
Abstract
Background:
The objective of this study was to compare the effectiveness and cosmetic results of tissue adhesive or surgical staples in thyroidectomy through a supraclavicular incision.
Methods:
This was a prospective, randomized study of consecutive patients undergoing thyroidectomy by a supraclavicular approach. Eligible patients were randomized into two groups: one group had the incision closed with tissue adhesive (the experimental group) and the other with surgical staples (the control group). The main outcomes included operative time, early postoperative pain measured by Visual Analog Scale, incidence of wound dehiscence and infection, perceived cosmetic outcome, and overall patient satisfaction by using Patient Satisfaction Assessment Form.
Results:
There were 151 consecutive patients assessed for eligibility, and 132 patients were enrolled over 22 months. The clinical characteristics of the patients in the two groups were similar. Main outcomes were assessed in the first 24 h postoperatively, the first month, and the third month postoperatively. Operation time was longer in the experimental group (P = 0.027). Mean Visual Analog Scale scores for pain were lower in the experimental group in the early postoperative period (P < 0.001). No patients developed surgical site infections or wound dehiscence. Lower scores for scar assessment and higher overall satisfaction levels at the first month after surgery were found in the experimental group compared to the control group (P < 0.001). There was no significant difference between the two groups at the third month postoperatively in perceived cosmetic result (P = 0.052) or overall satisfaction (P = 0.059).
Conclusions:
Tissue adhesive is effective and reliable in skin closure for thyroid surgery. While this closure may take somewhat longer to perform, it leads to less postoperative pain, more acceptable wound cosmesis, and higher patient satisfaction levels in short postoperative follow-up.
Introduction
Thyroid disease and thyroid surgery have increased in incidence over time. Cosmetic scars are important in patient satisfaction. There have been numerous techniques developed to enhance the cosmetic results of neck incisions.
In the last decade, minimally invasive thyroid surgery (MITS) techniques have been developed (1–4). However, these techniques are indicated in strictly selected patients. Thyroidectomy through a supraclavicular approach has been developed to obtain a better cosmetic result; its indications have been extended in recent times. The technique has been regarded as a viable addition to the growing number of minimally invasive techniques (5).
There are many different methods of wound closure, which were designed to achieve better cosmesis. All methods have aimed to have no adverse reactions, provide simple postoperative management, simple suture removal, shorter hospital length of stay, and optimal cosmetic appearance of the scar. A major constituent of the tissue adhesive we applied is the liquid monomer of butyl cyanoacrylate. It is inexpensive, simple, painless, and bactericidal, and the most important advantage is its result in optimal cosmetic appearance of the scar, without many of the risks and disadvantages of alternatives (6). A wide variety of studies have compared the cosmetic outcome obtained with tissue adhesive and standard sutured methods in other surgeries (7–10). There have been no large randomized controlled trials confirming the advantage of tissue adhesive in thyroid surgery, especially its role in thyroidectomy through a supraclavicular approach.
The objective of this study was to assess outcomes of thyroidectomy through a supraclavicular approach using tissue adhesive and to determine whether it provided better clinical results than staples.
Patients and Methods
From January 2008 to October 2009, 151 patients were assessed for eligibility. All of these patients had unilateral thyroid nodules with maximum dimension less than or equal to 5 cm and underwent fine needle aspiration biopsy (FNAB) in our department. Results showed that these were atypical thyroid nodules or follicular lesions requiring thyroid surgery for further histological diagnosis. The exclusion criteria were as follows: thyroid carcinoma examined through FNAB; active thyroiditis; a history of previous neck surgery; patients with known blood-clotting disorders; allergy to tissue adhesive, cyanoacrylates, or moleskin; a recent history of fever or infection; hyperthyroidism or hypothyroidism; diabetes mellitus; hypertension; and personal or family history of keloid or hypertrophic scar formation. Those patients in American Society of Anesthesiologists class IV or class V were also excluded (11). In addition to these exclusion criteria, patients whose intraoperative frozen pathological examination showed malignancy and who were in need of expanding the scope of operation and increasing the length of incision were excluded from the study. Patients who agreed to the study criteria were randomly divided into two groups (the experimental group and the control group) (Table 1).
