
Abstract
Venous malformations often manifest in early childhood and do not spontaneously resolve. Most vein malformations of the lips are typically treated at a young age, with giant arteriovenous malformations being particularly rare. Herein, we introduce the case of a 47-year-old man who presented to our department complaining of a progressive mass on his lower lip. Clinical examination revealed a mass measuring 10 cm × 8 cm × 4 cm in size, characterized by a soft texture and smooth edges. Despite a series of sclerotherapy interventions, the lesion remained unresponsive. Consequently, we performed a preoperative embolization of the malformed vessel using digital angiography, followed by extensive resection of the lesion and repair of the defect using an adjacent flap. The postoperative period was uneventful, and no local recurrence was observed during a 4-year follow-up period. Therefore, we recommend preoperative angioembolization as a valuable approach for addressing large lower lip deformities to enable extensive surgical resection and robust therapeutic outcomes.
Introduction
Vascular anomalies can be stratified into hemangiomas and vascular malformations (VMs). 1 Congenital VMs, typically present at birth, may continue to grow and can be exacerbated by trauma and hormonal changes. Lips, owing to their rich vascular network, are susceptible to enlargement and deformation when arteriovenous malformations occur. VMs are mostly treated at a young age, and primary treatment approaches include laser therapy, photocoagulation, sclerotherapy, vascular embolization, and surgical resection.2,3 The choice of treatment approach largely depends on the size and location of the lesion, with large and complex lesions often necessitating the involvement of a multidisciplinary team. 4 The stomatology and interventional therapy department assessed the present case of giant venous malformation of the lower lip, and we opted for an angiography prior to resection to embolize the malformed feeding artery. This facilitated the mass removal under general anesthesia and reconstruction of the lower lip using a unilateral nasolabial groove musculocutaneous flap.
Case Report
