
Abstract
Background and Aims:
The reconstruction of the lower lip defects which may result from malignancy, trauma, and burn is necessary for mastication, oral competence, salivary retain, articulation, and aesthetic appearance of the face. While small (30% of the lower lip) and medium (30%–80% of the lower lip) size defects are reconstructed using primary repair and local flaps, reconstruction of the large defects including total and near-total of the lower lip is very challenging entity. We introduce a new modification of the fan flap named extended fan flap for reconstruction of the total and near-total lower lip defects.
Material and Methods:
The extended fan flap was used for 12 patients with defects involving more than 80% of the lower lip due to squamous cell carcinoma excision. Most of the patients were males (80.9%) with an average age of 66.8 years (range, 47–82 years).
Results:
No major complication is observed in the postoperative period. The functional and aesthetic results were satisfactory. The sphincter function for normal mastication, eating, and salivary retain was reestablished. No microstomy was seen and insertion of artificial dentition was possible for patients.
Conclusion:
We believe that the unilateral extended fan flap is a reliable and safe option with satisfactory functional and aesthetic results for total and near-total (more than 80%) lower lip defects.
The lips appear to play an important role as a functional and aesthetical unit of the face. They are responsible for food intake, imbibition, mastication, oral competence, salivary retain, articulation, and speech. The lips take their part in facial expression of emotions and verbal or nonverbal communications. Because of their high number of nerve endings, the lips act like a tactile and erogenous organ. They are also involved in the aesthetic appearance of the face. Lip defects may result from a variety of pathologies such as vascular anomalies, trauma, burns, and tumors. Resection due to squamous cell carcinoma (SCC) is the most common cause of the lower lip defects (1). Smoking and sun exposure are the most frequently seen environmental factors of the lip cancer (2). The main goal of the lower lip reconstruction is restoration of the sphincter function for normal mastication, eating, and salivary retain while reestablishing the aesthetic appearance of the lips.
Various reconstruction techniques for lower lip defects have been described in the literature. Musculocutaneous flap transfers are commonly advocated for reconstruction of the lip defects to maintain the oral competence (3–9). The most important factor is the size of lower lip defect for determining the reconstructive method to be employed. Lower lip defect which is smaller than one-third of the entire lower lip can be closed by primary repair, while the local musculocutaneous flaps such as Abbé flap, Estlander flap, Karapandzic flap, and depressor anguli oris flap may be used for lip defects ranged between 30% and 80% of the lip (3, 8–14). The reconstruction of the total and near-total (more than 80% of the entire lip) lower lip defects are very challenging entity and local flaps such as Gate flap and distant flaps such as radial forearm flaps have been also used (2, 4).
In this study, we introduce a new modification of the fan flap named “Extended Fan Flap” for total and near-total lower lip reconstruction.
Anatomy
An understanding of normal anatomy is important for adequate reconstruction of lip defects. The lips are bordered laterally by the nasolabial crease, superiorly by the base of the nose, and inferiorly by mentolabial crease. The lips consist of three layers, skin, orbicularis oris muscle, and mucosa. The outer border is formed by vermilion which is the mucocutaneous junction between the mucosa and outer skin. The repair of the vermilion border must be accurately maintained because even minor misalignments can be noticeable (12). The central muscle is orbicularis oris which acts as a constrictor. The intrinsic fibers of orbicularis oris which is thinnest and deepest part pass around the angle of the mouth. The extrinsic fibers form the bulk of the muscle. The central fibers of the orbicularis oris cross over, forming the modiolus which is a fibrous structure attached to the deep layers of the skin at the level of commissure. The muscles controlling dilatation also inserts to this structure (13). The depressor muscles of the lip are the depressor anguli oris, the labii inferioris, and platysma. The elevator muscles are the levator labii superior, zygomaticus, risorius, and mentalis. All of these muscles function together to provide the competency of the lips. The zygomatic, buccal, and marginal mandibular branches of the facial nerve innervate the musculature of the lip. The mental branch of the trigeminal nerve supplies the sensory innervation of the lower lip whereas the sensation of the upper lip is derived from infraorbital branch. The blood supply is through the superior and inferior labial arteries which are the branches of the facial artery. The labial arteries course superficial to the orbicularis oris muscle and deep to the mucosal surface of the lip. The veins usually accompany arteries.
