
Abstract
Background:
Rectal cancer surgery is standardized, resulting in improved survival. Colon cancer has fallen behind and therefore more radical surgical techniques have been introduced. One technique is complete mesocolic excision. The aim of this article was to study the complications after the introduction of standardized complete mesocolic excision in a single center.
Methods:
Complete mesocolic excision was introduced in 2007, and data were collected from 286 patients prior to surgery (2007–2010). The surgeon decided on open or laparoscopic surgery. Follow-up information was recorded until 31 December 2015. Complications were classified according to a modified Clavien–Dindo classification.
Results:
Complications occurred in 47%, severe complications (grade III and IV) in 15%. In-hospital mortality was 3.5%. A total of 142 patients (49.7%) were operated by open surgery. Logistic regression revealed anemia (p = 0.001), open surgery (p < 0.001), and long operating time (p < 0.001) as significant factors for complications in general. Multinomial logistic regression revealed that severe complications occurred more often in males (odds ratio: 2.56; 95% confidence interval: 0.98–6.68), patients with anemia (odds ratio: 3.49; 95% confidence interval: 1.27–9.60), elevated body mass index (odds ratio: 1.14; 95% confidence interval: 1.02–1.28), and in open surgery (odds ratio: 9.95; 95% confidence interval: 2.58–38.35). Age was not associated with severe complications. Survival was not significantly influenced by complications. Overall survival (5 years) was 90% among patients with complications and 92% among those without complications.
Conclusion:
Severe complications following the introduction of complete mesocolic excision are patient dependent and related to open surgery. Patients selected for laparoscopy had less number of complications; therefore, introducing complete mesocolic excision by laparoscopy is justified. Identification of these factors can improve selection of appropriate surgical approach and postoperative patient safety.
Keywords
Introduction
Oncological quality in colorectal cancer surgery depends on meticulous dissection of anatomic structures. Implementation of total mesorectal excision has improved outcome for patients with rectal cancer (1). A similar approach in colon cancer surgery has been developed and is described as complete mesocolic excision (CME) with central vascular ligation (CVL). This technique has been advocated by groups in Japan, Australia, Denmark, and Germany (2–4). Technical notes are outlined in the article by Hohenberger et al. (5) from 2009.
Standardized surgery based on these principles was introduced at Haraldsplass Deaconess Hospital in 2007. The implementation of CME has been associated with improved short-term survival (6). However, concern has been expressed for increased complication rates of CME (7). Available studies are few, and the definition and classification of complications varies considerably. A recent study by Bertelsen et al. (8) indicated that CME is associated with more severe complications. Complications matter because they contribute to morbidity, hospital stay, quality of life, and mortality. These factors may influence survival and must be taken into account when introducing a new procedure.
This article studies the implications of introducing CME regarding short-term complications and survival.
Methods
Between 2007 and 2010, 286 consecutive patients with colon cancer were included prospectively. Patients classified as not resectable (13 patients), either in staging pre-operatively by computed tomography (CT) scan or intra-operatively, were excluded, along with patients who underwent operations that were not in accordance with CME principles (35 patients). CME was introduced by visiting workshops in Erlangen and proctors from Germany and Japan during the first operations. Documentation of the technique was recorded in standardized drawings. Peri-and postoperative data were collected prospectively. All patients were operated with adherence to CME with CVL, with either open technique or laparoscopic approach. The open approach was always from lateral to medial, whereas the laparoscopic method was from medial to lateral. Standardized surgery stressed sharp dissections of mesocolic planes, with an intact fascia and a central tie. For right colectomies, CVL meant ligation of the ileocolic artery at the right side of the superior mesenteric vein (SMV) and division of the right branch of the middle colic artery. When extended right-sided resections were done, the middle colic artery was ligated at its origin. The lymphatic tissue around the SMV was not removed. On the left side for sigmoid resections, the inferior mesenteric artery was ligated close to its origin, proximally to the division of the left colic artery, sparing the sacral nerve plexuses. For tumors in the left flexure or left transverse colon, a subtotal resection or segmental resection was performed. No quality control of CME was carried out.
The operating surgeon decided if the patient was to undergo the operation by laparoscopy or by open technique. The decision to use an open or laparoscopic approach was based on the technical skills of the surgeon. The surgery was performed by four colorectal surgeons, one of whom mainly performed laparoscopy.
