
Abstract
Aims:
Wound closure after thyroidectomy and parathyroidectomy is associated with patients’ satisfaction, perception of cosmetic appearance, and experience of postoperative pain. Subcutaneous sutures, clips, and tissue adhesive are the three major methods of wound closure. In this study, we conducted a meta-analysis of randomized controlled trials to evaluate the outcomes of these methods.
Methods:
Relevant studies published before December 2017 were identified from PubMed, Embase, Cochrane Library, Scopus, and the ClinicalTrials.gov registry. Individual effect sizes were standardized, and a meta-analysis was conducted to calculate the pooled effect size by using random-effect models. The primary outcome was the cosmetic appearance, which was evaluated 4 weeks, 6 weeks, and 6 months after surgery. The secondary outcomes were patient satisfaction, postoperative pain, and complications.
Results:
A total of nine trials with 612 patients were reviewed. No significant difference was observed in patient satisfaction, postoperative pain, and complications among the wound closure methods. However, according to surgeon assessment, the subcutaneous suture method resulted in a significantly more favorable cosmetic appearance than the clip method (mean difference: −1.47, 95% confidence interval: −2.72 to −0.23).
Conclusion:
In the current study, no differences were found in patient satisfaction and postoperative pain among the subcutaneous suture, clip, and tissue adhesive wound closure methods. However, surgeons provided a more favorable appraisal for the subcutaneous suture method because of the improved cosmetic appearance. The choice of the closure method should be based on surgeon’s preference and cost.
Keywords
Introduction
Thyroidectomy and parathyroidectomy are common neck incision surgeries for patients with nodules suspected for malignancy, papillary thyroid cancer, multinodular goiter, symptomatic goiter, hyperthyroidism, or primary hyperparathyroidism (1). Because thyroid diseases are relatively common among young women and the incision sites are normally uncovered by clothing, the cosmetic outcome is a concern in the surgical procedures. Generally, three methods are commonly applied for wound closure, as follows: conventional subcutaneous sutures, surgical clips or staples, and tissue adhesive. Subcutaneous sutures are widely applied because of the benefits such as less tissue reaction and the absence of mark points (2). Compared with subcutaneous sutures, surgical clips or staples cause less tissue damage and require shorter wound closure time (3–6). Tissue adhesive, such as 2-octylcyanoacrylate, is supplied as monomer in liquid form that polymerizes on contact with tissue anions, forming a strong bond that holds the opposed wound edges together (7). Moreover, tissue adhesive has higher flexibility and breaking strength than clips or sutures do (8).
In addition to varying cosmetic outcomes, the wound closure methods cause different levels of postoperative pain. The patient’s general satisfaction and perception are essential for choosing a suitable wound closure method. Several randomized controlled trials (RCTs) have compared the wound outcomes of the subcutaneous suture, clip, and tissue adhesive methods (9, 10). However, there is no conclusion on which method is better in the aspects of cosmetic outcome, level of pain, patient satisfaction, and complications. Therefore, we conducted a systematic review and meta-analysis to compare the outcomes of the subcutaneous suture, clip, and tissue adhesive methods of wound closure in patients undergoing thyroidectomy or parathyroidectomy.
Materials and methods
Inclusion criteria
RCTs comparing the outcomes of the subcutaneous suture, clip, and tissue adhesive methods in patients undergoing thyroidectomy or parathyroidectomy were included in this review. Studies were also required to clearly report the inclusion and exclusion criteria for patients, the surgical technique, and the definitions and evaluation methods of cosmetic appearance, patient satisfaction, postoperative pain, and complications. We excluded trials that met at least one of the following criteria: (a) pediatric patients; (b) patients with concomitant conditions that might influence wound healing, such as neoadjuvant chemotherapy, immunosuppression, or allergies to adhesive tape; and (c) overlap of authors, centers, or patient cohorts in two or more studies.
Search Strategy and Study Selection
Relevant studies published before December 2017 were identified from the databases of PubMed, Embase, Scopus, and Cochrane Library. The following Medical Subject Headings were used: (thyroid OR parathyroid) AND (surgery OR excision OR resection), (thyroidectomy OR parathyroidectomy OR head and neck incision) AND (tissue adhesive OR adhesive strip OR octyl-2-cyanoacrylate adhesive OR synthetic glue OR tissue glue OR octylcyanoacrylate tissue adhesive OR tissue adhesion), (subcuticular suture OR suture OR subcuticular closure OR subcutaneous suture), OR (staples OR clips). The “related articles” option in PubMed was used to broaden the search, and all abstracts, studies, and citations retrieved were reviewed. In addition, we identified other studies by using the reference sections of relevant papers and by corresponding with subject experts. Finally, unpublished studies were collected from the ClinicalTrials.gov registry (http://clinicaltrials.gov/). No language restrictions were applied. The systematic review described herein has been accepted by PROSPERO, an online international prospective register of systematic reviews curated by the National Institute for Health Research (CRD42016053856).