Patients and Methods
An informed consent was obtained from each patient. The diagnosis of SCC was confirmed with biopsy prior to the definitive surgery. Preoperative, intraoperative, and postoperative pictures were taken for each patient.
Flap Design
After the resection of the lower lip, precise defect size is determined. For the defects more than 80% of the entire lower lip, reconstruction with extended fan flap is planned. The flap is marked starting from the upper lip toward just lateral to the alar base like Estlander flap. The lateral margins of the flap run along the nasolabial fold and mandibular border (Fig. 1). The width and the length of the flap were designed according to the defect size. Then, the entire flap is elevated including the full thickness of the lip and cheek consisting of the skin muscle and mucosa. During the elevation of the flap located in the upper lip, the vermilion border including superior labial artery is preserved similar to the preparation of Estlander flap. The other important point is that facial artery and the depressor muscles located closer to the mandibular border must be included into the flap. Dissection of the lower border of the flap must be carried out carefully to identify facial artery. The facial artery must be dissected until the mandibular border to allow mobilization and rotation of the flap (Fig. 2). After the flap is elevated, mucosa, muscle, and skin are sutured. Especially at level of oral commissure, the remaining muscles surrounding the mouth, such as zygomaticus major and minor muscles, the risorius muscle, and the buccinators muscle should be carefully sutured to the orbicularis oris muscle. To redefine the mucocutaneous junction of the lower lip, mucosal layer of the flap is advanced and sutured to the skin of the flap (Fig. 3).
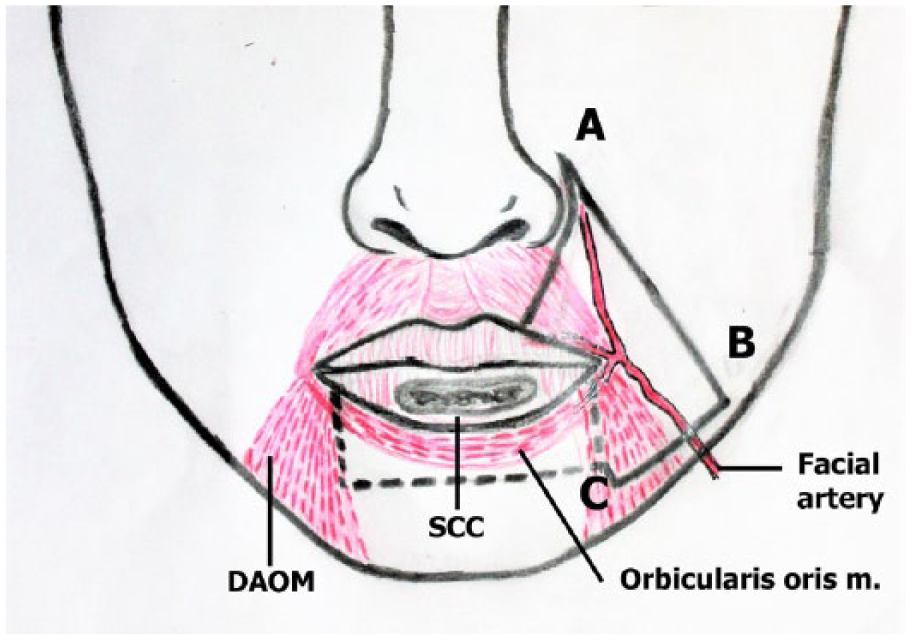
The schematic drawing of the flap design.