Initially, open surgery was chosen for advanced tumors and tumors located in the transverse colon, including the flexures. In both open surgery and laparoscopy, the anastomosis was end-to-end and hand sewn. For left-sided resections, the rectosigmoid was divided at the level of the promontory and the anastomosis was done by suture machine.
Anemia was defined according to World Health Organization (WHO) as hemoglobin (Hb) levels below 12.0 g/dL in non-pregnant women and below 13.0 g/dL in men. Complications were classified according to the Clavien–Dindo classification (9) and grouped as (a) no complications, (b) Clavien–Dindo Grade I–II, and (c) Clavien–Dindo Grade III–V.
After discharge, the patients were followed at the out-patient clinic, and variables such as adjuvant therapy, recurrence, surgery, cause of death, Hb levels, C-reactive protein (CRP), carcinoembryonic antigen (CEA), and weight were recorded every 6 months along with CT scans of abdomen and lungs. Follow-up information was recorded until 31 December 2015.
Statistical Analysis
Descriptive statistics are reported using the mean, standard deviation (SD), percentage, and range. The distributions of basic characteristics were compared between patients with and without complications, using Gosset’s unpaired t-test and the exact Pearson’s chi-square test. Simple and multiple binary logistic regression were used to explore the potential impact of risk variables on the risk of complications. The grades of complications (none, Clavien–Dindo I–II and Clavien–Dindo III–V) were analyzed using multinomial logistic regression. Results from unadjusted, fully adjusted, and a simplified final model were reported. The final model was determined by backward stepwise selection of variables from the fully adjusted model at a significance level of 0.05, and estimates were expressed using the odds ratio (OR) with 95% confidence interval (CI).
Anastomotic leakage was analyzed separately with unpaired t-test, chi-square test, and logistic regression. Overall survival (OS) and time to recurrence (TTR) were calculated. To analyze OS and TTR, we used the Kaplan–Meier method for unadjusted comparisons and Cox regression for adjusting for potential confounders (e.g. age and gender).
Generally, a p-value ⩽ 0.05 was considered significant. All analyses were performed using PASW SPSS 21–23.
Ethics
The Regional Committee for Medical Research Ethics of Western Norway and the Data Inspectorate for National Registries approved the study. All participants provided written informed consent. The study is part of a prospective project registered with clinicaltrials.gov (NCT00963352). The authors have no conflicts of interest.
Results
Patient Characteristics
A total of 334 consecutive patients were eligible for the study. A total of 48 patients were excluded (irresectable tumors (13) and patients with surgery not in accordance with CME principles (35)). Table 1 shows descriptive statistics of the patients. Around 34.6% of the patients had tumors located in the right colon, 7.3% in the right flexure, 15.4% in transverse colon, 1.7% in the left flexure, and 41% in the left/rectosigmoid colon. Around 48% had a right or an extended right hemicolectomy, 3% a segment resection of the transverse colon, 6% a left hemicolectomy, 35% a sigmoid/anterior resection, and 8% a combination. The majority of the patients had a pT3 cancer. One of the surgeons performed 42% of the operations, of which 85% were done laparoscopically.
Descriptive statistics for baseline and clinical variables regarding complications in 286 patients who underwent radical surgery for colon cancer in a Norwegian community teaching hospital during 2007–2010.