Profile of randomized trial.
Randomization was performed prior to the study, using randomization tables. Patients enrolled in the study were blind to their treatment group prior to the operation.
Most of the surgeries in the study applying the use of tissue adhesives were performed by one senior surgeon only (J-M Qu, n = 120).
Approval was sought from the institutional Ethics Committee for Human Research before initiating the study, and informed consent was given by the patients.
Operative Technique
Patients in two groups underwent thyroidectomy through a supraclavicular lateral collar incision (approximately 5 cm). We have been using this approach since 1999. In the last decade, we have performed this approach on more than 500 patients and found that patients who undergo this surgery have better cosmetic results compared with the conventional surgery (12). All patients underwent preoperative laryngoscopy to assess vocal fold movement. Patients were randomized preoperatively to the incisional closure technique. The thyroidectomy was performed with the patient in a supine position with a roll beneath the shoulders to extend the neck. After routine preoperative preparation, a cervical plexus block with ropivacaine 0.0375% 20 mL was performed. The incision was placed on the ipsilateral enlarged thyroid lobe side. During the operation, we found and protected the recurrent laryngeal nerve in the tracheoesophageal groove. All patients underwent the operations successfully without transecting the cervical anterior muscles, and meticulous attention was paid to wound hemostasis.
At the end of the surgical procedure, saline was used to irrigate the remained cavity and hemostasis was assured under Valsalva maneuver. We did not use drains in any of the patients in the study. The subcutaneous tissue was sutured with Coated VICRYL™ Plus Antibacterial suture (size 4/0), which could aid in apposition of the wound edge margins, relieve tension, ensure adequate skin edge eversion, and prevent deposition of tissue adhesive into the wound; subsequently, we dried the incision and painted it with povidone–iodine; finally, in the experimental group, the incision edges were aligned and then tissue adhesive was applied directly to the incision and repeated two or three times after 10-s intervals. We covered the incision with steristrips. For the patients in the control group, stainless steel skin staples were used. They were removed 5 days postoperatively.
Patients rated their postoperative pain using a Visual Analog Scale (VAS): 0 represented no pain and 10 the worst level of pain (13). The use of VAS and the wound examination were performed by a surgeon who was not informed about each patient’s treatment group and not been involved in the patient’s operation.
Primary Outcome
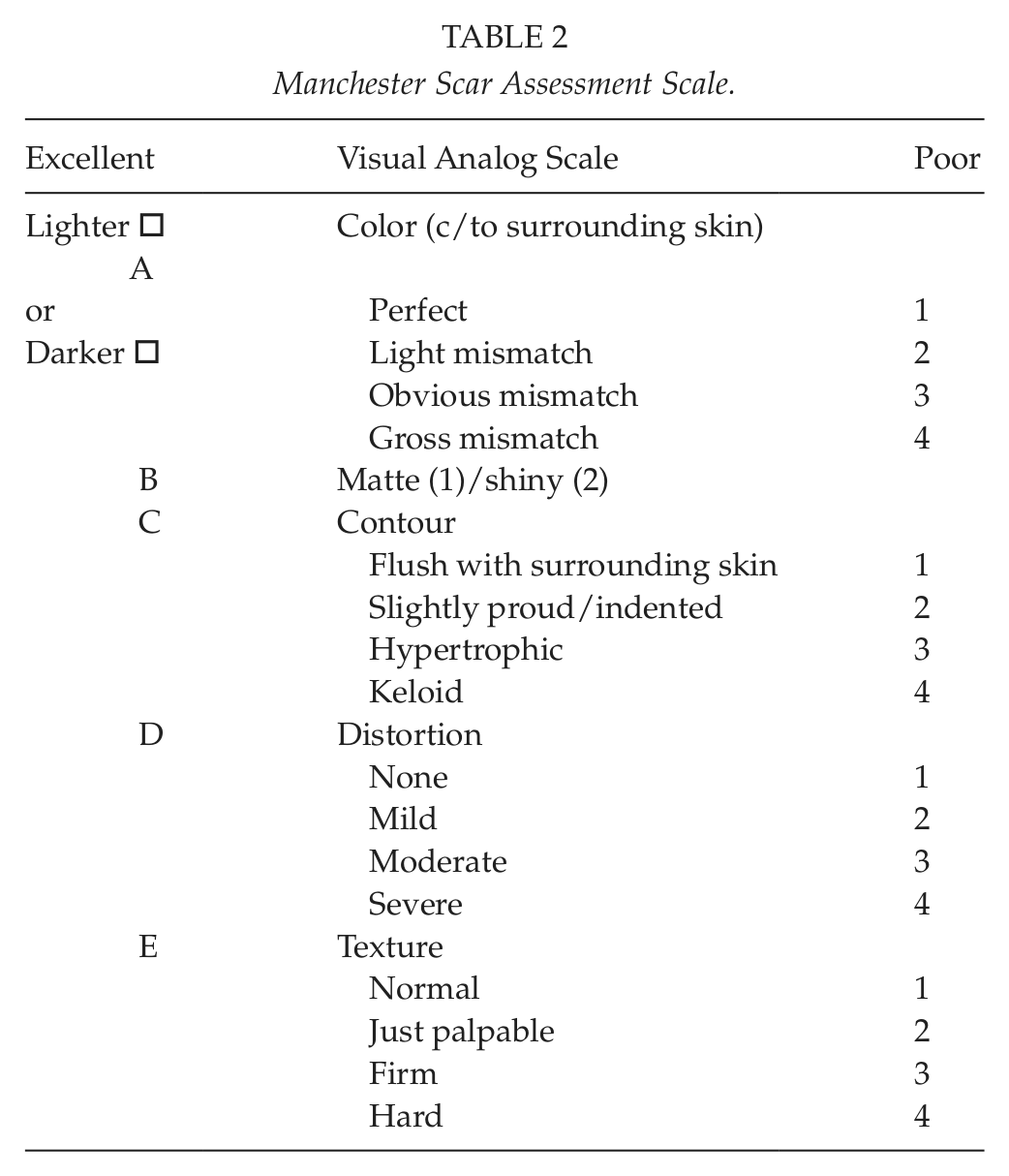
The primary outcomes of the study were operation time, early postoperative pain, incidence of wound dehiscence and infection, cosmetic outcome, and patient satisfaction. Cosmetic outcome and patient satisfaction were assessed at the first and third months after surgery. The Manchester Scar Scale, which is a validated tool and has been used in some other studies to assess scar esthetics, was used in the assessment of cosmetic outcome (Table 2) (14–16). Patient satisfaction was recorded by using the patient Satisfaction Assessment Form, which has also been validated (17). It is based on Cochrane Database recommendations 2002 (18) and devised by Mohamed Amin et al. (Table 3) (14).
Manchester Scar Assessment Scale.
Patient Satisfaction Assessment Form.
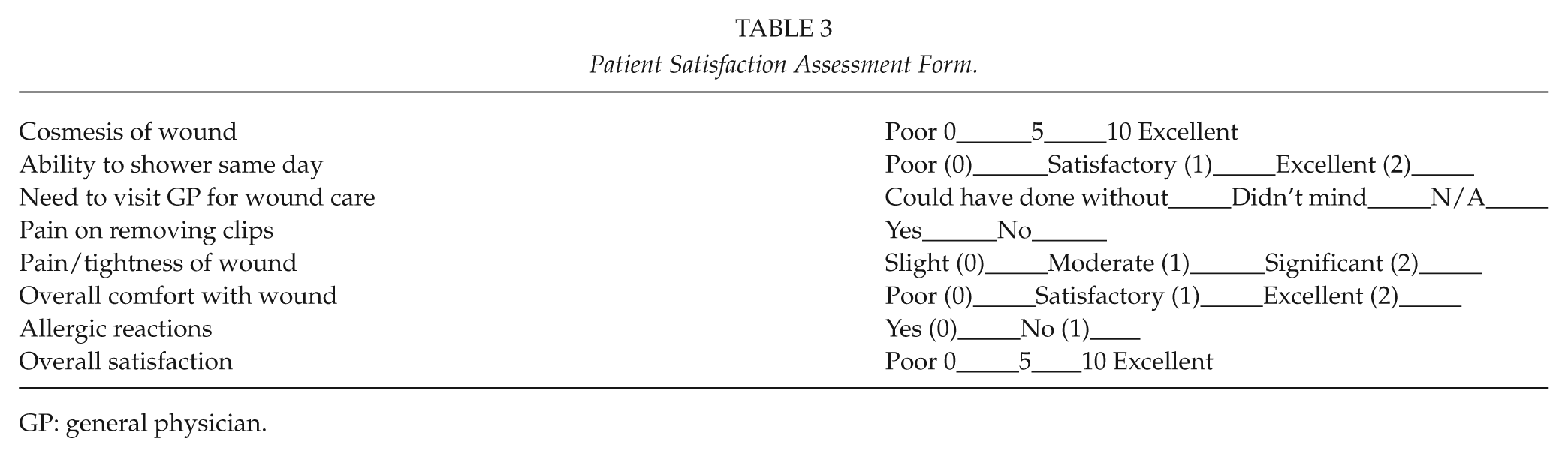
GP: general physician.