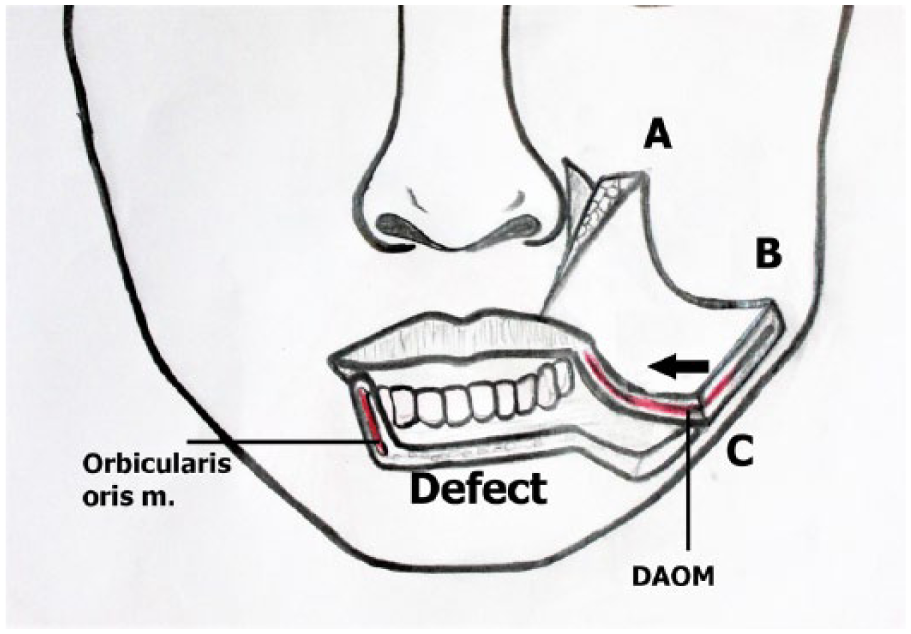
Elevation of the flap.
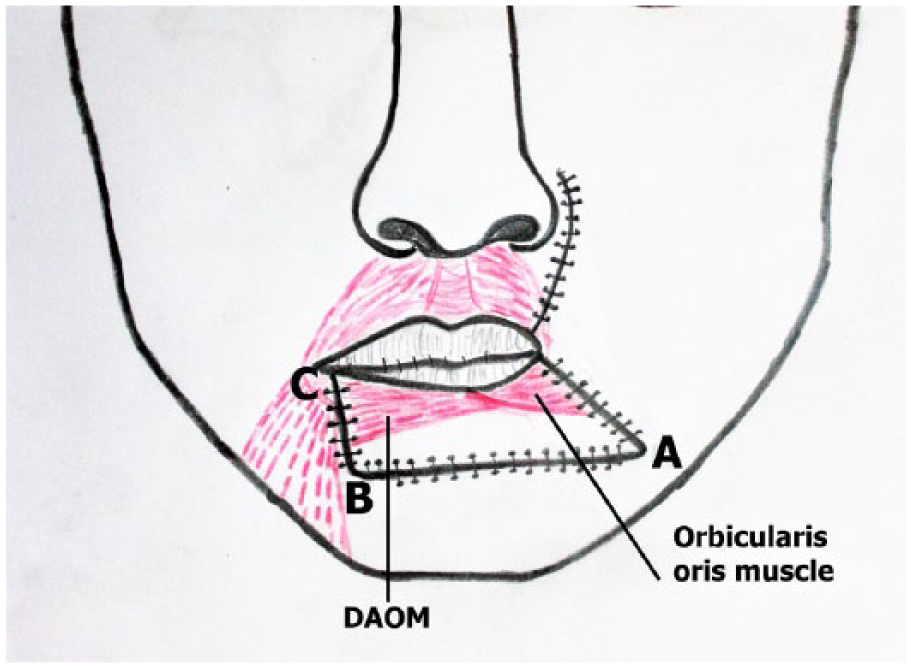
Adaptation of the flap.