Data Extraction
Baseline and outcome data were independently retrieved by two reviewers (Y.-H.H. and C.C.), and the study designs, study population characteristics, inclusion and exclusion criteria, surgical techniques, cosmetic appearance, patient satisfaction, postoperative pain assessment, and complications were extracted. Decisions recorded individually by the reviewers were compared, and disagreements were resolved by a third reviewer (K.-W.T.). The authors of the studies were contacted for additional information.
Appraisal of Methodological Quality
Two reviewers (Y.-H.H. and C.C.) independently assessed the methodological quality of each study by using the risk of bias method recommended by the Cochrane Collaboration (11). Several domains were assessed, including the adequacy of randomization, allocation concealment, outcome assessor blinding to patient information, follow-up duration, information provided to participants regarding study withdrawal, whether intention-to-treat analysis was performed, and freedom from other biases.
Outcomes
The primary outcome was the cosmetic appearance, which was evaluated 4 weeks, 6 weeks, and 6 months after surgery. The secondary outcomes were patient satisfaction, postoperative pain, and complications, including infection, seroma, and wound dehiscence.
Statistical Analyses
Data were entered into and analyzed using the Review Manager, Version 5.3 (The Cochrane Collaboration, Oxford, England). Meta-analysis was performed following the Preferred Reporting Items for Sysmetaic Reviews and Meta-Analyses (PRISMA) guidelines (12). Standard deviations were estimated from the provided confidence interval (CI) limits or the standard error. Dichotomous outcomes were analyzed by using risk ratios (RRs) as the summary statistic. The effect sizes of continuous outcomes were reported as the weighted mean difference (WMD). The precision of the effect sizes was reported as 95% CIs. A pooled estimate of the RR and WMD was computed using the DerSimonian and Laird random-effect models (13).
Statistical heterogeneity and the inconsistency of treatment effects across studies were evaluated using Cochrane Q tests and I2 statistics, respectively. Statistical significance was set at p < 0.10 for Cochrane Q tests. Statistical heterogeneity across studies was assessed using the I2 test, which quantifies the proportion of the total outcome variability across the studies. Moreover, subgroup analyses were performed by pooling available estimates for similar subsets of patients across trials.
Results
Trial characteristics
Fig. 1 illustrates the flowchart of trial screening and selection. The initial search yielded 335 citations, of which 291 were ineligible based on the criteria used for screening titles and abstracts. Thus, the full texts of 44 studies were retrieved. However, most of these studies were excluded from our final review because of the following reasons: 32 used different interventions, 2 were review articles, and 5 were not randomized. Thus, nine studies were eligible for inclusion in this study (9, 10, 14–20).
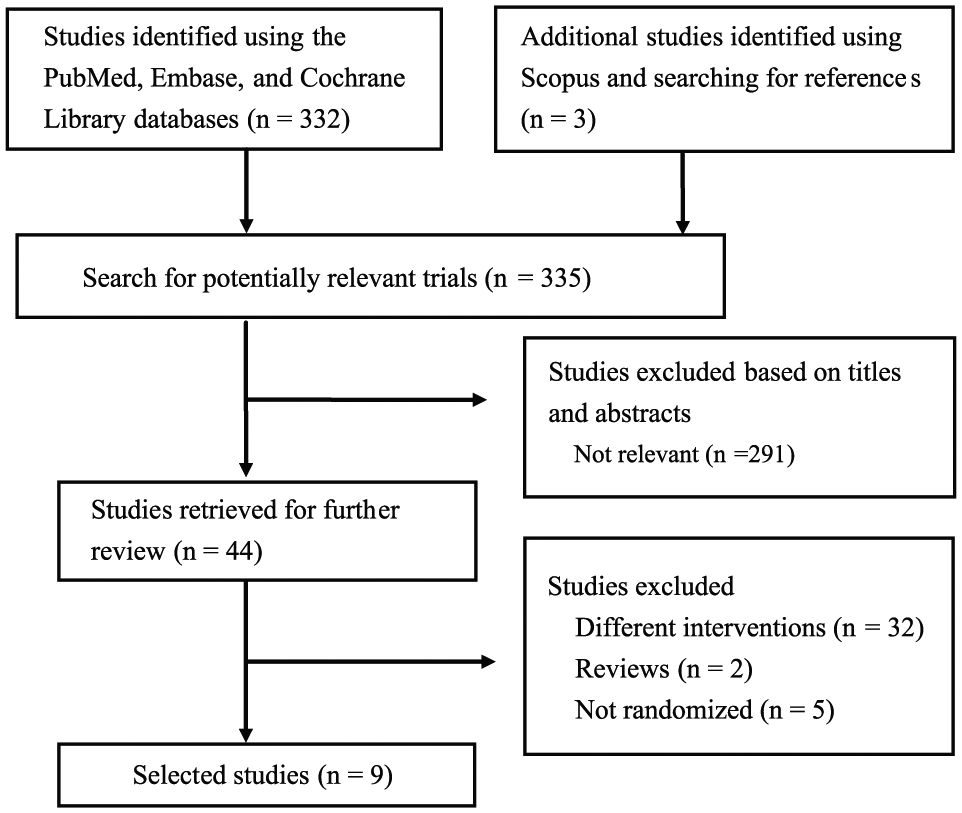
Flowchart of study selection.