Statistical Analyses
This was a blinded, prospective randomized clinical trial. Normally distributed continuous data were assessed using the Student t-test. Categorical data were analyzed using standard χ2 test with or without Yates’ correction. Noncontinuous parametric variables were analyzed using Mann–Whitney U-test. All statistical data were calculated with the SPSS statistical software package 17.0 for Windows (SPSS Inc., Chicago, IL, USA). A P value of less than 0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 151 consecutive patients were asked to participate in the study; 11 patients were excluded (7 patients did not meet inclusion criteria, 3 patients refused to participate, and 1 patient had other reasons). Therefore, 140 patients were enrolled in the study. These patients were randomly divided into two groups (one experimental and one control group) of 70 patients each. In the process of the study, 8 patients were excluded because of intraoperative findings, which led to the need to expand the scope of operation and increase the length of incision. Therefore, there were 65 patients in the experimental group and 67 patients in the control group (Table 1). The clinical characteristics of 132 patients in the two groups were similar (Table 4). All 132 patients completed postoperative follow-up visits at 24 h and at the first and third months.
Patient characteristics.
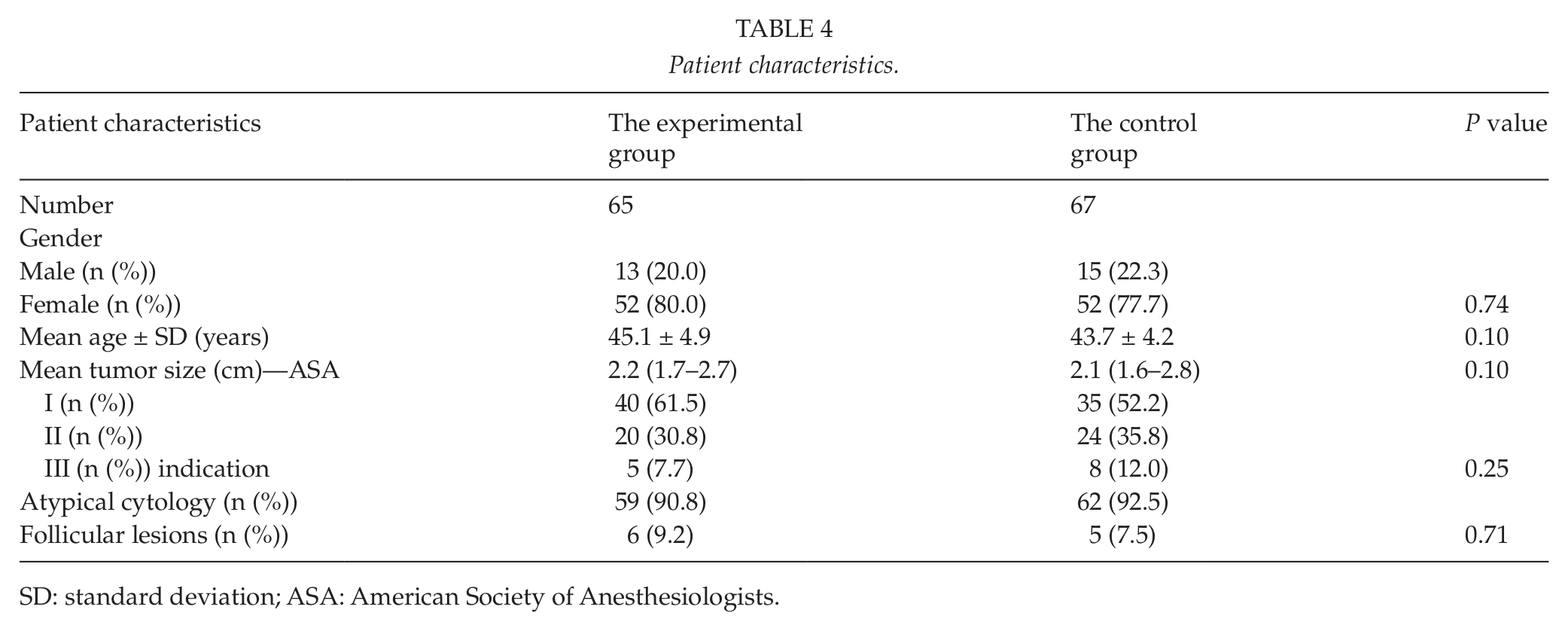
SD: standard deviation; ASA: American Society of Anesthesiologists.
Outcome Measures
Operation time
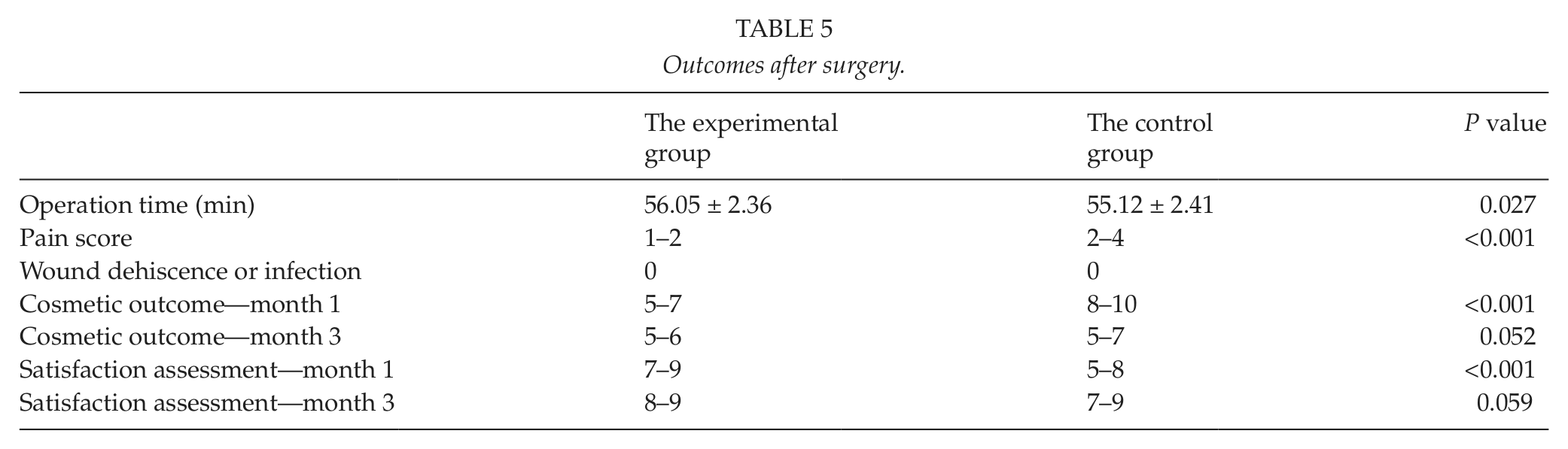
Operation time was longer in the experimental group (56.05 ± 2.36) compared to that of the control group (55.12 ± 2.41) (P = 0.027).
Early postoperative pain
There was significant difference between the two groups in the first 24 h after surgery. The range of VAS scores in the experimental group was 1–2 in the experimental group versus 2–4 in the control group, P < 0.001.
Wound dehiscence and infection
No patients developed surgical site infection or wound dehiscence.
