
Abstract
Background:
Acute cholecystitis has the potential to cause sepsis and death, particularly in patients with poor physiological reserve. The gold standard treatment of acute cholecystitis (cholecystectomy) is often not safe in high-risk patients and recourse is made to percutaneous cholecystostomy as either definite treatment or temporizing measure. The aim of this study is to evaluate early and late outcomes following percutaneous cholecystostomy in patients with acute cholecystitis treated at our institution.
Methods:
All patients who underwent percutaneous cholecystostomy for acute cholecystitis (excluding patients with malignancy) between January 2005 and September 2014 were included in the study.
Results:
A total of 53 patients (22 female, median age, 74 years; range, 27–95 years) underwent percutaneous cholecystostomy during the study period. In total, 12 patients (22.6%) had acalculous cholecystitis. The main indications for percutaneous cholecystostomy were significant co-morbidities (n = 28, 52.8%) and patients too unstable for surgery (n = 21, 39.6%). The median time to percutaneous cholecystostomy from diagnosis of acute cholecystitis was 3.6 days (range, 0–45 days). The median length of hospital stay was 27 (range, 4–87) days. The overall 90-day mortality was 9.3% with two further deaths at 12-month follow up. The mortality was significantly higher in patients with American Society of Anesthesiology grade 4–5 (18% vs 0% in American Society of Anesthesiology grade 2–3, p = 0.026) and in patients with acalculous cholecystitis (25% vs 4.5%, p = 0.035). The overall readmission rate was 18%. A total of 24 (45.2%) patients had surgery: laparoscopic cholecystectomy, n = 11; laparoscopic converted to open, n = 5; open total cholecystectomy, n = 5; open cholecystectomy, n = 1; laparotomy and washout, n = 1; laparotomy partial cholecystectomy and closure of perforated small intestine and gastrostomy, n = 1.
Conclusion:
Percutaneous cholecystostomy is a useful temporary or permanent procedure in patients with acute cholecystitis of both calculous and acalculous origin, who are unfit for surgery.
Introduction
Acute cholecystitis (AC) has the potential to cause sepsis and death, particularly in patients with significant co-morbidities and poor physiological reserve (1–3). The most common cause of AC is gallstone related (calculous cholecystitis, CC), and in a minority of patients, it is associated with an underlying critical illness, diabetes, immunosuppression, chronic kidney disease, viral illness, hemoglobinopathies, and vasculitis (acalculous cholecystitis, ACC) (4–6).
The treatment of CC is antibiotics followed by early laparoscopic cholecystectomy (7). The treatment of ACC is antibiotics and treatment or optimization of underlying illness and cholecystectomy. A minority of patients in both groups can be unfit for surgery due to overwhelming sepsis, co-morbidities, or poor physiologic reserve. In these groups of patients, alternative treatment options such as percutaneous cholecystostomy (PC) can be used as a treatment option (8). PC involves radiological placement of a percutaneous drain into the gallbladder under image guidance using either modified Seldinger technique or trocar technique. It can, therefore, serve as a bridging therapy allowing patients to recover from the acute illness and become stable enough to undergo surgery. There is lack of evidence as to the outcome of high-risk patients with AC deemed unfit for surgery. In patients whose pre-morbid state prevents an operation, it may be the definitive management. The aim of the study was to determine the early and late outcomes of PC in a tertiary care hospital.
Materials and Methods
All patients who underwent PC for non-malignant causes of AC between January 2005 and September 2014 at our institution were included in the study. Patient details were obtained from a software called CRIS™, which contained information about all imaging in real time performed at the hospital. The CRIS software was searched for all reports containing the word “cholecystostomy” during the study period. All patients with no gallstones on imaging were diagnosed to have ACC (Fig. 1).