These nine trials were published between 1994 and 2016, and have sample sizes ranging from 20 to 132. Four trials recruited patients undergoing thyroidectomy or parathyroidectomy (9, 14–16). Four trials recruited patients undergoing thyroidectomy (17–20). One trial recruited patients undergoing head and neck surgeries other than thyroidectomy (10). Minimally invasive thyroid surgery was performed in one trial (17). Four trials compared the outcomes of the tissue adhesive and clip methods (15, 17, 19, 20), two compared the outcomes of the clip and subcutaneous suture methods (16, 18), and three compared the outcomes of the tissue adhesive with subcutaneous suture methods (9, 10, 14). The approximation of the strap muscles and the reconstruction of the platysma were achieved in the same way in all groups, with the use of interrupted absorbable stitches. The use of perioperative prophylactic antibiotics was not mentioned in all trials. All nine trials evaluated the cosmetic appearance. Three trials evaluated patient satisfaction (17, 19, 20), whereas five trials evaluated the levels of postoperative pain among different wound closure methods (14, 16, 17, 19, 20). Baseline patient characteristics in the nine included RCTs were balanced (Table 1).
Characteristics of included randomized controlled trials.
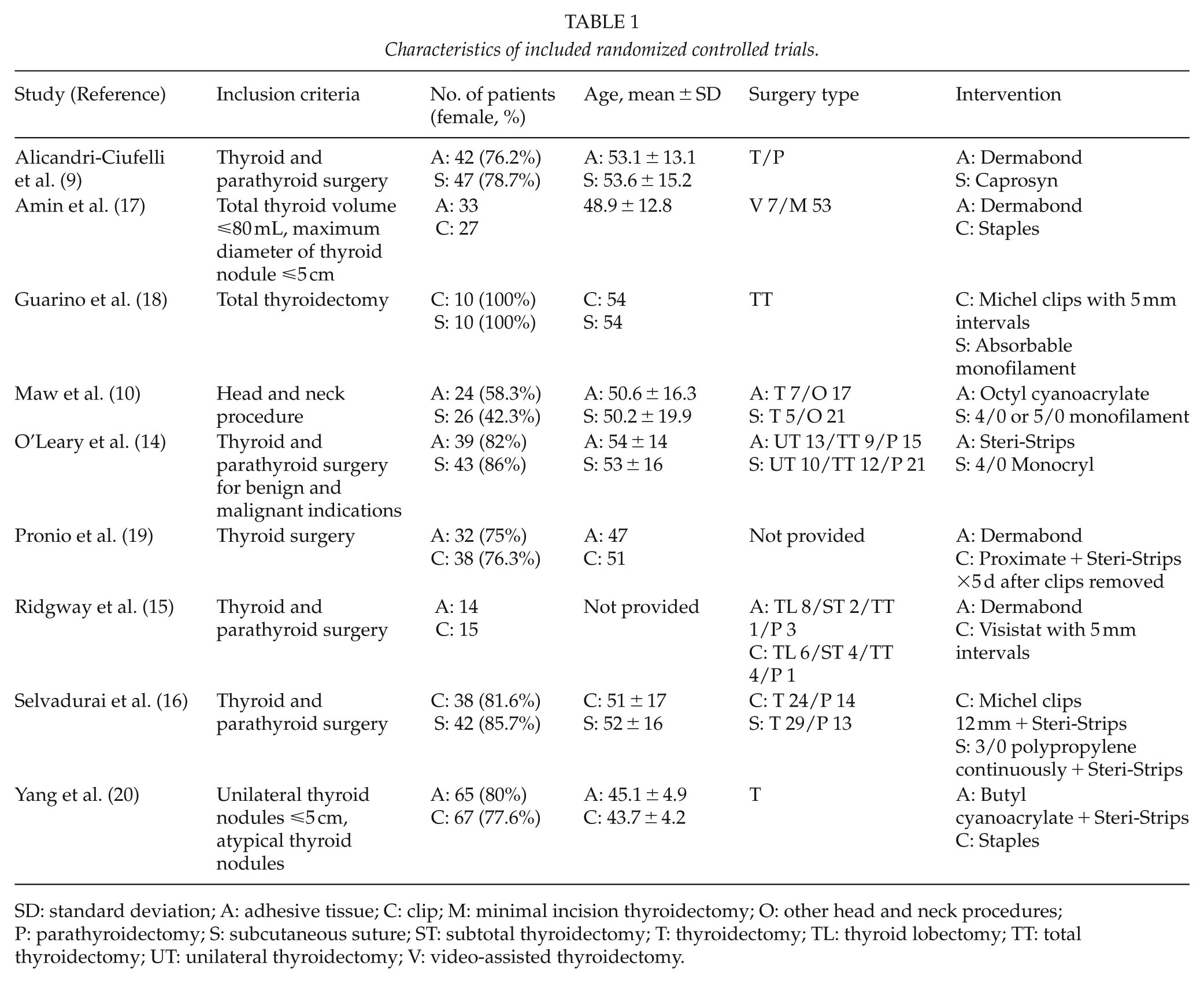