The 47-year-old male patient was born with a lower lip lesion measuring approximately 5 mm × 5 mm in size, accompanied by local red plaques. The mass exhibited progressive enlargement, and, at times, surface ulceration would cause pain. After the age of 15, the tumor’s growth escalated, leading to significant deformation of the lower lip. A series of local sclerotherapy was conducted at several hospitals, but it proved ineffective in fully controlling the abnormal growth.
Upon clinical examination at our department, the patient’s lower lip appeared substantially enlarged, measuring around 10 cm × 8 cm × 4 cm in size. Additionally, his lip was red, soft, non-tender, and exhibited compressibility. Positive eversion of the mucosa of the lower lip was observed, along with a dry mucosal surface devoid of obvious ulceration. The uplift was around the midline of the lip, with a slightly less pronounced uplift on the right side compared to the left (Figures 1A and 1B).
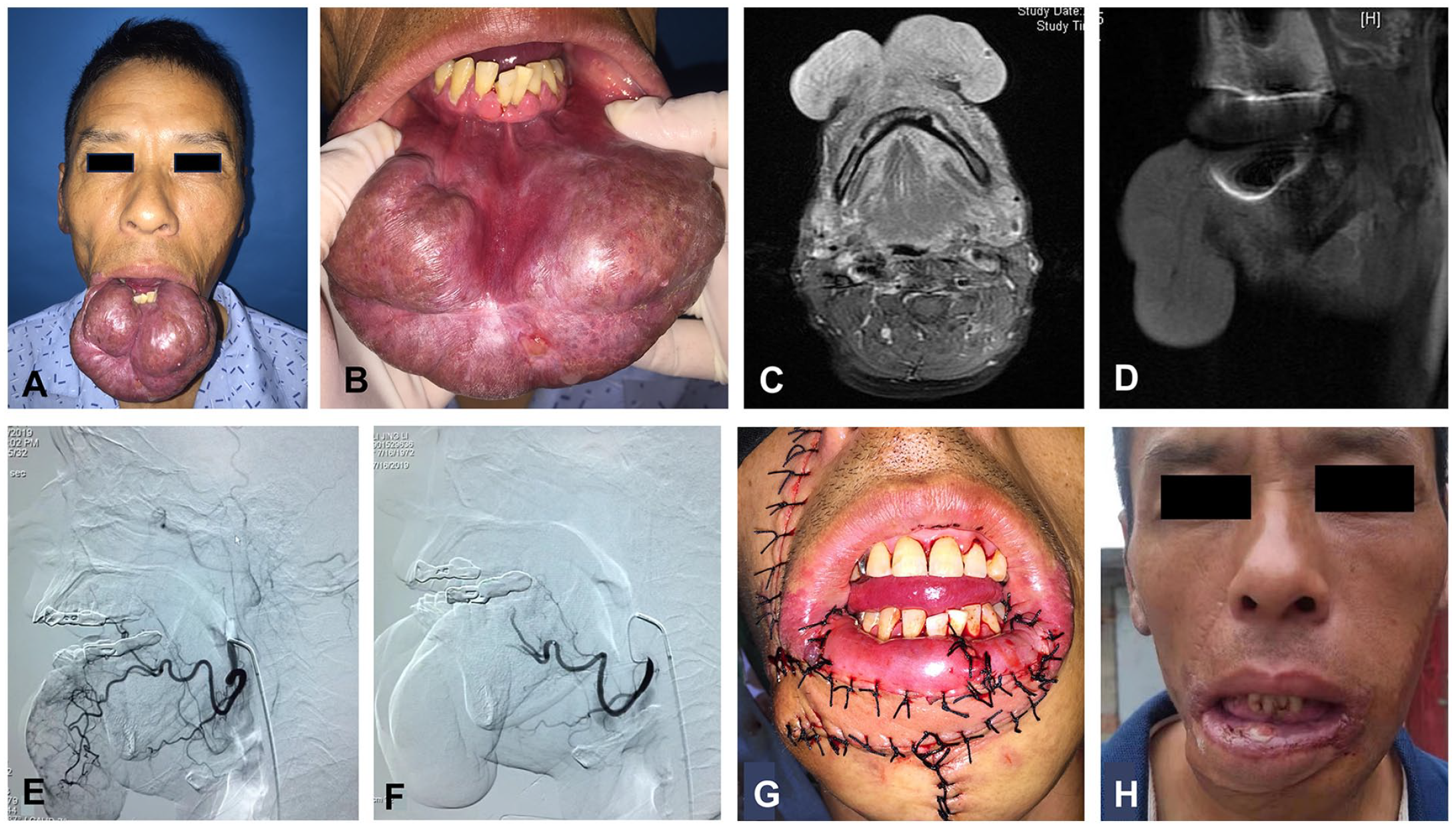
(A) Lateral view of the patient’s lip. (B) Frontal view of the patient’ s lips. (C) Coronal view of the lower lip lesion (D) Sagittal view of the lower lip lesion. (E) Before arterial embolization. (F) After arterial embolization. (G) Immediately after surgery. (H) One year after surgery.
Imaging examination revealed the presence of a large soft tissue lesion in the lower lip and chin, with a cross-sectional area of 31 mm × 97 mm × 79 mm, and cord-like low-signal shadows were seen internally, consistent with VM (Figures 1C and 1D). Subsequently, angiography was performed via the femoral artery under local anesthesia, revealing marked arterial filling on the left side of the lower lip while the right supplying artery remained unperfused. During the procedure, the left external maxillary artery was selectively catheterized, and gelatin sponge particles (ranging from 350 to 560 μm to 1000 to 1400 μm) were utilized for embolization of the lower lip artery. Angiography further confirmed the cessation of arterial blood supply (Figures 1E and 1F).
The surgical intervention involved the removal of the mass and the affected portion of the lower lip. A transfer of the right nasolabial fold skin flap was performed to address the lower lip defect, restoring both its height and width. Furthermore, the vermilion of the lower lip was reconstructed using inverted buccal mucosa (Figure 1G). Histopathological analysis indicated diffuse growth of VMs within the submucosa and myometrium, extending to the peripheral edges and basal layer, without evident endothelial abnormalities, confirming the venous malformation diagnosis (Figure 2).