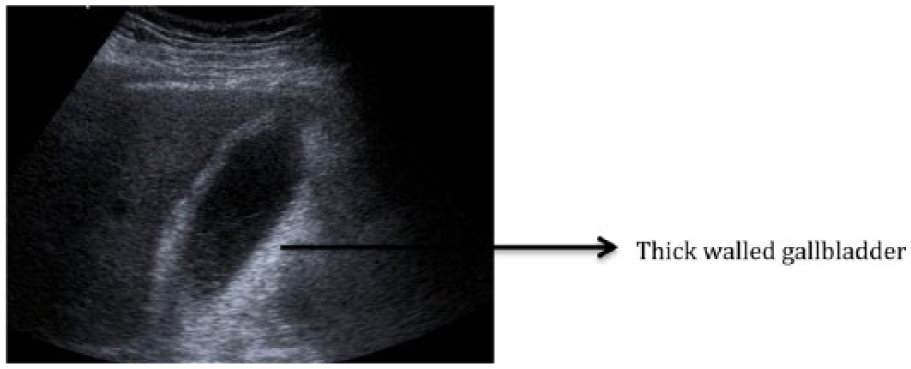
Ultrasound image showing thickened gallbladder (GB) wall >3 mm in keeping with acalculous cholecystitis (ACC).
A total of 53 patient notes were reviewed and the following information was collected for analysis: patient demographics, history and examination, details of all investigations, indication for PC, duration between the diagnosis and decision to treat with PC, duration between decision to treat with PC and time of PC was performed, post-procedure complications, and long-term management of patients. PC was performed under local anesthetic, using the aseptic technique an 18G needle is inserted into the gallbladder transhepatically with direct ultrasound guidance (Fig. 2). 0.035 amplatz® stiff wire is inserted through the needle and 8F or 10F locking pigtail catheter placed. The drain is left on free drainage until sepsis settled. A tubogram (Fig. 3) is performed to access the cystic and common bile ducts patency before capping the drain. We routinely perform a repeat tubogram as soon as signs of sepsis have improved and drain fluid was clear bile. In patients with drain-related issues, tubogram was arranged as soon as possible. In patients with stones in the common bile duct on initial tubogram, a repeat tubogram was arranged after stones were removed via ERCP.
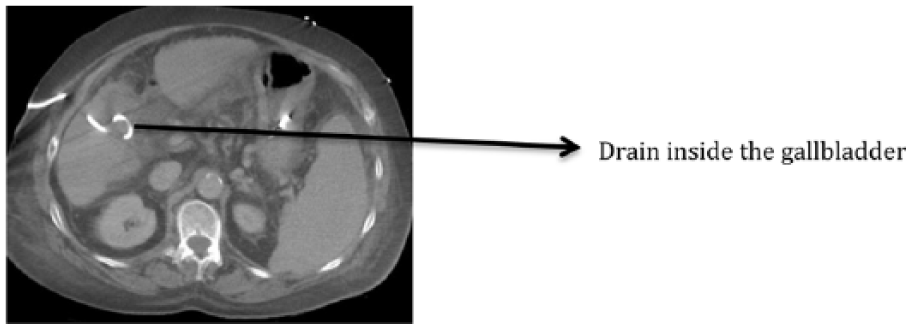
CT image demonstrating transhepatic placed drainage catheter into gallbladder, which is decompressed due to external drainage.

Fluoroscopy image showing drain in the gallbladder. Contrast injected through the drain demonstrating free flow of contrast from the GB into the cystic duct, common bile duct (CBD), and in the duodenum. No filling defects seen.
Patients who were fit enough to have cholecystectomy had removal of PC tube at the time of cholecystectomy, which was usually around approxi-mately 6 weeks. For patients proceeding to cholecystectomy after PC, the outcome of surgery and the associated complications were recorded. All patients were followed up for at least 1 year to determine the outcome of patient and procedure.
Statistical Analysis
Statistical analysis was carried out using chi-square and Mann–Whitney U tests where appropriate and a p-value of <0.05 was considered statistically significant.