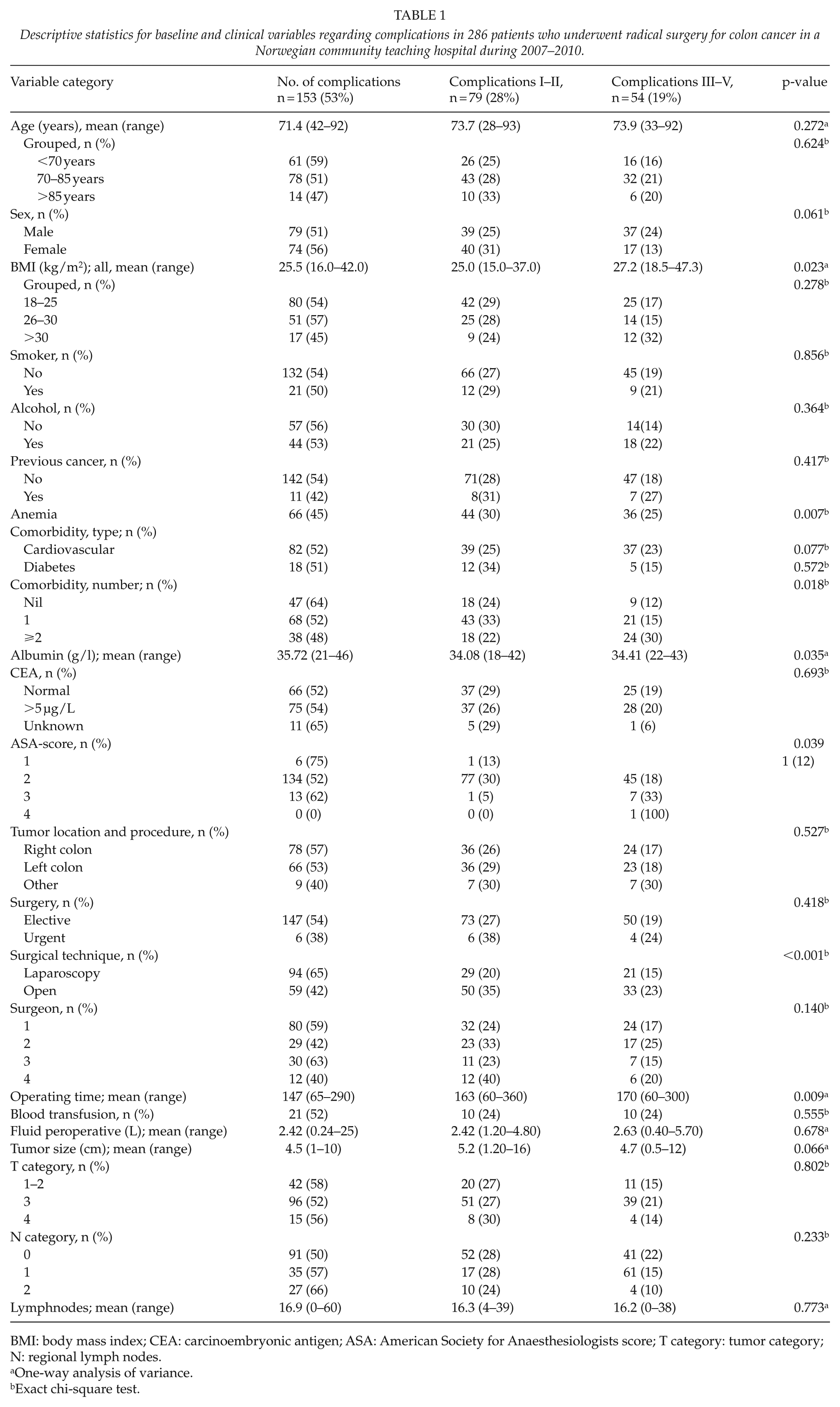
BMI: body mass index; CEA: carcinoembryonic antigen; ASA: American Society for Anaesthesiologists score; T category: tumor category; N: regional lymph nodes.
One-way analysis of variance.
Exact chi-square test.
Complications
Of the patients, 46.6% had complications. Grade I and II complications (minor complications not requiring surgical, endoscopic, or radiological intervention) were experienced by 27.6% of the patients, grade III and IV complications by 15.5%, and in-hospital mortality (ranging from 5 to 50 days) was 3.5% (grade V complications). Descriptive statistics for assorted variables associated with complications are shown in Table 1. These are body mass index (BMI), anemia, comorbidities, low preoperative albumin, the American Society for Anaesthesiologists (ASA)-score, open surgery, and operating time.
Logistic regression (Table 2) revealed anemia (p = 0.001), open surgery (p < 0.001), and long operating time (p < 0.001) as significant factors for complications in general. Elderly patients were not prone to more complications (p = 0.323).
Results from logistic regression analysis of complications in 286 patients who underwent radical surgery for colon cancer in a Norwegian community teaching hospital during 2007–2010.