Patient 1
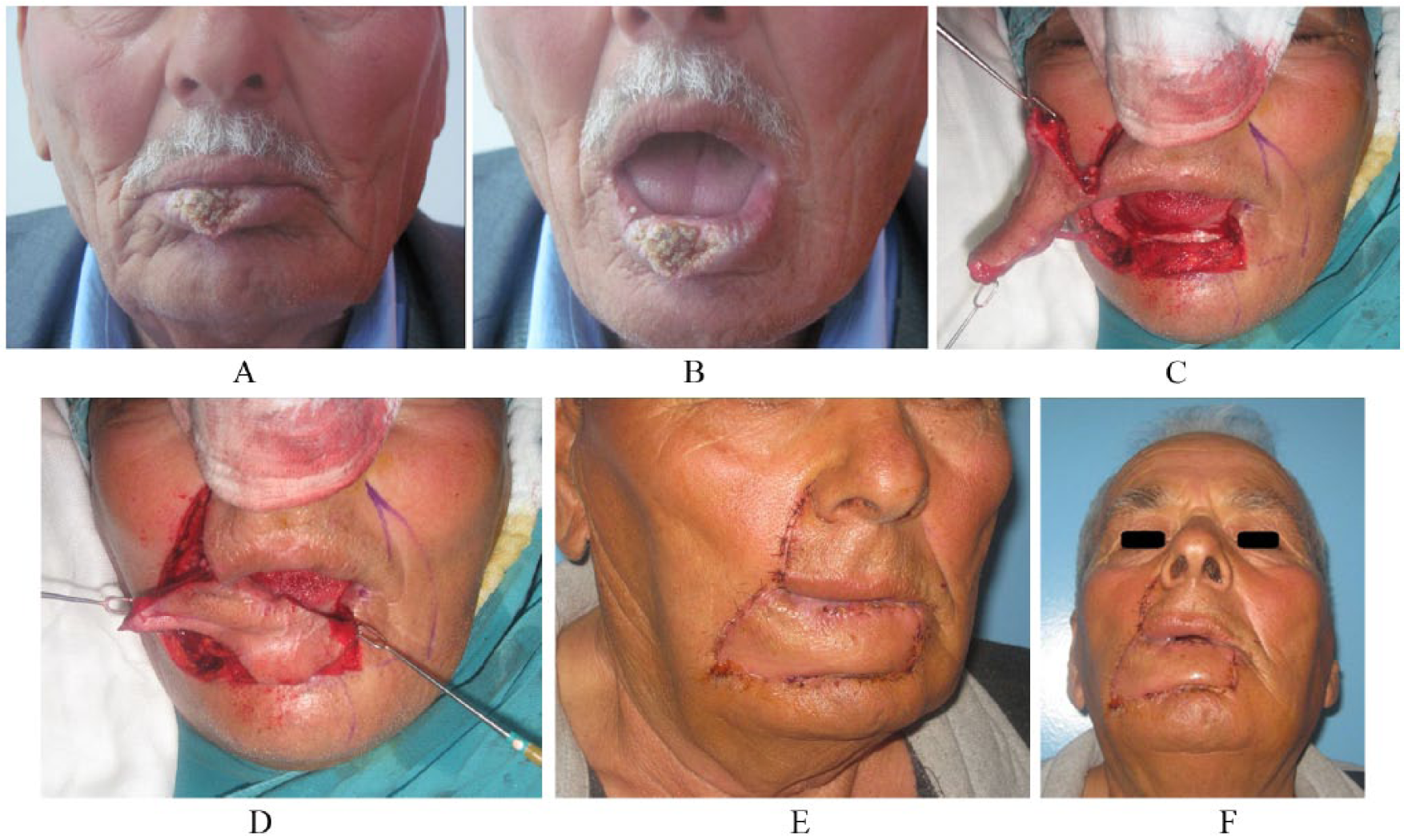
A 78-year-old male patient was admitted to the hospital with complaint of the growing mass and non-healing wound in the lower lip for 5 years. He had an ulcerated mass occupying 2/3 of the lower lip centrally. Histopathology of the incisional biopsy revealed SCC (Fig. 4A, B). The tumor is excised with 1 cm safe margin under general anesthesia. The remaining defect involved more than 80% of the entire lower lip. Lower lip defect was reconstructed using extended fan flap from the left side (Fig. 4C to E). The continuity of the superior labial artery and facial artery is protected. No postoperative complication was seen during the 12-month follow-up. The functional and aesthetic outcomes were acceptable (Fig. 4F–H). During the 6th postoperative month, an electromyographic assessment revealed normal function of the depressor muscles which were included into the flap.