Results
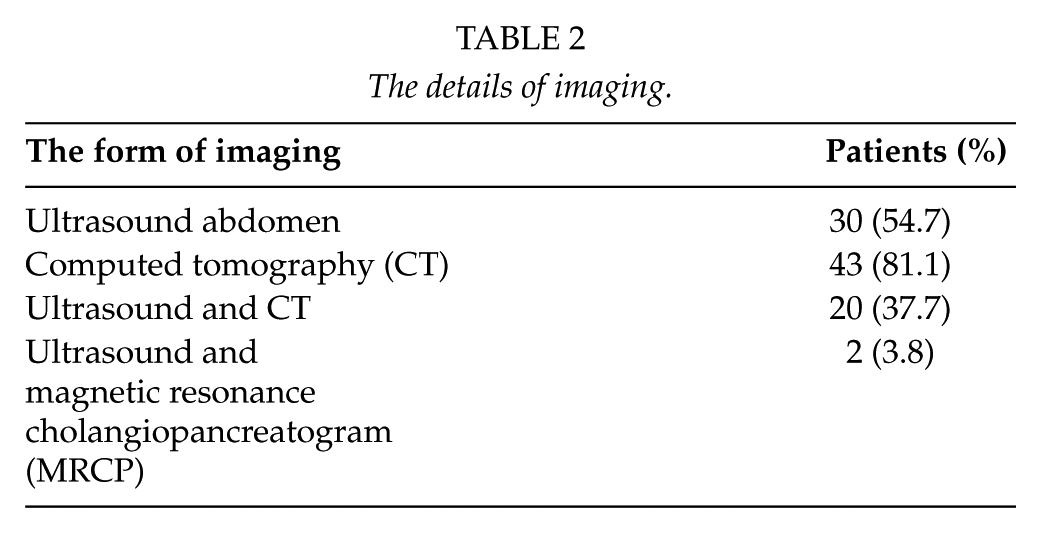
During the study period, 53 patients had PC for AC. Patient characteristics are described in Table 1. A total of 27 (51%) patients were admitted under the care of surgeons, whereas 19 patients were under physicians and 7 directly to the intensive care unit (9). The main reasons why patients were considered unfit for cholecystectomy are described in Table 1.
Patient demographics.
PC: percutaneous cholecystostomy.
The details of imaging that patients had prior to PC are described in Table 2. The median time from admission to imaging was 1 day (range, 0–45 days). A total of 13 patients (24.5%) with no gallstones were diagnosed with ACC. The median time from diagnosis of AC to PC was 3.6 days (range, 0–45 days); however, the time from decision to treat with PC and having PC was a median of <1 day (range, 0–2 days). The median length of hospital stay was 27 days (range, 4–86 days) and median time from PC to discharge was 21 days (range, 2–79 days).
The details of imaging.
During the study period, 11 patients had magnetic resonance cholangiopancreatogram (MRCP) to look for common bile duct pathology following PC. In total, 10 patients had ERCP and 1 patient had both MRCP and ERCP following PC. Eight patients found to have stones in the bile duct subsequently underwent ERCP and removal of stones. Two patients who did not have prior MRCP had negative ERCP. A total of 38 patients had tube cholecystography (Fig. 3) prior to any form of definitive treatment. Three patients who died in the hospital did not have any further imaging. In two patients drain came out prematurely. One patient was transferred to a peripheral hospital and lost to follow-up. The information about the duration of the drain was not available in four patients, of the remaining the drain was removed earlier than 6 weeks in 30 patients (56.6%) and later than 6 weeks in 14 patients (26.4%). The median duration of the drain was 21 (4–336) days. We followed all these patients and found out that 81% had no further recurrence of cholecystitis and drain was removed. In patients who were re-admitted, over half of the re-admissions were due to recurrent cholecystitis and the rest were issues related to drain. Overall readmission rate within 90 days was 18%. The details of readmission are described in Table 3. Two patients have been readmitted due to the displacement of the drain on day 4 and day 15 and both of them had a cholecystectomy during the second admission.
Details of readmission, drain-related complications, and mortality associated with acute cholecystitis.
