
Abstract
Background:
Total mesorectal excision has evolved from open to minimally invasive techniques. To overcome difficulties in the lowest part of the pelvis, transanal total mesorectal excision was introduced and has gained acceptance in the recent years. The results of transanal total mesorectal excision seem to be comparable to laparoscopic total mesorectal excision. Whether or not transanal total mesorectal excision has changed the pattern of defects in the retrieved mesorectal specimens is yet to be clarified.
Purpose:
To determine the pattern of mesorectal defects following transanal total mesorectal excision, compared to laparoscopic total mesorectal excision. The primary end-point was the location of defects in the part of the mesorectum below the peritoneal reflection, as it is this part, which is dissected from below in the transanal total mesorectal excision procedure.
Methods:
From our transanal total mesorectal excision database that includes all transanal total mesorectal excision procedures performed at our institution since 2013, we have included 29 patients who originally had defects in their retrieved specimens. Another 29 patients who underwent laparoscopic total mesorectal excision with mesorectal defects served as a control group. All specimen photos and pathology reports were reviewed systematically; sites and pattern of defects were defined.
Results:
A higher ratio of the defects in the laparoscopic total mesorectal excision group was located below the peritoneal reflection (P = 0.043). The distribution of defects by anatomical quadrant was not statistically different between the groups.
Conclusions:
The ratio of defects below the peritoneal reflection was lower in the transanal total mesorectal excision group. Whether this is due to a lower incidence of defect in transanal total mesorectal excision is not part of our study.
Keywords
Introduction
The aim in rectal cancer surgery is the achievement of clear resection margins through dissection in the correct planes (1). Adherence to the correct planes is an important prognostic factor for local recurrence (2, 3). As a “gold standard” technique, total mesorectal excision (TME) can improve rectal cancer care (4–6). The quality of surgery via laparoscopic approach seems to be comparable with that of open approach, of which the initial improvements were attributed to (7–9). The importance of a clear circumferential resection margin (CRM) in rectal cancer surgery is well documented (10). However, the macroscopic quality of the retrieved specimens has indeed an important prognostic role (11). Systematic gross evaluation of the mesorectal specimen adds important information to the microscopic examination (12).
Although excellent surgical resection plane results have been achieved in the recent years by open and laparoscopic surgeries for rectal cancer (13, 14), transanal total mesorectal excision (TaTME) could potentially improve several outcomes, including the specimen quality. The published literature has shown promising results (15–17). However, TaTME is merely a modification of laparoscopic total mesorectal excision (LaTME), where part of rectal dissection is done from below. Thus, it is not well understood how much TaTME has contributed to the improvement in the quality of the resected specimen (if any) or influenced the site and pattern of defects in the mesorectal specimen compared to LaTME. We hypothesized that TaTME could have changed the pattern of mesorectal defects, especially under the peritoneal reflection, which is where quality improvement is hoped for. Thus, we aimed in this study to determine the sites and pattern of mesorectal defects in TaTME and LaTME.
Methods
Rectal cancer surgery is well standardized and organized in Denmark and our unit is a large-volume colorectal surgery center. We have adopted a multidisciplinary team approach in the last 10 years. Since 2013, TaTME was implemented and a prospectively maintained database created. In addition, all colorectal cancer patients are registered in a national database since 2001 (4, 18). From our TaTME database, we have chosen 29 patients who had suboptimal TME specimen quality (intramesorectal plane and muscularis propria plane) (2). At the time of inclusion, some 130 patients have undergone TaTME at our institution. A control group of 29 patients who underwent LaTME, in whom the specimen quality was suboptimal in the immediate period prior to the implementation of TaTME. The study includes patients operated from October 2010 to March 2017. No approval of the scientific ethical committee was required, as the study did not include patient intervention. “The Danish Data Protection Agency” has approved the database.
Preoperative Diagnostic Workup and Surgical Technique
Our standard preoperative assessment and details of the surgical technique in both TaTME and LaTME are described in our previous publication (16).
Pathological Assessment
The standard histopathological assessment at our institution includes a combined evaluation of the freshly excised, and later of the formalin-fixed specimens. All specimens are photographed and the macroscopic evaluation is included in the assessment of the surgery plane in concordance with National Danish Guidelines as original suggested by Quirke et al. (2) Specimens are classified according to our standard evidence based protocol into the following grades of quality.
Complete (mesorectal plane)
Intact mesorectum with only minor irregularities of a smooth mesorectal surface; no defects deeper than 5 mm: no coning; and smooth CRM on slicing.
Nearly complete (intramesorectal plane)
Moderate bulk to mesorectum, with irregularities of the mesorectal surface; moderate distal coning; muscularis propria not visible with the exception of the levator insertion; and moderate irregularities of CRM.
Incomplete (muscularis propria plane)
Little bulk to mesorectum with defects down onto muscularis propria, very irregular CRM, or both.