SD: standard deviation; A: adhesive tissue; C: clip; M: minimal incision thyroidectomy; O: other head and neck procedures; P: parathyroidectomy; S: subcutaneous suture; ST: subtotal thyroidectomy; T: thyroidectomy; TL: thyroid lobectomy; TT: total thyroidectomy; UT: unilateral thyroidectomy; V: video-assisted thyroidectomy.
The methodological quality of the included trials is summarized in Table 2. Nine studies reported acceptable methods of randomization. Outcome assessors were not blinded to patient information in three studies (10, 18, 19). Three studies used intention-to-treat analysis (3, 4, 6), whereas the other six used per-protocol analysis. The number of patients lost to follow-up was acceptable (<20%) in all trials, except for that in the trial by Alicandri-Ciufelli et al. (9). Other biases included the lack of patient characteristics (15, 17) and the lack of a standardized surgical process, with two different wound closure procedures performed by two surgeons (15).
Methodological quality assessment of included trials.
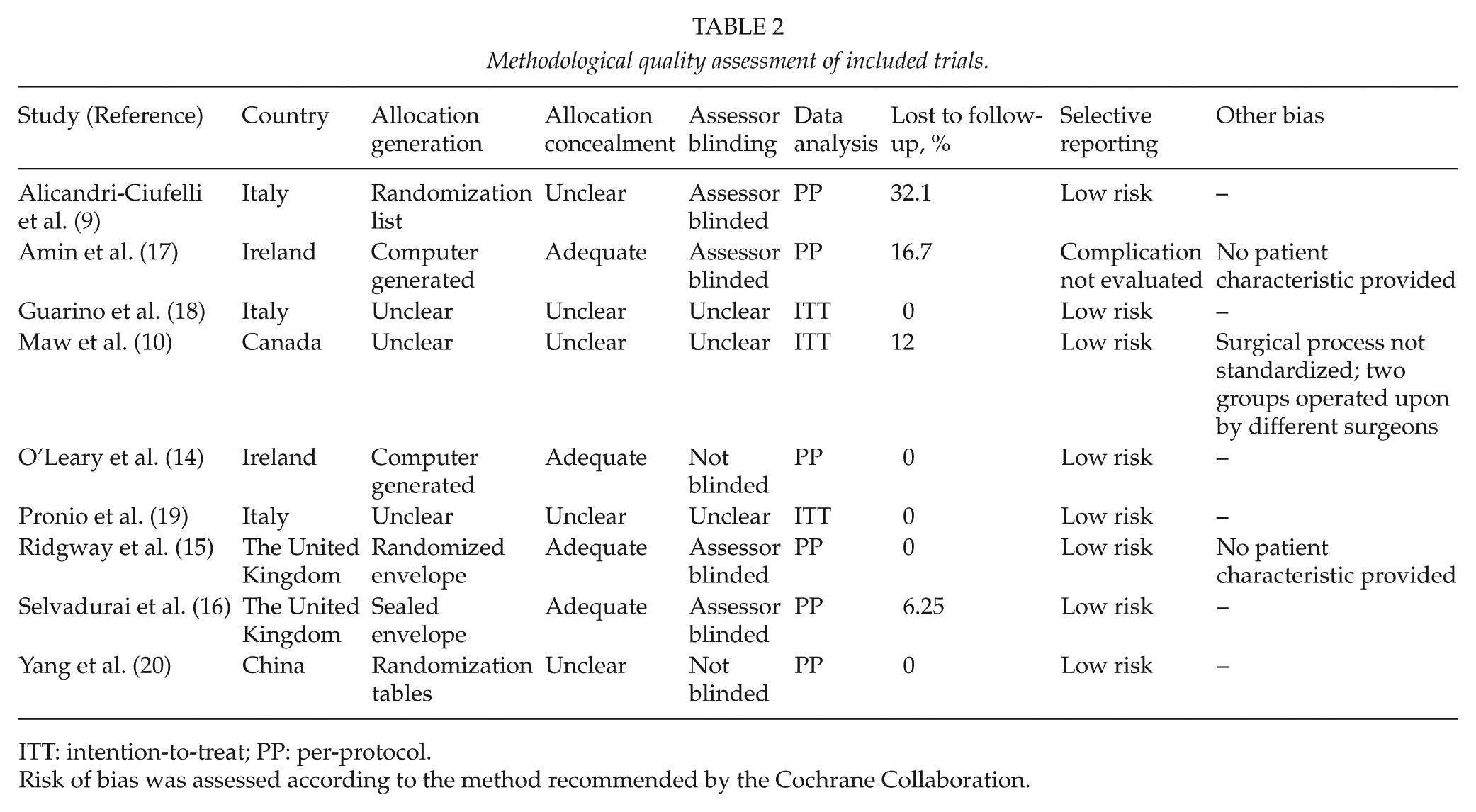
ITT: intention-to-treat; PP: per-protocol.
Risk of bias was assessed according to the method recommended by the Cochrane Collaboration.
Cosmetic Appearance
Four trials compared the cosmetic outcome of the tissue adhesive and clip methods (15, 17, 19, 20). Ridgway et al. (15) and Yang et al. (20) assessed the cosmetic appearance by using the 10-cm visual analog scale (VAS). Pronio et al. (19) assessed