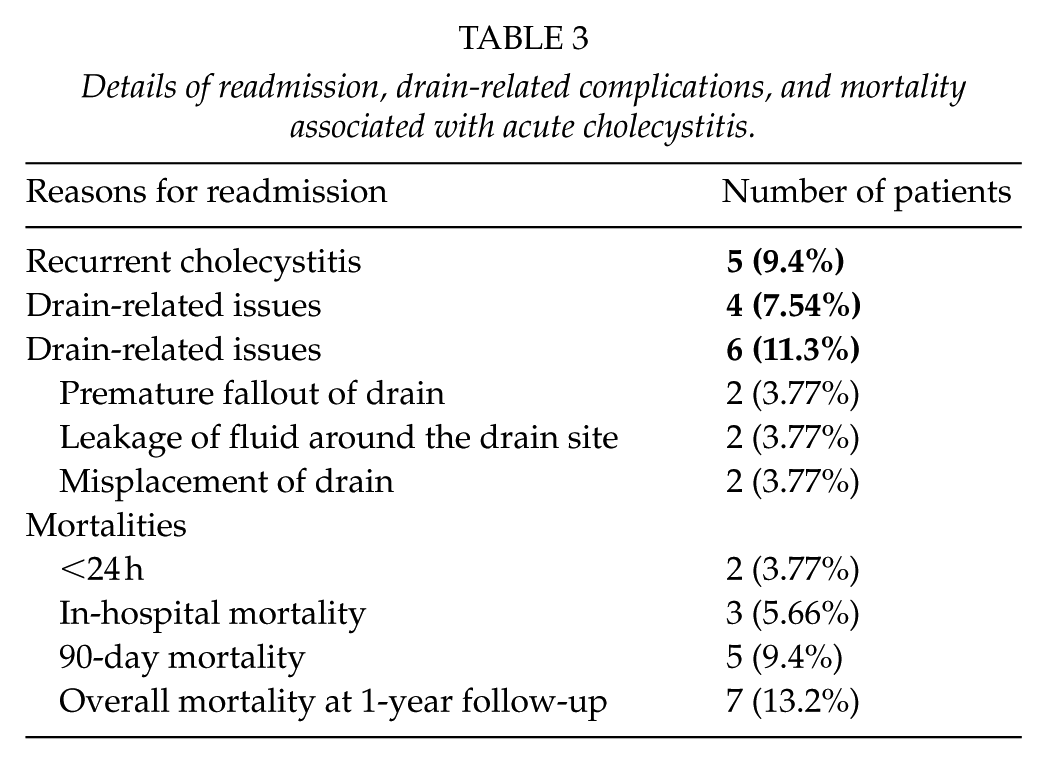
The overall mortality was 13.2% at 1-year follow-up. The details of mortality are described in Table 3. Three patients died prior to discharge from the hospital and two of these patients died within 24 h after PC and third patient died on day 21. All three patients died due to sepsis. The 90-day mortality was significantly higher in American Society of Anesthesiology (ASA) grade 4–5 group (17.8% vs 0%, p = 0.026) and in patients with ACC (23% vs 4.8%, p = 0.035). Mortality was also much higher in patients with ACC at 12 months; however, it was not statistically significant (23% vs 10%, p = 0.17).
A total of 24 (45.2%) patients had surgery: 7 within 6 weeks from the time of admission and 17 subsequently (details of surgery are described in Table 4). The median timing of cholecystectomy was 47 days (range, 4–346 days). The procedure was started laparoscopically in 16 and open in 8 patients. The laparoscopic operation was converted to open in 5 out of 16 patients (conversion rate 31%). The main reasons for conversion were adhesions in three, unclear anatomy in one, and technical difficulties due to perforated gallbladder in one patient. Eight patients underwent an open operation. Six underwent open cholecystectomy as a planned procedure. Two had laparotomy; one for peritonitis secondary to small bowel perforation, and the patient had closure of small bowel perforation along with partial cholecystectomy. The second patient had purulent fluid in peritoneal cavity with no obvious source of perforation, apart from diverticular disease.