Lesions involving the peritoneal surface and expose mesorectal fat were scored, likewise the surgical resection margin. Thus, we included in the present study those specimens from our database that were classified as nearly complete or incomplete. Both macroscopic and microscopic assessments form the basis for a comprehensive histopathological report as a standard part of the multidisciplinary rectal cancer care. The report additionally includes information about the CRM and distal resection margin (DRM) status, whether or not mucinous component, lymphovascular or perineural invasion were present. The CRM and DRM were considered involved if the distance from the resection margin to the tumor was <1 mm. The status of lymph node yield and involvement is documented. We have chosen the following method to re-evaluate the mesorectal specimens with focus on the end-points of this study: two specialized colorectal pathologists have separately reviewed specimen photos for each patient. First, each pathologist evaluated the specimen photos independently of one another without using the information documented in the original comprehensive pathology report. The original report was used as a third independent evaluation. Disagreements were solved through consensus between the two pathologists. For specimens retrieved through TaTME, the distal 1 cm was not included in the evaluation as it is composed of the purse string suture. The primary end-point was the study of the defects in the lower part of the rectum, which is dissected from below in the TaTME procedure and thus differentiates the two procedures. To ease the pathological assessment, we have used the peritoneal reflection as the separating line between what is “above” and what is “below.” The peritoneal reflection was considered the level of the horizontal/circumferential line that differentiated the two parts of dissection in TaTME.
Statistical Analysis
Data are expressed as mean with standard deviation. Comparisons were done by independent samples t test for numerical variables and Pearson chi-square test or Fisher’s exact test for categorical variables when appropriate. A P value < 0.05 was considered statistically significant. All analyses were performed with the software package SPSS, version 24.0 (SPSS 24.0; SPSS Inc., Chicago, Illinois, USA).
Results
The baseline patient and tumor characteristics are summarized in Table 1. Except for American Society of Anesthesiologists (ASA), both groups were statistically comparable. Operative data showed a statistically significant difference in operative time, blood loss, and DRM involvement in favor of TaTME group, as summarized in Table 2.
Baseline patient and tumor characteristics.
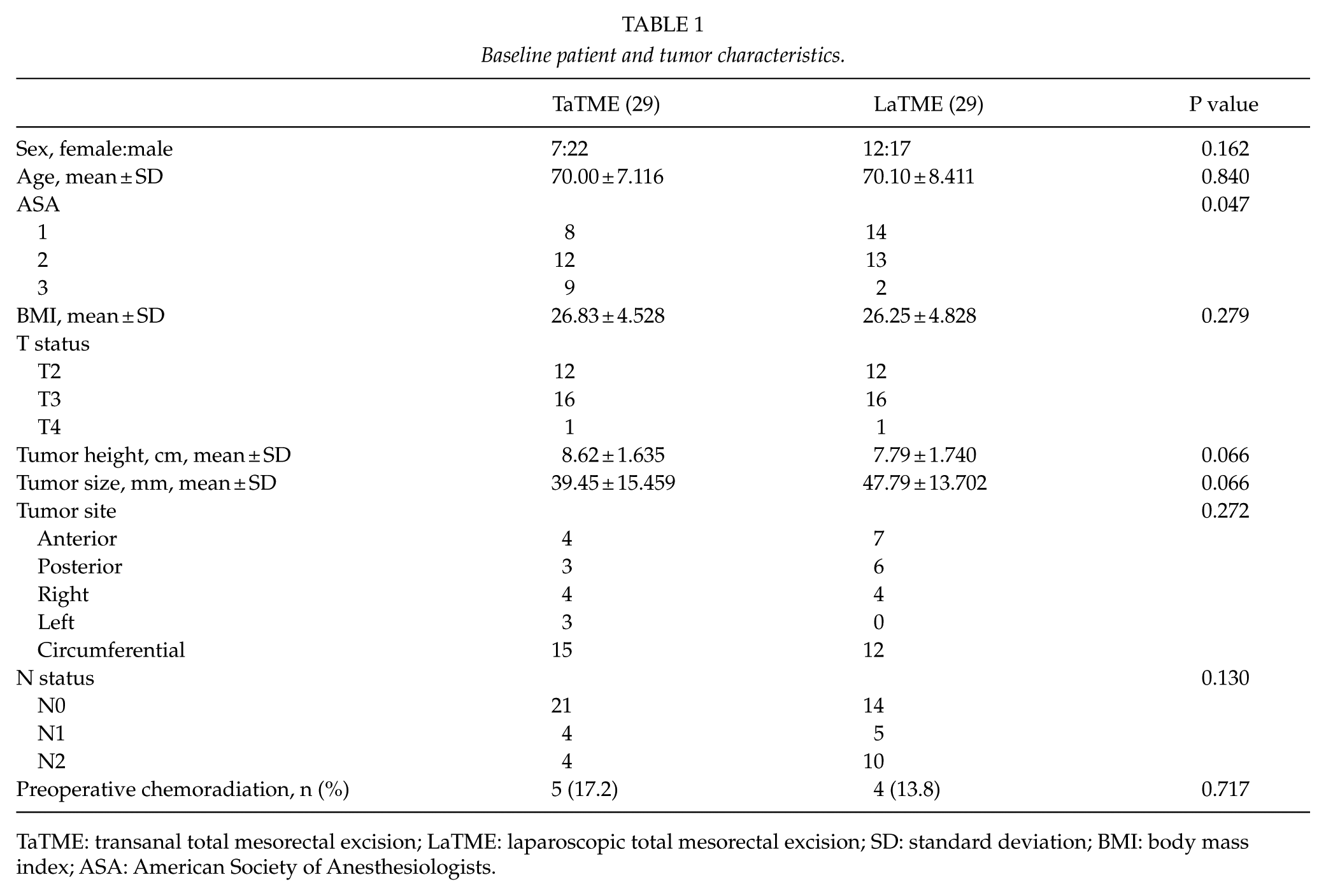
TaTME: transanal total mesorectal excision; LaTME: laparoscopic total mesorectal excision; SD: standard deviation; BMI: body mass index; ASA: American Society of Anesthesiologists.
