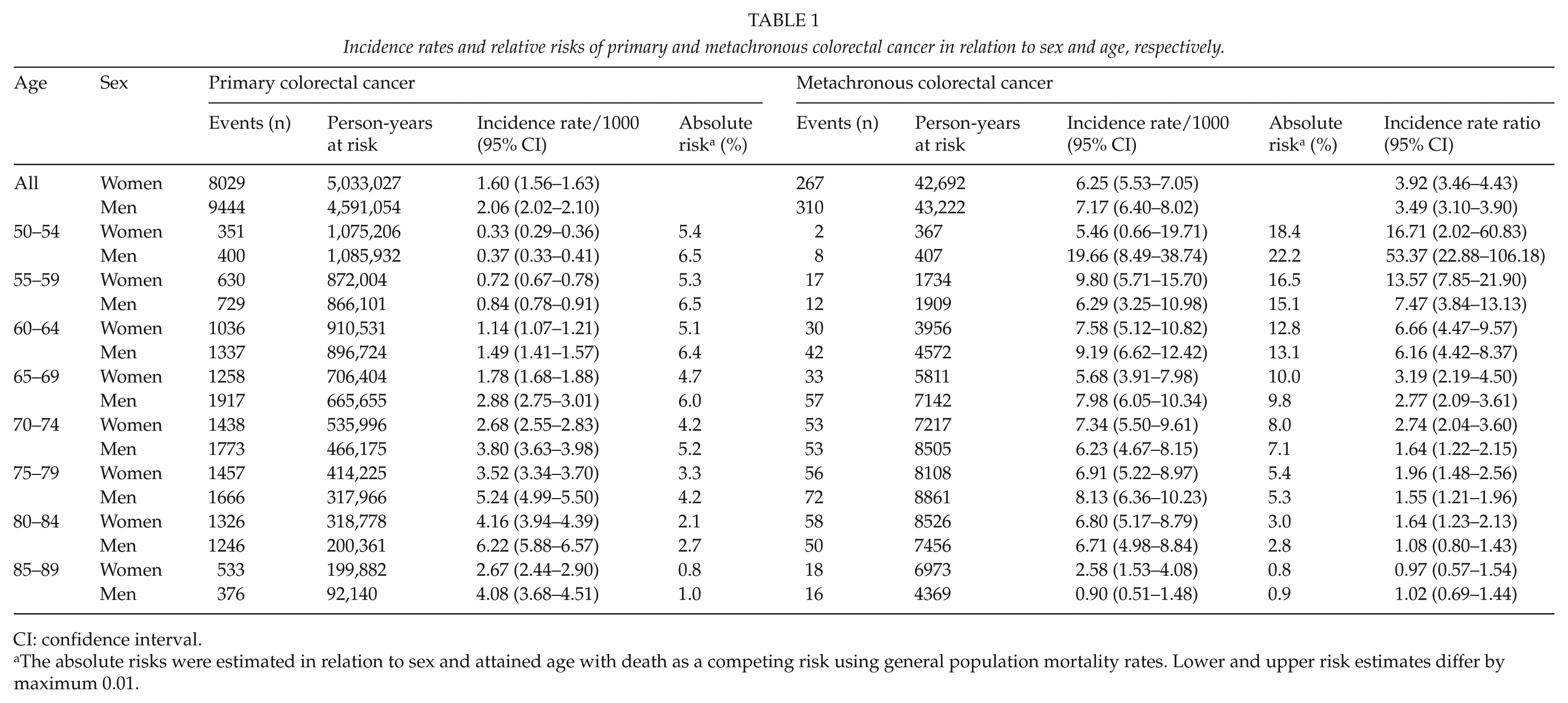
CI: confidence interval.
The absolute risks were estimated in relation to sex and attained age with death as a competing risk using general population mortality rates. Lower and upper risk estimates differ by maximum 0.01.