Details of type of surgery.
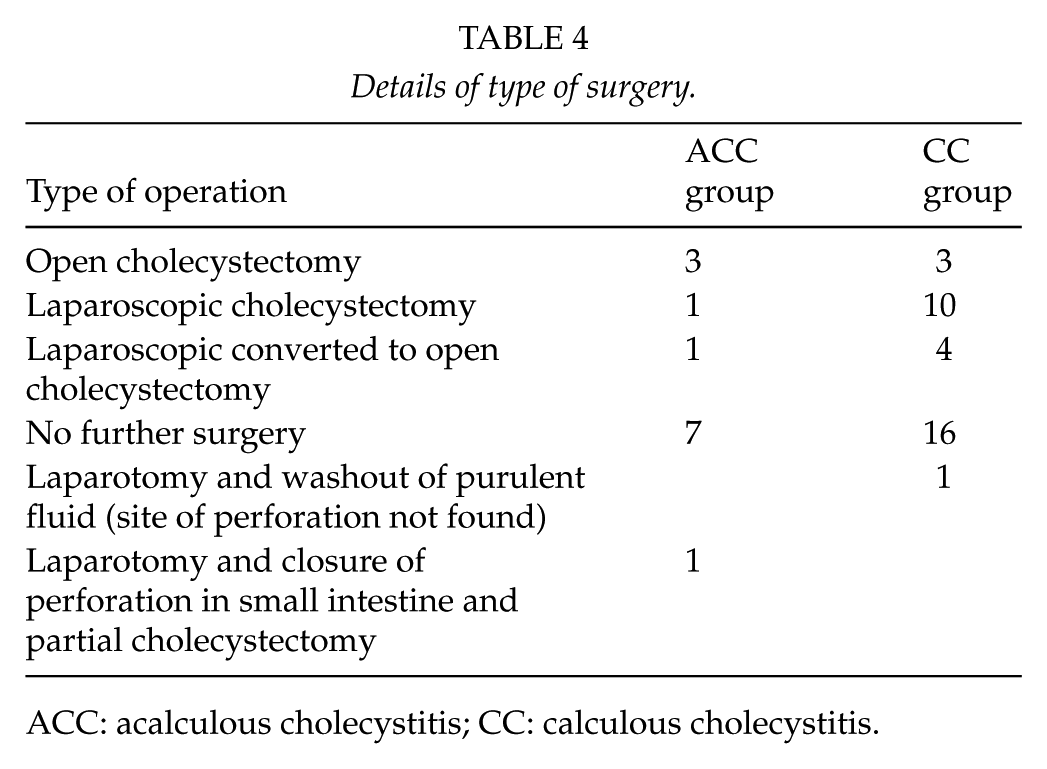
ACC: acalculous cholecystitis; CC: calculous cholecystitis.
Discussion
Current UK guidelines state that the definitive treatment for cholecystitis is laparoscopic cholecystectomy (9). However, this can be unsafe and not appropriate for patients who are unfit—either due to co-morbidities or them being too unwell for surgery (due to sepsis). Alternative life saving and less invasive treatment options are needed for patients in this category. One such treatment option is PC. Several studies have found that PC has favorable outcomes in the short term (10). However, its long-term role is still not clear, as there is conflicting evidence in terms of its benefits and associated risks of the procedure. Dimou et al. found that since the introduction of Tokyo guidelines, the use of PC has increased and the definite treatment with cholecystectomy has decreased. They also found that PC is associated with higher mortality and increased readmission rate (11).
We decided to evaluate the role of PC in our hospital, which serves a population of 450,000. In our study, the median age of patients undergoing PC was 74 years. Over half of these patients had multiple co-morbidities and were not fit for early laparoscopic cholecystectomy. Over 50% of patients in this series were ASA grade 4 and above at the time of diagnosis. These patients were at an increased risk of complications due to their co-morbidities and sepsis (3).