this outcome by using a verbal response with a numerical scale (9–10 = excellent, 7–8 = good, 5–6 = mild, and 0–4 = poor), and Amin et al. used the Manchester scar assessment tool (17). Because Yang et al. assessed the cosmetic appearance with rating in opposite directions, the results were converted to the same direction as those of Ridgway et al. Outcomes over 4 to 6 weeks after surgery were compared. The results of Amin et al. (17) (which only reported p values and provided no additional data) and Pronio et al. (19) (used the numerical scale) were not comparable and were thus excluded from our meta-analysis. Although the tissue adhesive group appeared to have a more favorable cosmetic outcome than the clip group, the trend was not statistically significant (mean difference: 1.80, 95% CI: −0.62 to 4.22; Fig. 2). Moreover, Amin et al. (17) reported no significant difference in the cosmetic outcome between the two groups at 3 months after surgery (p = 0.443). Pronio et al. (19) reported a more favorable cosmetic appearance in the clip group than in the tissue adhesive group at 7 days after surgery (p < 0.05), but not at 15 days, 1 month, 3 months, 6 months, and 12 months after surgery.
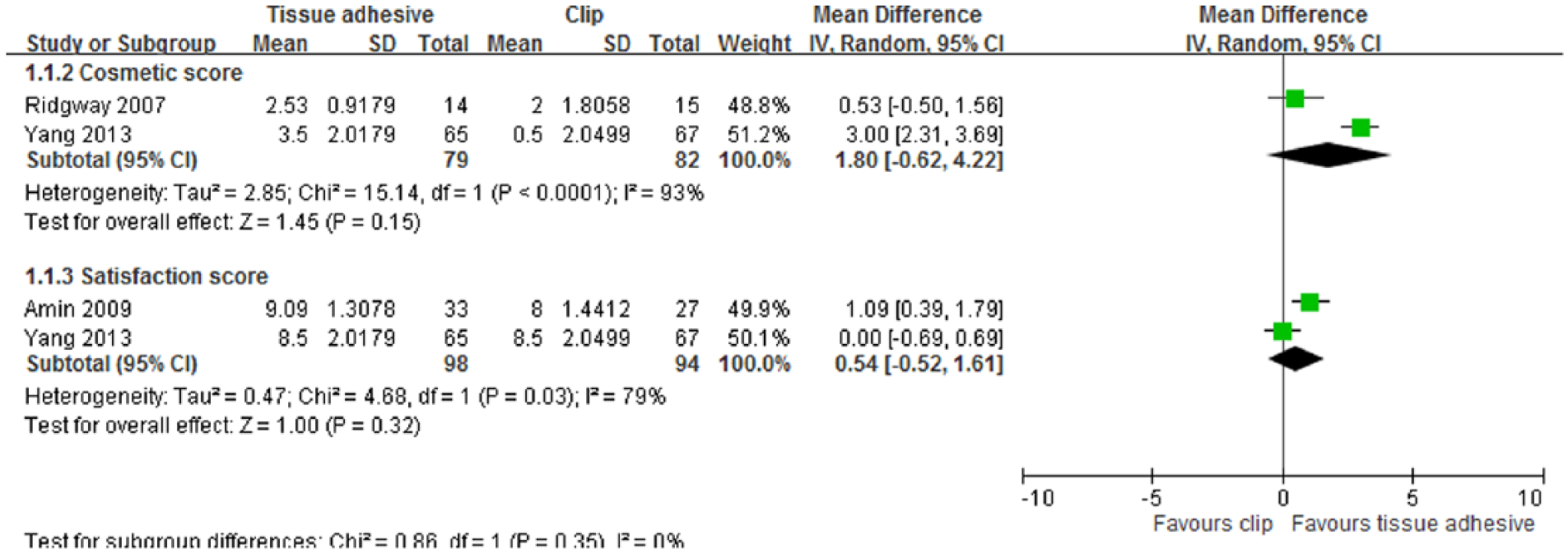
Forest plot of comparison of cosmetic score at 4 to 6 weeks after surgery and patient satisfaction score at 3 months after surgery between tissue adhesive and clip groups.