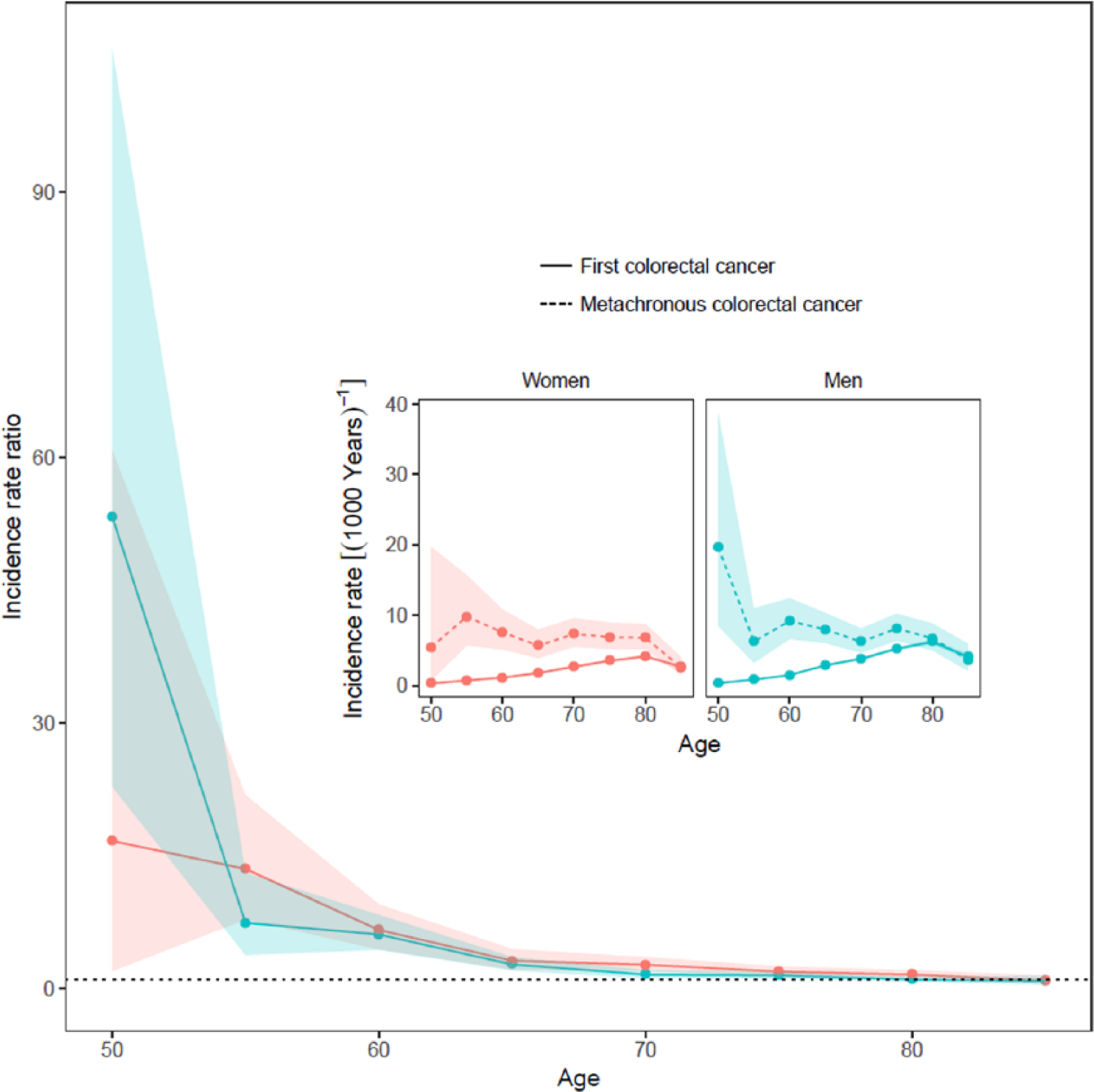
Incidence rate ratios for metachronous CRC in relation to first colorectal cancer in the different age groups: men (blue) and women (red). For each 5-year group, the data are presented at the age of entry. Inserted figures depict the underlying incidence rates. Shaded areas represent 95% confidence intervals.