One of the main findings of our study was 94% survival to discharge. The overall mortality at 12-month follow-up was 13.2%. The overall 90-day mortality was significantly higher in ASA grade 4 and 5 groups compared to ASA grade 3 and less. Overall mortality was also higher in patients with ACC both at 90 days and at 1-year follow-up. The higher mortality in patients with ACC reflects the fact that these patients were much sicker due to their underlying illness, which was the predisposing factor for cholecystitis (12). Despite the fact that over 50% of patients were ASA grade 4 and 5, the majority of these patients survived, most likely due to successful PC. This supports the fact that PC can be a useful bridging procedure for future surgery and as the definitive procedure in selected group of patients.
Our overall mortality figures are significantly better compared to the similar studies published in the literature (13). In a systematic review on treatment of choice for ACC, Soria et al. observed that mortality among patients with ACC is 30%, and it is related to clinical severity and higher prevalence of gangrene (50%) and perforation (10%) (14). In our series, mortality was significantly higher in patients with ACC compared to AC, which we think is mainly due to underlying associated co-morbidities. PC may manage 85%–90% of patients with severe cholecystitis with success rates ranging from 56% to 100%. In a series of 57 patients with ACC, PC was successful in all and symptom remission occurred within 4 days in 93% of patients (15). A recent systematic review on the role of cholecystectomy concluded that PC may be the definitive treatment for high-risk patients for surgery (14). The overall morbidity associated with PC was 21%. In our series, drain and drain-related issues were observed in 11.3% of patients. There was no drain-related mortality; however, one patient had peritonitis secondary to small bowel perforation, which could be related to drain.
In our series, half of our patients were admitted under physicians with unknown source of infection. These patients were subsequently found to have cholecystitis on imaging. We noted that patients who had the longest time delay from admission to PC were under the care of the physicians. We do not know the exact reason for the delay, but it may be that these patients were initially treated with empirical antibiotics and when their condition did not improve, treating clinicians decided to investigate the patients with abdominal imaging after excluding another source of infection. It is also possible that the