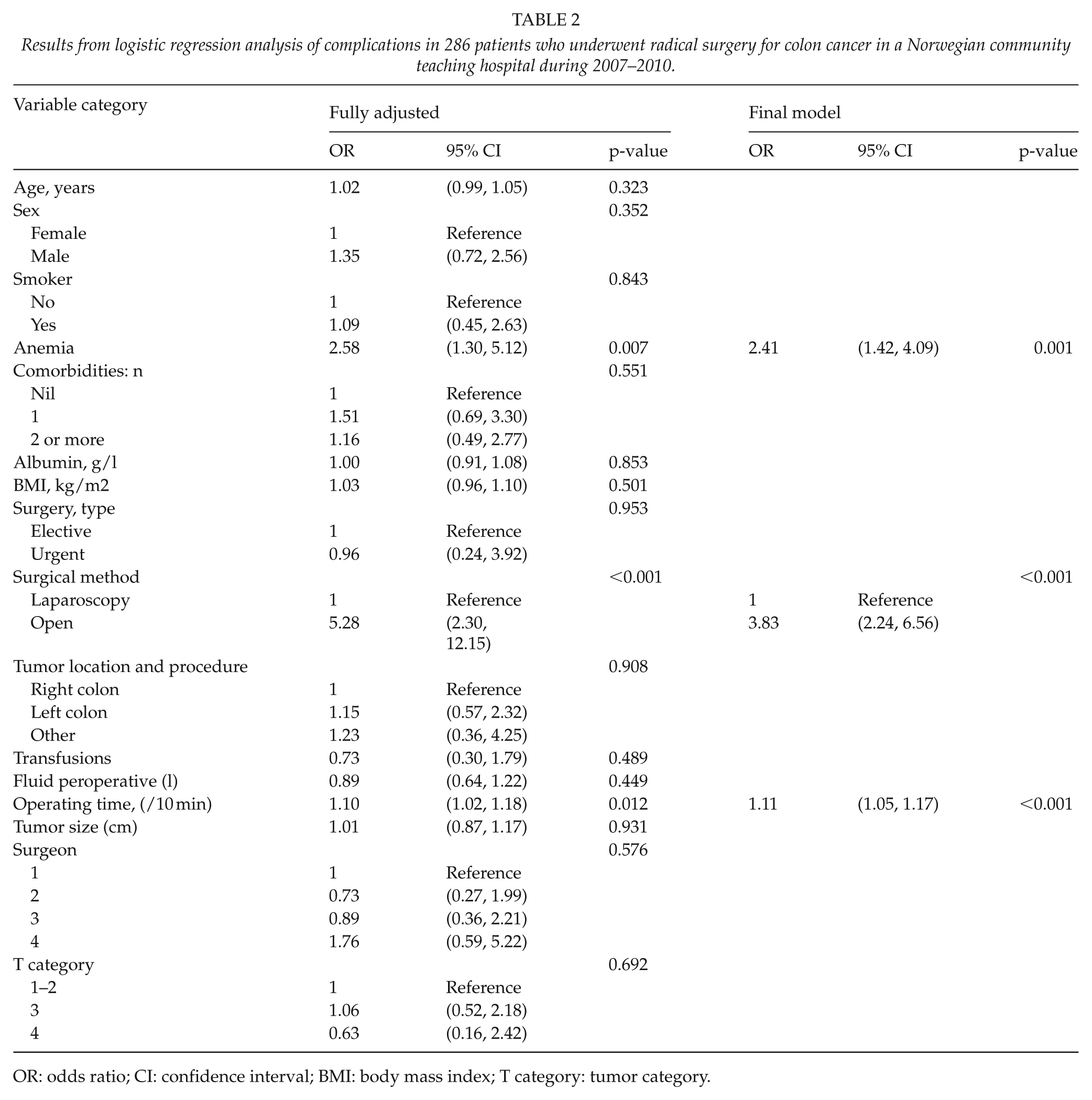
OR: odds ratio; CI: confidence interval; BMI: body mass index; T category: tumor category.
Complications were analyzed according to severity by multinomial logistic regression (Table 3). The characteristics significantly associated with severe complications (grade III–V) were male gender, elevated BMI, anemia, and open surgery. In the final model, the variables associated with severe complications were the same as those with grade I and II complications, that is, anemia (p = 0.001), long operating time (p < 0.001), and open surgery (p < 0.001). This was established by backward stepwise regression from the fully adjusted model.
Results from adjusted multinomial logistic regression of complications grade I–II and III–V vs no complications, in 286 patients who underwent radical surgery for colon cancer in a Norwegian community teaching hospital during 2007–2010.