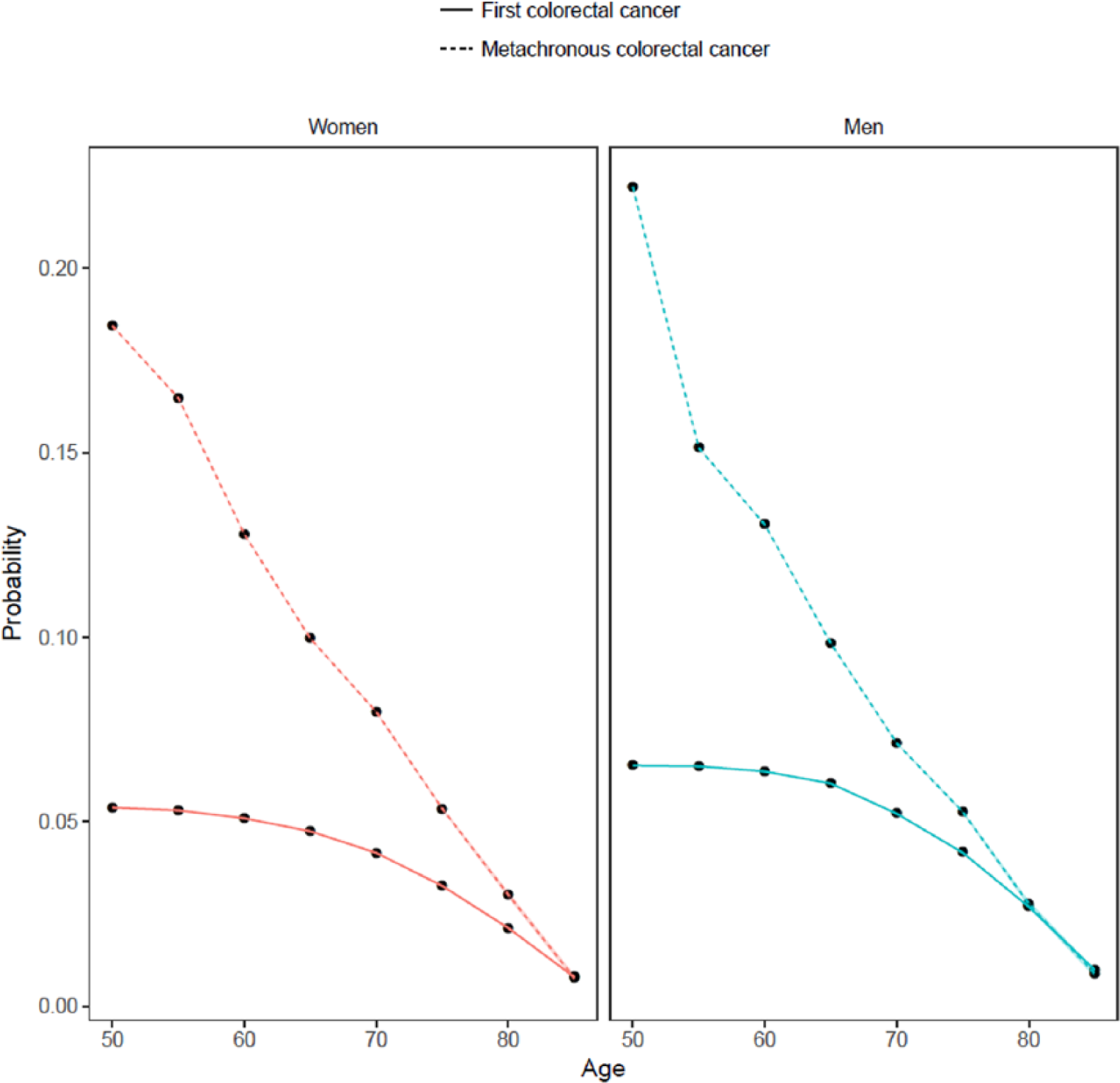
Absolute risk estimates for metachronous CRC (dotted line) in relation to colorectal cancer (full line) for different age groups with separate analyses in men (blue) and women (red).
Synchronous first CRCs were found in 229 (1.3%) patients with a first CRC in the study period (Fig. 1, area A) and in 291 (1.0%) patients who became at risk of MCRC in the study period (Fig. 1, area B). These patients were 2.1 times more often diagnosed with MCRC than patients with a first solitaire CRC (p = 0.01). Tumor location within the bowel had an impact on the risk of MCRC. Primary CRC in all colonic segments except for the transverse colon showed increased IRRs of 1.5–2.5 compared to the rectum, which was set as reference (p < 0.0001).