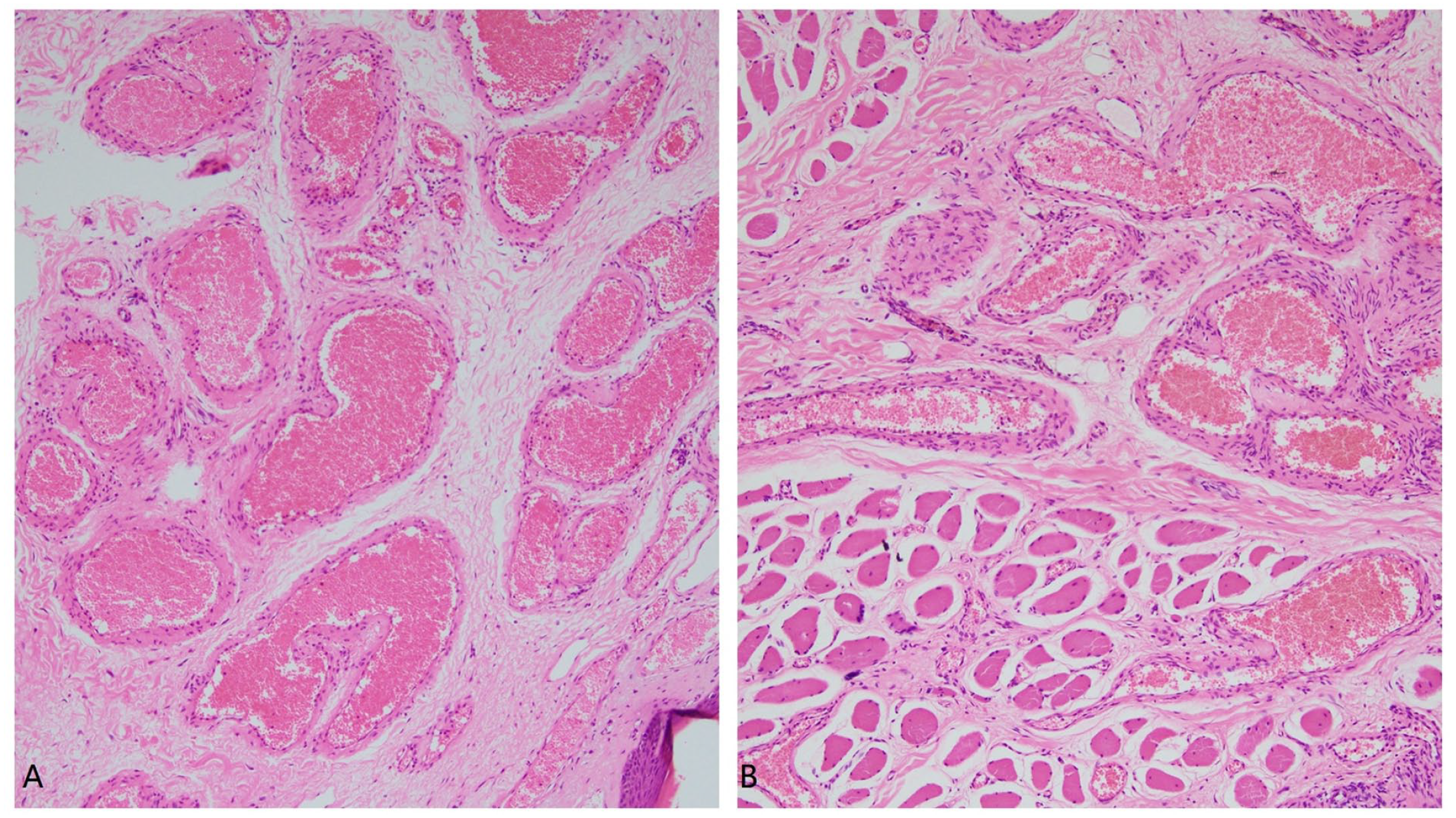
Hematoxylin–eosin staining (×100) reveals the extent of venous malformation infiltration in the (A) mucosa and (B) muscle tissues.
Following the surgical intervention, the lower lip regained its normal appearance, exhibiting proper lip closure functionality, and did not affect the patient’s pronunciation. Notably, no local recurrence was observed during a 4-year follow-up period (Figure 1H).