Cosmetic outcome
We assessed the cosmesis of the wound by using the Manchester Scar Assessment Tool (Table 3) at the first and third months after surgery. We used VAS to rate the overall assessment, 0 indicating excellent wound healing and 10 indicating a poor one. At the first month after surgery, the score was significantly lower in the experimental group (range: 5–7) compared to that of the control group (range: 8–10; P < 0.001) (Fig. 1). However, at the third month after surgery, there was no significant difference between the two groups (5–6 vs 5–7; P = 0.052) (Fig. 1).
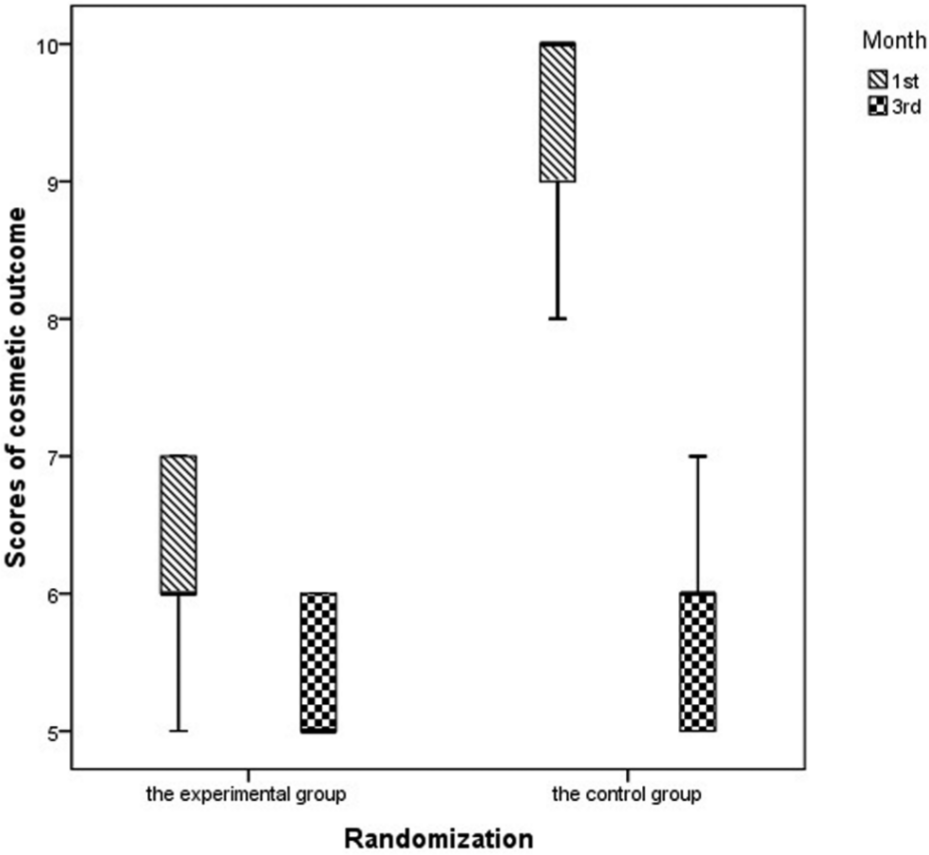
VAS scores used to rate cosmesis at the first and third months of follow-up.
Overall satisfaction
We also used VAS to rate overall satisfaction at first and third months after surgery. The results were different between the two groups at the first month after surgery (P < 0.001). Patients in the experimental group reported less discomfort than those in the control group at the first month after surgery (P < 0.001), but there was no longer a difference in discomfort by the third month (P = 0.059) (Fig. 2). An important contributing factor for patient comfort was the ability to shower immediately and postoperatively in the control group (Fig. 3).