Discussion
This population-based approach estimates the risk of SCRC and MCRC in patients diagnosed with sporadic CRC after age 50. Based on the national registry approach >9000 CRCs from individuals at risk of familial and/or hereditary cancer were excluded motivated by our focus on non-heritable tumors (Fig. 1). We define a frequency of SCRC of 1.3% and demonstrate that SCRC is associated with a significantly two times increased risk of MCRC, which fits well with previous observations (4, 9). The risk of MCRC was strongly influenced by age. The highest IRRs for MCRC were observed between 50 and 65 years, whereas the IRRs above age 70 in men and above age 75 in women were below 2 (Table 1). Our IRRs are based on IRs of first CRC in age- and sex specific strata in the general population and is thus comparable to standardized incidence ratios (SIRs) reported by others; and our findings support previous observations on SIRs of 5.1–7.5 in patients below age 50 and of 1.0 in patients above age 75–80, although based on a cohort where hereditary cases have as far as possible been excluded (2, 5). Sex had a minor impact on the IRR for MCRC with similar and non-significant differences between the sexes for each age group. The absolute risks of MCRC decreased with age with 9.8%–22.2% in patients below age 70 and 0.8–8.0% in patients above age 70. In individuals diagnosed with a first CRC above age 80 the risk of MCRC was 0.8%–2.7%, which is at the same level as observed by Battersby et al. (8), who identified a 2% 10-year risk above age 75.
The impact from the location of the first CRC within the bowel on the risk of MCRC is a matter of controversy with various conclusions reached. An increased risk of MCRC following a first CRC in the transverse and the descending colon was reported by Phipps et al. (7) and no influence from primary tumor location reported by Levi et al. (5), although several studies have identified increased risks with SIRs of 1.9–2.1 in individuals with a first CRC in the proximal colon (2, 3, 6, 9). The divergent conclusions reached likely reflect differences in study design, follow-up time, and inclusion of subsets with various predispositions. In our series, the location of the first CRC had a minor impact on the risk of MCRC. The lowest risk was seen for primary tumors in the rectum, which was set as a reference. With the exception of the transverse colon, primary tumors within the various colonic segments were associated with IRRs of 1.5–2.5.
Our use of population-based data contributes with robust estimates and as such provides a reference for further work to develop stratified surveillance following a primary CRC. Strengths of the study include possibilities to exclude familial and hereditary cases based on long-term national registration, minimal loss to follow-up (0.007%), minimal misclassification of CRCs during the study period (<0.03%), and long term (70 years) of individuals at risk. Weaknesses include potential inclusion of yet unrecognized cases of familial and hereditary cancer that have escaped recognition and inclusion in the HNPCC-register. Furthermore, we lack data on surveillance and on diagnosis and removal of polyps or carcinomas in situ. The results may also be affected by changing incidence rates, although these have been reported to be stable during the study period (19) and a possible effect from population-based CRC screening is unlikely since this was implemented in Denmark in 2014, that is, after the study period. It is also important to consider the variable definitions of SCRC and MCRC used in international literature. Although we used the more conservative 1-year cut-off to define SCRC versus MCRC and less likely development of SCRC in the cohort studied, the variable definitions used, for primary tumors as well as metastases, decrease comparability of studies in this area (3, 9, 20).
In conclusion, we used population-based data to demonstrate an increased risk of MCRC after exclusion of individuals with young age at onset and familial or hereditary predisposition. Patients with primary SCRC were at increased risk of MCRC and the risk was higher for patients with colon cancer than for rectal cancer. Age was inversely correlated with risk of MCRC with ⩾10% absolute risk for patients with primary CRC below age 65. Taken together, our data underscore the need for surveillance also for individuals affected by sporadic CRC after age 50. Assuming that an absolute risk of 10% motivates surveillance beyond population screening programs, our data suggest surveillance until age 69 for both men and women. Hereafter, population screening may be sufficient and repeat colonoscopies more often than every 5 years is seldom warranted. These data provide a basis for development of stratified surveillance strategies at higher age.
Footnotes
Acknowledgements
Lars Smith-Hansen, the Danish HNPCC-register, Clinical Research Centre, Hvidovre Hospital, and Steffen Bülow, the Danish FAP-register, Gastroenterological Department, Hvidovre Hospital, are acknowledged for extracting register data on hereditary cases.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
According to Danish ethical legislation, register-based studies are not subjected to ethical review, but the study database was approved by the Danish Data Protection Agency (AHH-2014-042).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Danish Cancer Society and the HNPCC-register, Clinical Research Centre, Hvidovre Hospital.
Research Data
Underlying research data related to this article can be accessed from the corresponding author.