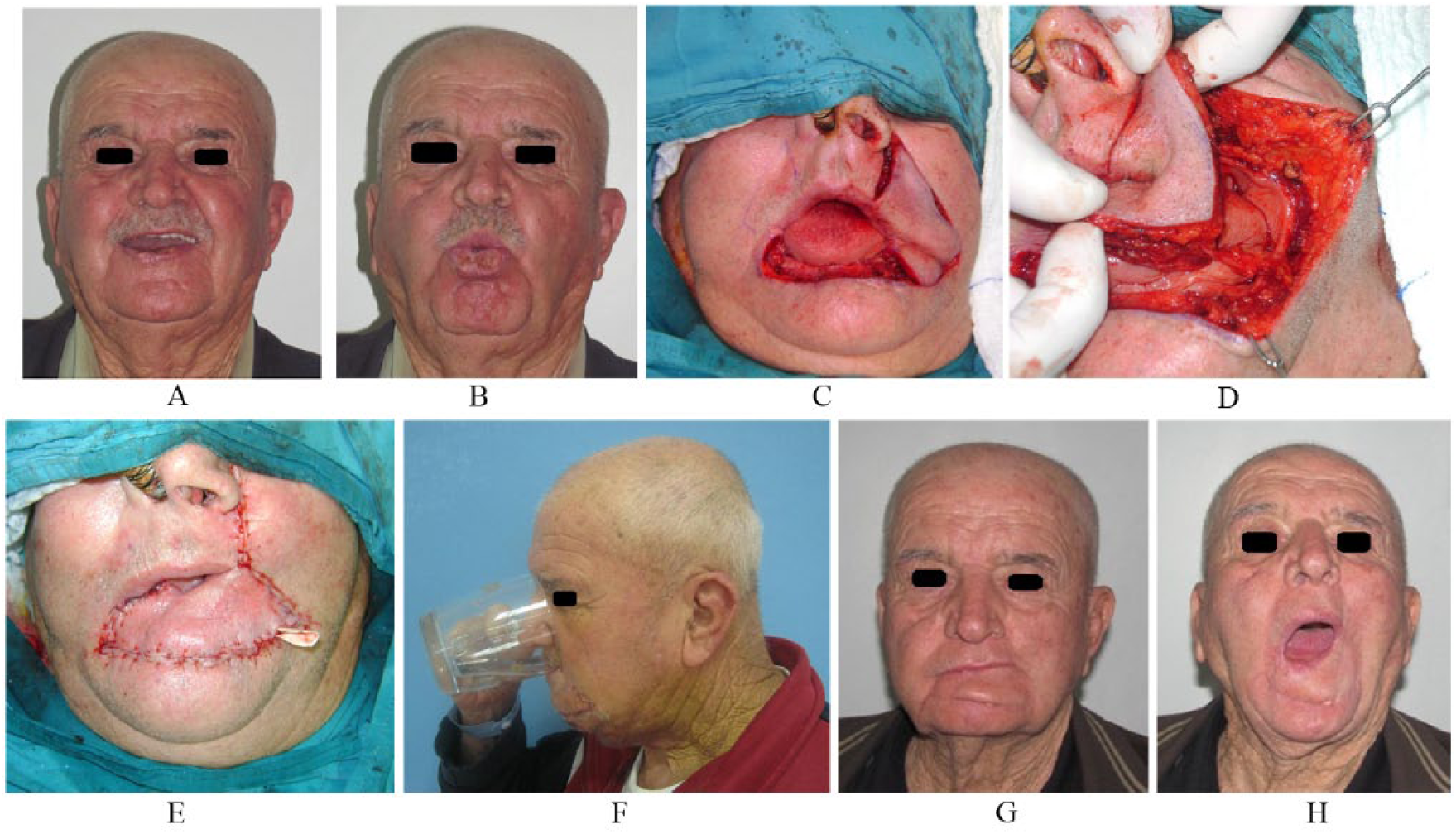
A) Preoperative view of patient 1. B) Preoperative view of patient 1. He had an ulcerated mass including 2/3 of the lower lip centrally. C) to E) Intraoperative view of patient 1. The extended fan flap was elevated from the left side and adapted to the defect. F) Early postoperative view of patient 1. He had full oral competence. No drooling was observed. G) and H) Late postoperative view of patient 1. Although there was a slight asymmetry of left commissure, the aesthetic result was satisfactory for the patient. The mouth opening was adequate.