Discussion
VMs are categorized into 3 primary types: microvenous malformations, venous malformations, and arteriovenous malformations. 5 Diagnosis predominantly relies on a combination of patient history, clinical assessment, ultrasound, and magnetic resonance imaging. Clinical presentations of VMs encompass a broad spectrum of manifestations, ranging from asymptomatic varicose veins to more pronounced alterations such as extensive facial deformities. Common characteristics of VMs include soft, compressible, pulseless bluish-violet papules or nodules that may grow in size over time.5,6
The treatment of VMs is contingent upon several factors, including their location, volume, as well as the psychological and aesthetic considerations of the patient. Treatment modalities include laser therapy, sclerotherapy, surgery, and vascular embolization. 7 Laser therapy is usually applied to small, superficial cutaneous venous malformations and capillary malformations, yielding favorable aesthetic outcomes. Sclerotherapy, generally a minimally invasive option, can yield effective results when used as a standalone treatment. 8 Its principle in-volves inducing injury to vascular endothelial cells, provoking inflammation and fibrosis, gradually leading to the occlusion or restricted growth of the hemangioma’s lumen. Surgical intervention is typically reserved for cases necessitating correction of facial deformities or VM located in proximity to critical anatomical structures, precluding sclerotherapy as a viable option. In instances of more extensive malformations, a combination of treatment methods may be employed.
Herein, the patient had previously undergone multiple sclerotherapy sessions at other hospitals. However, these treatments failed to resolve the issue of impaired mouth closure function associated with the enlarged lip, necessitating surgical intervention. The lip is a highly vascularized anatomical region with significant functional importance. To mitigate bleeding during surgery, preoperative digital angiography was employed to embolize the dominant artery of the lip. Vascular embolization can be categorized as either permanent or temporary. Commonly used embolization methods include the use of spring coils, polyvinyl alcohol (PVA) particles, n-butyl cyanoacrylate (nBCA), and gelatin sponge, with PVA particles, nBCA, and spring coils being examples of permanent embolization agents. In contrast, gelatin sponge is employed as a temporary embolization material. 9 It is a protein-based adhesive substance devoid of antigenicity, thereby avoiding toxic and adverse effects while being well-tolerated. Gelatin sponges are absorbable, typically being resorbed within 2 weeks, allowing for the restoration of blood flow in vessels. Temporary embolization serves to reduce intraoperative bleeding and facilitates the post-surgery restoration of blood flow in non-lesioned areas. 10 In the present case, gelatin sponge was used for preoperative embolization, yielding favorable outcomes.
During the surgical procedure, the VM affecting the lower lip was completely excised. The primary goals of the reconstruction were to restore both the white and red portions of the lip, reestablish the height and width of the lower lip, and simultaneously reinstate the functional ability of the lower lip for activities like sucking. 11 Geelan-hansen et al. 12 previously described various flap techniques essential for lip reconstruction, as well as the refinement of lip contour through secondary surgery. In the present case, the choice of the nasolabial artery flap was motivated by the substantial defect. The nasolabial sulcus flap possesses muscle tissues with the ability for expression, and has attributes suitable for the partial restoration of the orbicularis oris muscle’s function. Moreover, it can be used to effectively reconstruct both the aesthetics of the white and red lip. Since the left nasolabial artery had been embolized, the decision was made to use the right nasolabial flap for the reconstruction of the lower lip to ensure the procedure’s success. Additionally, the excess buccal mucosa resulting from the medial expansion of the buccal mucosa of the skin flap was utilized for the reconstruction of the lower lip’s red portion. The surgical outcome was highly satisfactory, obviating the need for further local dressing or intervention.
Conclusion
Huge lip malformation resulting from vascular lesions of the lower lip necessitates a multidisciplinary approach to treatment. Preoperative embolization plays a crucial role in enhancing the safety of surgical resection and facilitates precise design and reconstruction of both the form and function of the lower lip.
Footnotes
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethics committee of the Affiliated Hospital of Qingdao University. The patients/participants provided their written informed consent to participate in this study.