delays could also be due to the fact that some of these patients might have been admitted with issues related to their underlying co-morbidities and subsequently have developed AC. Whatever may be the reason for the delay, an increase in general awareness could lead to earlier intervention, which can lead to even better outcomes for these patients. We also recommend having local guidelines and an algorithm for management of patients with PC. Although we have no locally agreed guidance and an algorithm, we propose an algorithm that is described in Fig. 4.
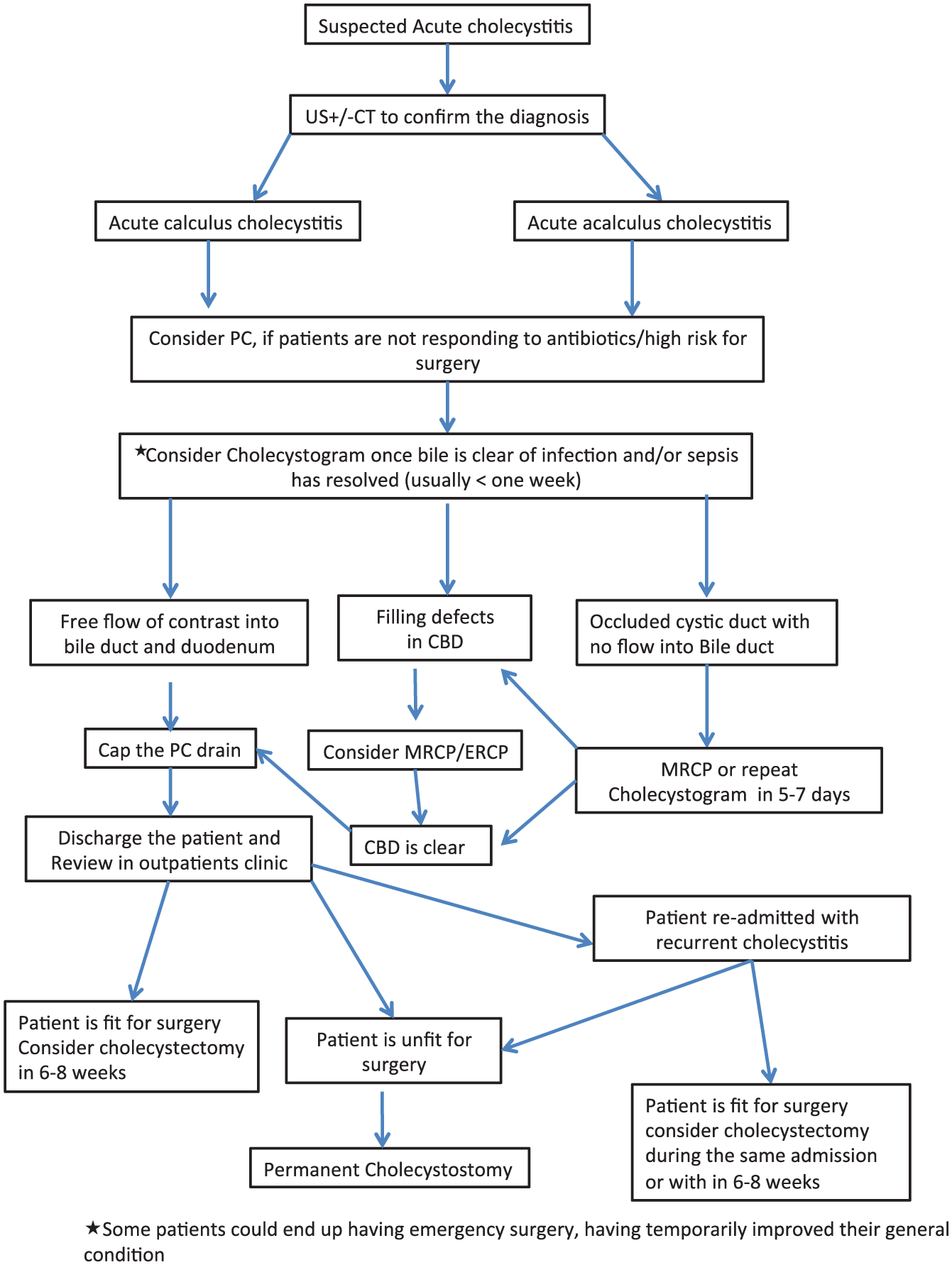
Management of patients with acute cholecystitis who are deemed unfit for surgery or too high risk for surgery.
Seven patients underwent cholecystectomy within 6 weeks after the insertion of PC and the rest during the subsequent weeks. The conversion rate to open cholecystectomy is over 30%, which was significantly higher compared to our institution rate of 5% (unpublished data) for elective/emergency laparoscopic cholecystectomy. However, our figures are similar to published literature (16). In a study by Simorov et al. (16), out of 1725 patients with ACC, 822 patients underwent laparoscopic cholecystectomy with a conversion rate of 26.5%. The most likely reasons for higher conversion rate were adhesions and unclear anatomy due to inflammation.
There are several limitations to our study and these are retrospective nature, small case series, and the inclusion of patients with acute CC and ACC. Acute CC and ACC are two entirely different diseases with different pathophysiology and outcomes. Patients with ACC are often elderly with several co-morbidities that often preclude surgery. This group of patients have higher mortality and also likely to end up with permanent drainage procedure. We should have evaluated these two groups of patients separately, but as the main aim of the study was to evaluate the early and late outcomes of PC, we decided to combine both groups.
With these limitations, we conclude that PC is a useful radiological procedure with good early and late outcomes. It should be considered either as a temporary bridging or as a permanent procedure in patients who are at high risk for surgery. We would also advocate raising awareness among non-surgical clinicians about PC as a form of sepsis control in patients who are unfit for surgery and not responding to antibiotics.
Footnotes
Acknowledgements
We would like to thank Mr Jacob Akoh, Consultant surgeon, for his expert advice and help with the preparation of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.