Patient 2
A 70-year-old male patient had ulcerated lesion of lower lip. The lesion was located on the central two-thirds of the lower lip. The incisional biopsy revealed SCC (Fig. 5A, B). He is operated under general anesthesia and the tumor is excised with 1 cm safe margin. A defect encountering more than 80% of the lower lip including right lower lip commissure is reconstructed with extended fan flap from the right side (Fig. 5C, D). No complication after surgery is observed and the result was satisfactory (Fig. 5E, F).
A) and B) Preoperative view of patient 2. He had an ulcerated mass including 2/3 of the lower lip. C) and D) Intraoperative view of patient 2. The extended fan flap was elevated from the left side. The facial artery which was included in the flap is visible. The mucosa at the site of vermilion was planned 5 mm greater than the skin for the reconstruction of the mucocutaneous junction of the reconstructed lip. E) and F) Early postoperative view of patient 2. The vermilion line is visible.
Results
A total of 21 patients with defects more than 80% of the entire lower lip were reconstructed using extended fan flap. Most of the patients were males (80.9%) with an average age of 66.8 years (range, 47–82 years). All the patients’ histopathological assessment revealed SCC. The average defect size was 85.4% of the lower lip. During the postoperative period, no complication such as venous and arterial circulation disturbances was observed except minor wound dehiscence which was seen in three patients. Wound dehiscence was treated with wound care and healing by secondary intention, except one case which required primary wound closure. Oral ingestion was possible 24 h later after the operation. The oral competences were good and patients’ speech was understandable. The mouth opening was adequate and there was no drooling. Insertion of the artificial dentition was possible for all patients. Although there was a slight asymmetry of the commissure at the site of flap, aesthetic result was acceptable. The mean follow-up time was 12.1 months. In order to evaluate the sensibility of the reconstructed lip, Semmes-Weinstein Monofilament Test (SWMT) and two-point discrimination tests were performed. These tests were not performed in six patients who could not be reached in the late postoperative period. None of the patients showed the evidence of loss of protective sensation according to SWMT. The result of two-point discrimination test varied between 3 and 8 mm. The detailed patient data are shown in Table 1.
Patient data.