Two trials compared cosmetic outcomes between the clip and subcutaneous suture closure groups (16, 18). Guarino et al. (18) assessed cosmetic appearance by using the 10-cm VAS, and Selvadurai (16) used verbal response and the 100-mm VAS for assessments. In both trials, cosmetic appearance was assessed by the patient, surgeon, and independent assessor at 3 months (16) and 6 months (16, 18) after surgery. The 100-mm VAS results of Selvadurai et al. were converted into the 10-cm format to enable comparison with the those of Guarino et al., and the results at 6 months were compared. Surgeon assessment revealed that the subcutaneous suture group exhibited a significantly more favorable cosmetic outcome than the clip group (mean difference: −1.47, 95% CI: −2.72 to −0.23). Patient (mean difference: −0.16, 95% CI: −1.38 to 1.07) and independent assessor (mean difference: −0.68, 95% CI: −1.85 to 0.49) assessments revealed no significant differences between the two groups (Fig. 3).
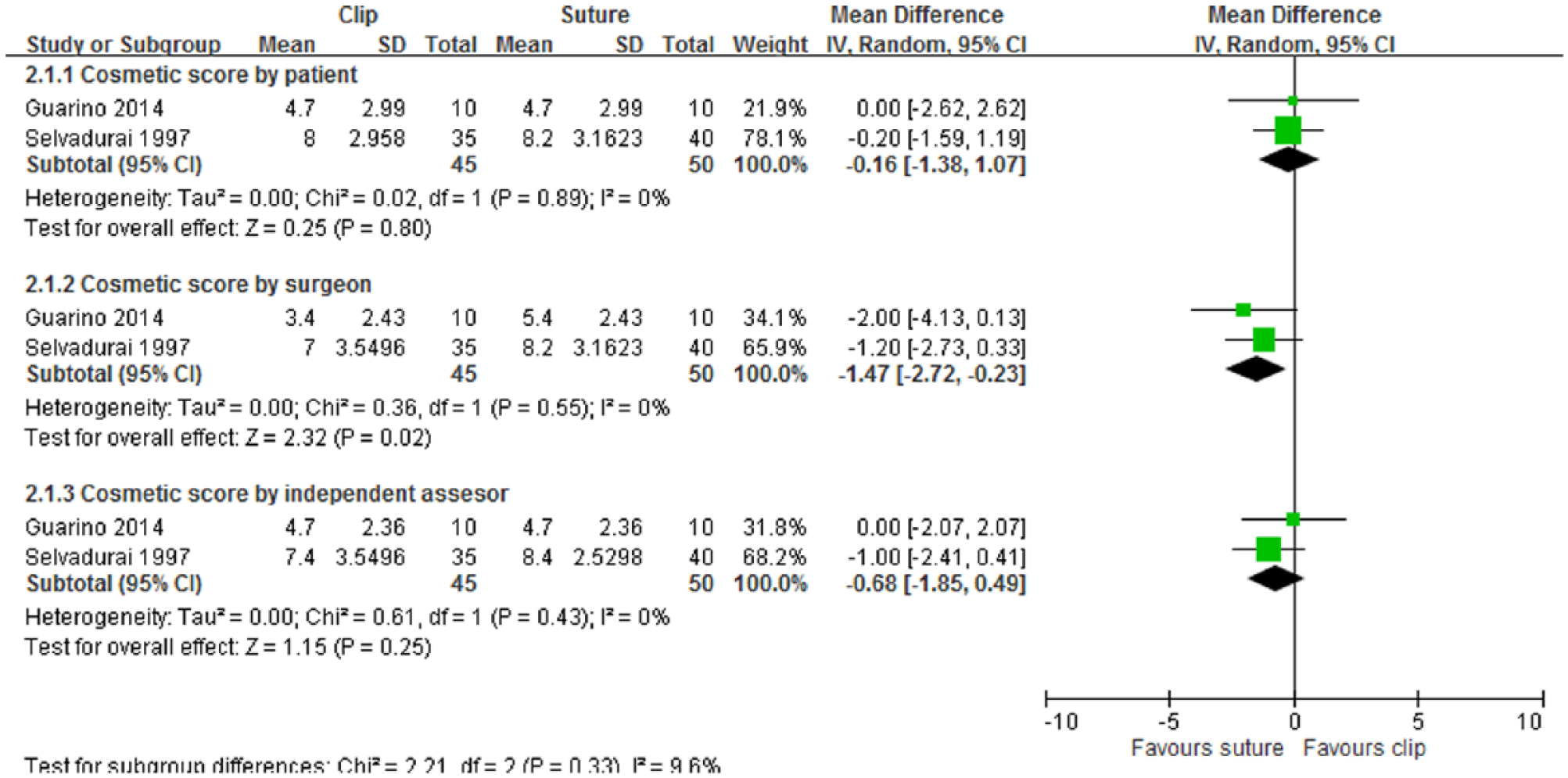
Forest plot of comparison of cosmetic score by the patient, physician, and independent assessor 6 months after surgery between clip and subcutaneous suture groups.
Two trials compared cosmetic appearance between the tissue adhesive and subcutaneous suture groups (9, 10). Alicandri-Ciufelli et al. assessed cosmetic appearance by using the 6-point Wound Registry Scale on day 10 after surgery and the 5-point Stony Brook Scar Evaluation Scale at 3 months after surgery (9). The suture group exhibited a significantly more favorable cosmetic outcome than the tissue adhesive group at 10 days (2.9 versus 1.4, p = 0.002), but the difference disappeared at 3 months (2.8 versus 3.1, p = 0.62) (9). Maw et al. assessed cosmetic outcome by using the 100-mm VAS and the Hollander Wound Evaluation Scale at 4 to 6 weeks after surgery and found no statistical differences between the groups (VAS: 58.7 versus 53.2, p = 0.44; Hollander Wound Evaluation Scale: 56.5% versus 50.0%, p = 0.67) (10).
Patient Satisfaction