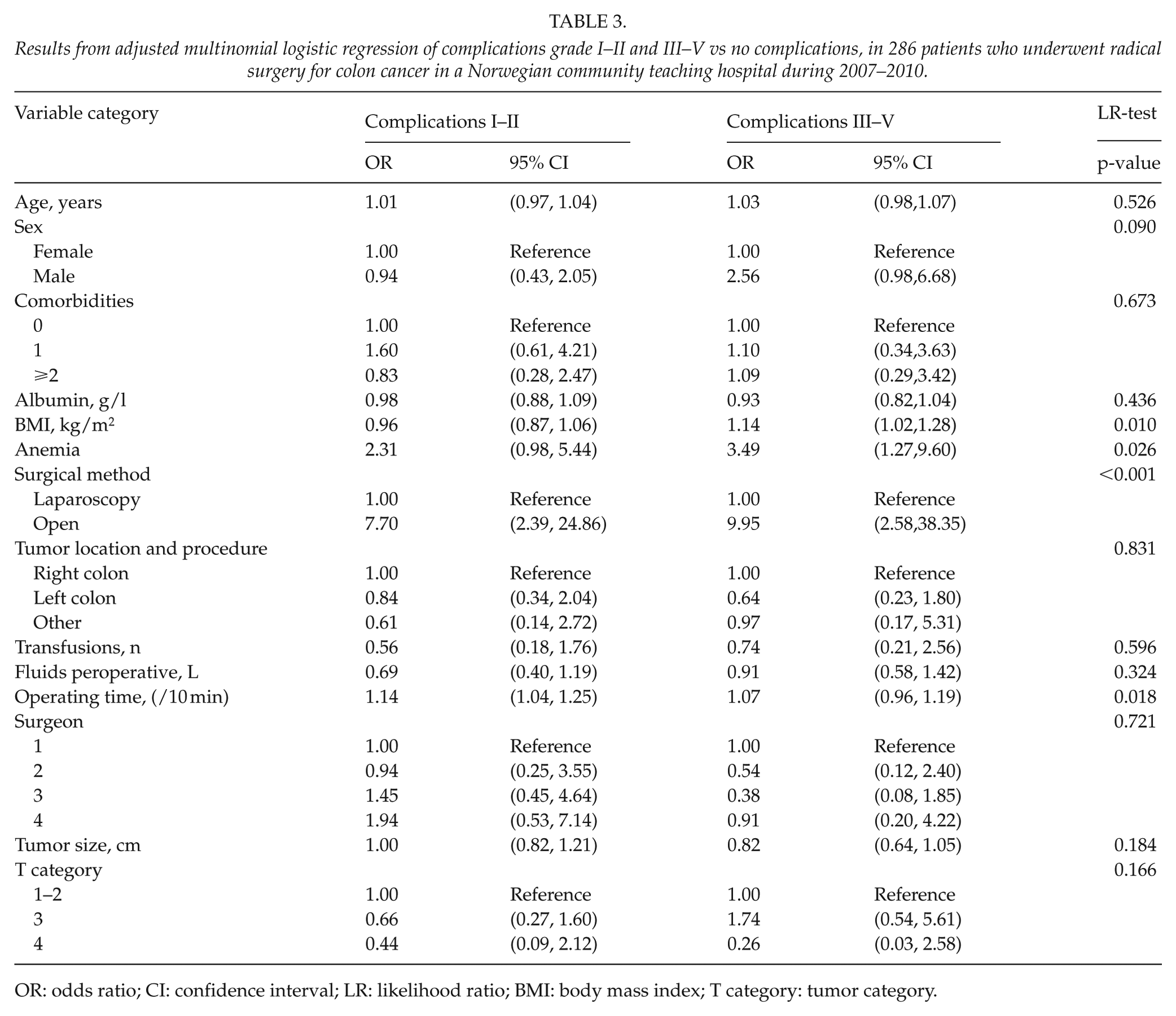
OR: odds ratio; CI: confidence interval; LR: likelihood ratio; BMI: body mass index; T category: tumor category.
Elevated CRP on the third postoperative day (mean): 237 (121.6) versus 135 (81.25) µg/L indicated anastomotic leakage (p < 0.001). The variables associated with leakage were elevated BMI, male gender, low albumin levels, and peroperative transfusions (data not shown, but analyzed separately with unpaired t-test, chi-square test, and logistic regression). The leakage rate was 8.4%.
The mean postoperative stay was 5.6 days (SD: 2.81; median: 5 days; range: 3–22) for patients without complications and 17.5 days (SD: 14.96; median: 12 days; range: 3–82) for patients with complications (p < 0.001). The mean postoperative stay was 11 days (SD:6.01; median 9 days; range: 4–38) for patients with grade I and II complications and 30.3 days (SD: 19.04; median:26; range 3–38) for patients with grade III and IV complications.