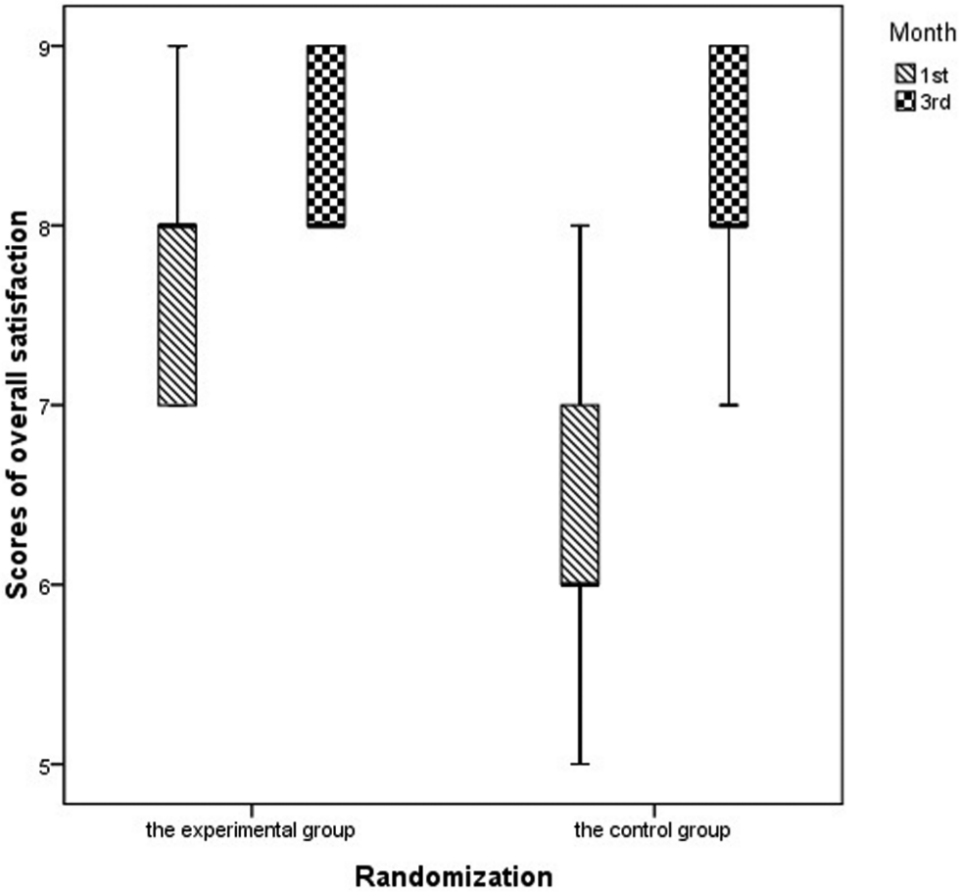
VAS scores of overall satisfaction at the first and third months of follow-up.
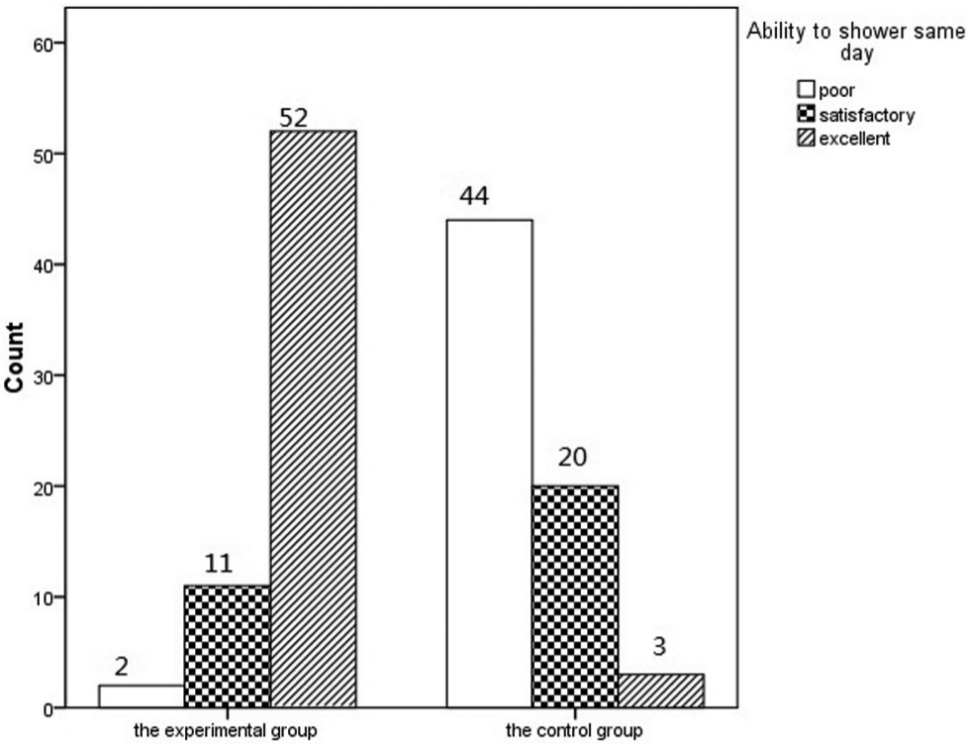
Ability to shower on the first day after surgery in the experimental group and the control group.