Three trials compared patient satisfaction between the tissue adhesive and clip groups (17, 19, 20). The assessment tools were the 10-cm VAS in two trials (17, 20) and the verbal rating response in one trial (19). The measurement time points of these studies ranged from 1 to 3 months after surgery. Only the results of Amin et al. (17) and Yang et al. (20) were included in the meta-analysis, because the verbal rating response used by Pronio et al. (19) was not comparable to the VAS. No significant difference was observed between the two groups at 3 months after surgery (mean difference: 0.54, 95% CI: −0.52 to 1.61; Fig. 2). Pronio et al. (19) reported higher patient satisfaction in the tissue adhesive group than in the clip group (p < 0.001) at 7 days after surgery, and no further follow-up data were provided.
No comparisons of patient satisfaction between the tissue adhesive and subcutaneous suture groups or between the clip and subcutaneous suture groups were conducted.
Postoperative Pain Assessment
Yang et al. assessed postoperative pain between the tissue adhesive and clip groups by using the 10-cm VAS (20). Pronio et al. (19) reported only the number of patients who experienced pain, and Amin et al. (17) did not describe the assessment method for pain. These trials measured pain at different time points. Because of the different data formats of these studies, no comparison was conducted. Amin et al. (17) reported no significant difference in the pain level at 1 day (p = 0.829) and 10 days (p = 0.931) after surgery. Similar findings were reported by Pronio et al. (19) for the pain level at 15 days, 1 month, 3 months, 6 months, and 12 months after surgery. By contrast, Yang et al. (20) reported a lower pain level in the tissue adhesive group than in the clip group at 1 day after surgery (p < 0.001).
Postoperative pain between the clip and subcutaneous suture groups was assessed using the verbal response and the 100-mm VAS at 1, 2, and 3 days after surgery in one trial (16). No statistically significant differences were observed in the VAS- (p value of VAS on days 1, 2, and 3 = 0.71, 0.35, and 0.65, respectively) or verbal-response-measured postoperative pain (p value of verbal response on days 1, 2, and 3 = 0.658, 1.000, and 0.664, respectively) between the two groups.
No comparison of postoperative pain between the tissue adhesive and subcutaneous suture groups was conducted.