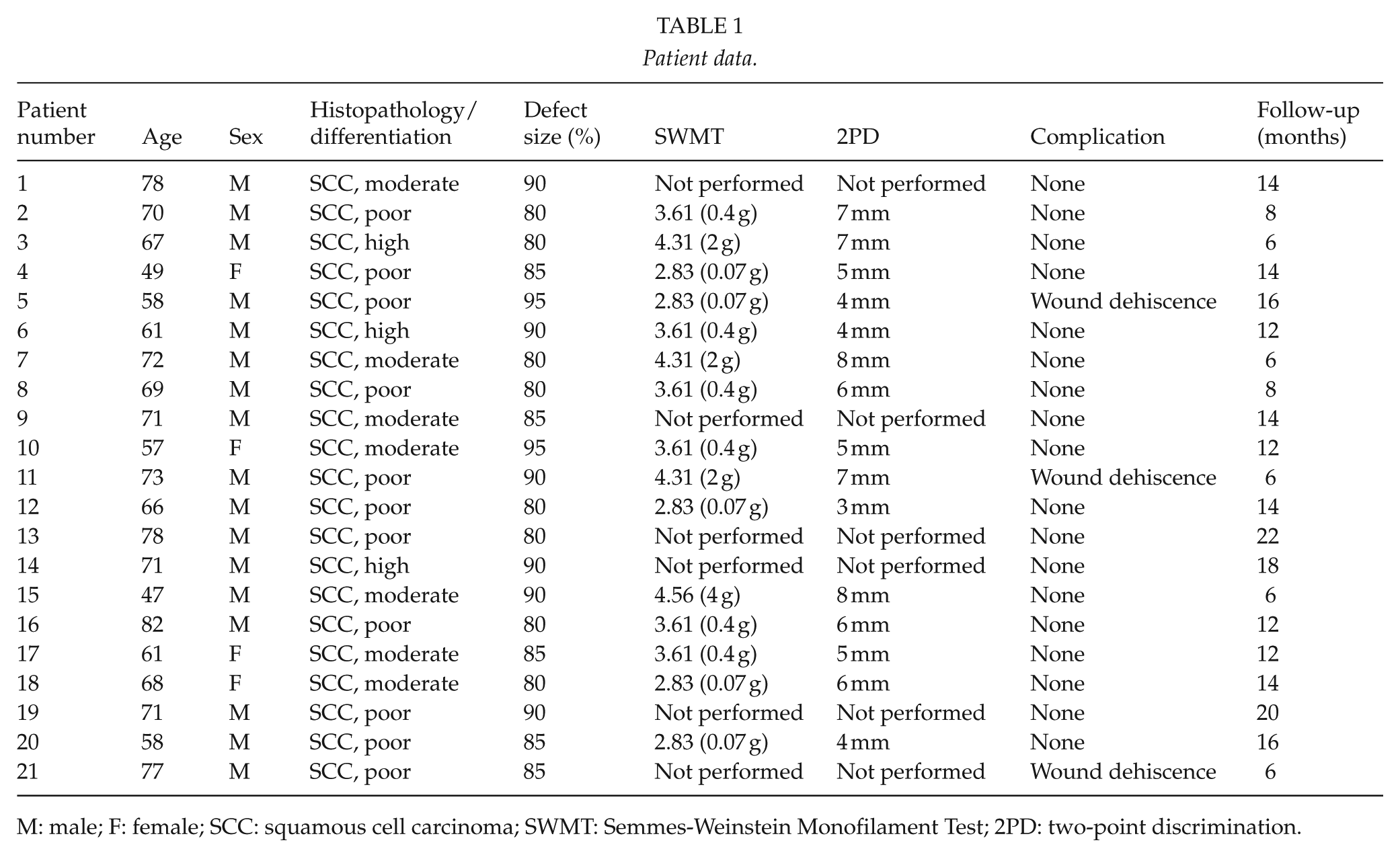
M: male; F: female; SCC: squamous cell carcinoma; SWMT: Semmes-Weinstein Monofilament Test; 2PD: two-point discrimination.
Discussion
The large sized defects involving more than 80% of the lower lip sometimes needs more challenging reconstructive procedures. Although some local flaps including Bernard-Webster technique, bilateral gate flaps, double cross-lip flap, and the depressor anguli oris musculocutaneous flap have been reported in the literature for large lower lip defects. Microvascular free flaps (radial forearm flap, anterolateral thigh flap, gracilis flap) have also been used in extensive defects (4, 5, 8, 14–22).