The outcome data for operation time, pain scores, incidence of wound dehiscence and infection, cosmesis, and satisfaction assessment are summarized in Table 5.
Outcomes after surgery.
Discussion
Surgical incisions and wounds have always been a source of worry for patients, especially when the incisions are in a visible area of the body, such as the neck (19, 20). Acceptable wound cosmesis has become a focus for thyroid surgeons. Various operative techniques and methods of skin closure have been described (3, 12, 14, 21, 22). Supraclavicular lateral collar incision is a feasible and safe approach for thyroidectomy. It has more extensive indications compared to the minimally invasive techniques, such as the completely endoscopic thyroid surgery and video-assisted small incision thyroid surgery. Our department has amassed a large experience in this approach (12). Some studies have found that there is no significant difference in operation time, blood loss, postoperative complications, length of stay, and hospital costs compared with conventional surgery (5). It has been shown to have a better cosmetic result compared with traditional incision, especially because of the shorter incision length and alternate site. In order to achieve even better cosmesis on the basis of the technique, we prospectively investigated the tissue adhesive versus stapled closure of incision after thyroidectomy for benign disease.
The application of tissue adhesive for skin closure in surgery is an attractive alternative to sutures (7, 23–25). A major constituent of the tissue adhesive we applied is butyl cyanoacrylate monomer, which is liquid. When coming into contact with water and tissue fluid, it synthesizes the polymer and forms a layer of waterproof adhesive material. It can inhibit microbial growth in vitro, such as Escherichia coli and Salmonella (26). The first study comparing tissue adhesive with standard suturing techniques in long surgical incisions demonstrated that there was a trend toward decreased incidence of wound infection in the group closed with tissue adhesive (18). To date, cosmetic outcome comparable with standard suturing techniques have been attained in many other surgeries, such as pediatric (11, 27), breast (7), and brain surgeries (23), and laparoscopic transabdominal preperitoneal hernioplasty (24).
No dressing change or suture removal is needed after tissue adhesive closure. Once the adhesive material falls off, the skin heals. The scar in skin wound is obviously less than that with traditional suture. Chen et al. (28) demonstrated that incisions closed with tissue adhesive have fewer early complications and a better cosmetic appearance. Amin et al. (14) reported higher patient satisfaction levels in MITS with the use of tissue adhesives. To our knowledge, this is the first large prospective randomized study to analyze the effects of tissue adhesive in thyroidectomy through a supraclavicular approach. The short- and long-term clinical results indicated that patients who had their incisions closed with tissue adhesive had a better cosmetic appearance and a higher degree of satisfaction than those closed with staples at the 1-month postoperative follow-up. However, patients were allowed to shower after closure with staples. These patients also appreciated the complete absence of gauze, ability to shower immediately after surgery, and no stitches being removed, all of which reduced the degree of anxiety. These benefits were no longer seen at the 3-month postoperative follow-up.
Some studies have indicated that staples would increase the incidence of wound complication, such as infection, compared with subcuticular suturing (29). Our study did not find any difference in wound complications.
Conclusion
The authors advocate that tissue adhesive for the closure of supraclavicular incision of thyroidectomy should be favored over skin staples. Tissue adhesive has many advantages, such as it is not needed to return to the hospital for suture removal, the ability to shower immediately after surgery, having a good cosmetic outcome, and high patient satisfaction levels in the short term.