Oncological Outcome
The presence of complications was not a prognostic factor for OS or TTR when multivariate Cox regression analyses were done (p = 0.993 and p = 0.900, respectively).
Discussion
This article describes complications in a consecutive series of 286 patients operated for colon cancer following the introduction of CME and identifies risk factors for the development of complications.
Almost half of the patients in this study had complications (46.6%). We registered complications prospectively and used a modified Clavien–Dindo classification, where any deviation from a normal postoperative course was documented. This high complication rate is a result of this prospectively registration of complications. Most of our patients with complications experienced complications grade I–II (28%). Around 19% of the patients had complications grade III–IV. The literature reports complication rates or postoperative morbidity rates associated with CME surgery from 19% to 35% (8, 10–15). Reviews published for the last few years to evaluate the safety, quality, and effect of CME discuss the different ways of reporting complications and thus making comparisons difficult (16–20). Killeen et al. found an overall morbidity rate of 19.4%. The review from Kontovounisios et al. concluded that surgical risks and postoperative complications are not increased when doing CME. The review from Wang et al. (18) comments on the difficulties in comparing studies due to variations in defining and registration of complications but concludes with CME being associated with greater intraoperative blood loss and more postoperative surgical complications.
Other studies using the Clavien–Dindo classification, report grade I and II complications at 20% and grade III–IV at 4% (21). Siani et al. (22) described an overall complication rate of 35.5%. Almost 88.7% were Grade I and II, and 11.2% had grade III–IV complications.
In this study, risk factors for severe complications were male gender, anemia, and increased BMI. This is in line with other studies that showed an association between male gender and an increased risk of severe complications such as anastomotic leakage (23), preoperative anemia increased postoperative complications, and mortality (24) and obesity also led to increased complication rates (25). The ASA-score showed no association with morbidity or mortality. Age was also not found to be an independent risk factor for postoperative complications.
The mortality rate in our study was 3.5%. This is comparable to the literature (16, 19, 26). Half of the patients died from non-surgical complications. Among patients with surgical complication one had bleeding from the spleen, and the others had anastomotic leakage. We did not experience an increase in the risk of organ injury during surgery. Bertelsen et al. (8) found no significance for higher mortality associated with CME, but injury to other organs observed during resection was more common in the CME group.
In addition to patient-related parameters, surgical method (open surgery) was an important factor contributing to severe complications. Laparoscopy was associated with less severe complications. In other studies comparing open and laparoscopic CME, we can observe a similar trend (12, 14, 15). Studies that compare laparoscopic and open CME are quite few and diverse.
Prolonged operative time also increased the risk of complications. Other studies have shown complication rates increasing with operating time (27) but also recognizing that operative time is multifactorial and also reflect more complex cases. In our study, all resections of tumors in transverse colon and the flexures were initially performed as open surgery by one surgeon. Comparisons of patient outcome by hospital- or surgeon-related factors are controversial. Some studies indicate that the surgeon’s experience and volume influence outcome (28). In this study, there was no significant difference between complications and the surgeon (Table 2). Our findings indicate that prolonged operative time is related to inferior outcome and may reflect intraoperative complications or difficulties.
We also studied the impact of complications on long-term outcomes as studies have shown that postoperative complications are an independent prognostic factor regarding survival (14). We could not show that complications were a prognostic factor for OS or TTR. Similar findings have been shown by Siani et al. (22) and Wang et al. (12).
Our study has some limitations. There is no control group regarding complications without CME. The quality of CME was not evaluated as such, but as an indicator or surrogate of surgical technique, the number of lymph nodes harvested was significantly higher after the introduction of more radical surgery (29).
Analyzing the introduction of CME revealed a high number of complications. Male gender, anemia, increased BMI, and open surgery were associated with severe complications. Introducing CME is technically demanding and should be restricted to a limited number of surgeons to achieve a high caseload. The operative technique should be standardized thoroughly. In this study, patients selected for laparoscopic CME had fewer complications than open surgery, even in elderly patients. Our findings indicate that introducing CME by laparoscopy is justified.
Due to the high number of complications and the potential risk for patients, risk factors should be identified prior to surgery and complications should be monitored carefully during the introduction of CME.
Footnotes
Acknowledgements
The authors gratefully acknowledge the contribution of the late Professor Søndenaa to this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.