Complications
One trial compared complications between the tissue adhesive and clip groups after surgery (19). No between-group difference was observed immediately after closure and 7 days after surgery, but a higher incidence of edema was found in the tissue adhesive group than in the clip group (25% versus 5.2%, p < 0.05) at 7 days after surgery. Similarly, no between-group difference was observed at 15 days and 1 month after surgery; however, a higher incidence of edema was found in the tissue adhesive group than in the clip group (15 days: 25% versus 5.2%, p < 0.05; 1 month: 28.1% versus 5.2%, p < 0.01). No differences were observed at 3, 6, and 12 months after surgery.
One trial compared complications between the tissue adhesive and subcutaneous suture groups after surgery (14). No difference was observed in the overall complication rate (9% versus 6%, p = 0.668). Two patients in suture group and one patient in tissue adhesive group had superficial wound infections. One patient developed seroma in the tissue adhesive group, and one patient developed a rash around the wound in the suture group.
No comparison of complications between clip and subcutaneous suture was conducted.
Discussion
The main finding of the current meta-analysis is that no significant difference was observed in patient satisfaction, postoperative pain, and complications among the wound closure methods. However, the subcutaneous suture group showed a significantly more favorable cosmetic appearance than the clip group according to surgeon assessment. The tissue adhesive group appeared to have a more favorable cosmetic result than the clip group at 4 to 6 weeks after surgery, although the differences were not statistically significant.
Previous systematic reviews found no significant difference in the cosmetic outcome, development of wound infection, pain, and dehiscence between the tissue adhesive and other closure methods—namely, subcutaneous sutures and clips—used for the closure of simple traumatic lacerations and certain small-length incisions (21, 22). Moreover, Figueroa et al. (23) enrolled 398 patients and reported no difference in postoperative pain, cosmesis, or patient satisfaction between the clip and subcutaneous suture methods for the closure of the Pfannenstiel incision. The aforementioned results are similar to our main finding.
The wound closure time is another concern considered in the choice of the wound closure method. In the RCT by Maw et al. (10), wound closure through the tissue adhesive method took much less time (27.9 s) than that through the subcutaneous suture method (289 s). Selvadurai et al. (16) found no significant difference in wound closure time between the clip (270 s) and subcutaneous suture groups (288 s). However, such a time difference is not a crucial concern for experienced surgeons, operation shift managers, or hospital administration.
The trials included in our study exhibited considerable heterogeneity because of various clinical factors. First, surgical techniques were not the same across all trials. Second, although the surgeries were limited to the thyroid or parathyroid, the surgical types varied among the trials. Third, postoperative care was not standardized. Finally, the time points of outcome evaluation differed in some trials. Such differences among studies resulted in heterogeneity.
This study has several limitations. First, some trials had a small sample size of 10 per treatment group (16). Second, it was not possible for surgeons to be blinded in these trials. Third, some outcomes could not be pooled for meta-analysis because of insufficient data provided. For example, Amin et al. (17) did not provide the original statistics but only provided p values. Fourth, the assessments of cosmetic appearance, patient satisfaction, and pain were subjective and difficult to integrate. Moreover, the time-point to assess cosmetic appearance earlier than 3 months is not relevant as final maturation of scar; however, only two trials assessed the cosmesis of the wound at 6 months (18, 19) and 12 months (19). Finally, because patients with longer incision sites were seldom recruited, we could not discuss the application of our results to patients with cervical node dissection.
Generally, patients incur additional costs for the tissue adhesive and clip methods. In Taiwan, the use of tissue adhesive (Dermabond) incurs a cost of 1260 TWD (US$39.4) and clips incur a cost of 600 TWD (US$18.75). Moreover, clips may not be the optimal choice from the patient’s perspective, because patients experience secondary pain during clip removal. Furthermore, surgeons provided a more favorable appraisal for subcutaneous sutures than for clips because of the improved cosmetic appearance. In conclusion, none of the methods show unique features that may enhance its application. The choice of closure methods should be made based on technical availability and cost.
Footnotes
Acknowledgements
K.-W.T. helped in conception and design, and development of methodology; Y.-H.H. and C.C. helped in acquisition of data; Y.-H.H., C.C., C.-H.L., E.-W.L., and K.-W.T. helped in the analysis and interpretation of data; Y.-H.H., C.C., C.-H.L., E.-W.L., and K.-W.T assessed in writing, review, and/or revision of the manuscript; Y.-H.H., C.C., C.-H.L., E.-W.L., and K.-W.T. helped in final approval of the version; and Y.-H.H. and C.C. contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from Taipei Medical University and Shuang Ho Hospital (105 TMU-SHH-07). The sponsoring organization was not involved in the study design, data analysis, or data interpretation.