The bilateral fan flaps, as described by Gillies in 1920 and modified by McGregor, provide a tissue with similar quality and texture for lower lip reconstruction (23). Rotation of the flaps as a fan shape reduces size of the oral opening causing microstomy which is especially important for the patients who require total lower lip reconstruction. Fan flaps are generally used bilaterally for lower lip defects. Facial and inferior labial arteries are always expected regarding the blood supply of bilateral rotation fan flaps. The rotation of the medial cheek flaps causes a distortion of the anatomy of the commissures. Distortion of the commissures may be restored using a commissurotomy, if necessary (24). Classical fan flaps may also cause distortion of the orbicularis oris muscular fibers because the orbicularis is not completely dissected and advanced but rather is pulled with pedicle. Full functional recovery and sensation may not return and oral incompetence may also result in patients who have lower lip reconstruction with classical fan flaps (2T). In extended fan flap technique, orbicularis oris muscle from the upper lip was fully dissected and rotated like Estlander flap and muscle fiber direction oriented in the right direction like lower lip orbicularis oris. The remaining depressor muscle fibers are also included in the extended fan flap and muscle fibers are directed horizontally oriented after 90 degree rotation. The extended fan flap includes orbicularis oris muscle and depressor anguli oris muscle which is close relationship at commissure level with orbicularis oris muscle. These muscles’ fibers are aligned horizontally. In our technique, these muscle fibers were sutured to the remaining orbicularis oris muscle at the other end of the defect. The functional outcomes such as good oral continence and salivary retain are results of the restoration of the circular anatomy of the muscle. The good functional recovery rates have been reported in the literature for Estlander flap which has been used for dynamic reconstruction of the middle-sized lower lip defects. We believe that good functional results of the extended fan flap are also dependent on the planning and dissection of the upper part of the flap like Estlander flap rather than fan flap.
The unilateral extended fan flap which was designed in this study was sufficient for total and near-total lower lip defects and one of the commissures was preserved. The results showed that the remaining mouth opening was sufficient for eating and using artificial dentition. We think that the size of the extended fan flap was really larger than the fan flap and Estlander flap, and the circulation from the upper labial artery may not be sufficient for the flap. Because of this reason, during the elevation of the extended fan flap, facial artery was dissected and included into the flap and the circulation from the upper labial artery was also preserved. Because of this rich dual vascular supply, no vascular complication was observed.
The sensation of the reconstructed lower lip is very important. Reconstruction of the lower lip with extended fan flaps preserves the opposite commissure and mental region and this might allow the restoration of the sensation of the flap. In our study, patients who were tested for Semmes-Weinstein monofilament examination did not show any evidence in loss of protective sensation. The results of SWMT were at least 4.56 (4 g) or better. These results were approved by the similar scores of two-point discrimination test which ranged between 3 and 8 mm.
The sensorial reinnervation of the flap could benefit from the rich sensorial network in perioral region. In our study, we did not add the infraorbital nerve into the flap to anastomose to a branch of the mental nerve. However, this can be considered in future cases.
The aesthetic results of the patients were satisfactory both for the surgeon and the patients; however, there was a slight asymmetry and elevation of the commissure at the flap’s donor site. The vermilion of the reconstructed lip composed is partially the upper lip vermilion and the rest is formed by suturing the edge of oral mucosa of the transposed flap to the skin margin. However, this mucosa is not sufficient for reconstruction of the vermilion so the flap mucosa should be prepared at least 5 mm larger than the skin to achieve vermilion reconstruction. Secondary procedures such as commissurotomy for commissural asymmetry and fat grafts for vermilion asymmetry may be employed to achieve better aesthetic results.
We believe that the extended fan flap is a reliable option with good functional and acceptable aesthetic results for total and near-total lower lip defects.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
We confirm that Ethical Committee approval was sought where necessary and is acknowledged within the text of the submitted manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
All authors hereby confirm that guidelines on patient consent have been met and any details of informed consent obtained are indicated within the text of the submitted manuscript.