Intraoperative and postoperative results.
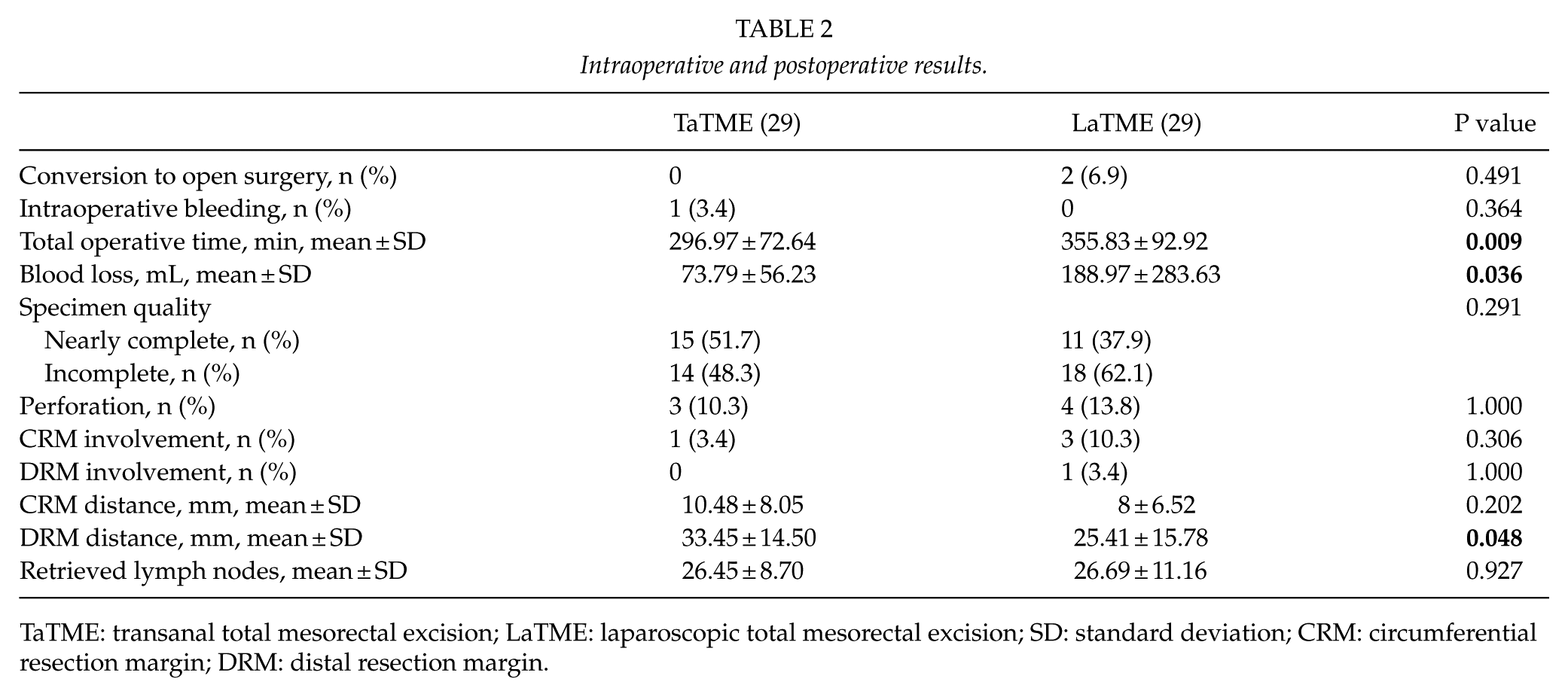
TaTME: transanal total mesorectal excision; LaTME: laparoscopic total mesorectal excision; SD: standard deviation; CRM: circumferential resection margin; DRM: distal resection margin.
Table 3 summarizes the main findings related to the mesorectal defects. The distribution of the mesorectal defects in relation to the peritoneal reflection for the whole cohort was as follows: above 17 (29.3%), below 22 (37.9%), and defects both above and below 19 (32.8). When the distribution of the defects was compared according to potential locations (above, below, or both), the difference did not reach statistical significance (P = 0.054). However, the difference reached statistical significance when categorizing the groups according to whether or not a specimen had a defect below the peritoneal reflection (P = 0.043). Thus, the ratio of the defects below the peritoneal reflection was higher in the LaTME group.
Comparison of mesorectal defect sites.
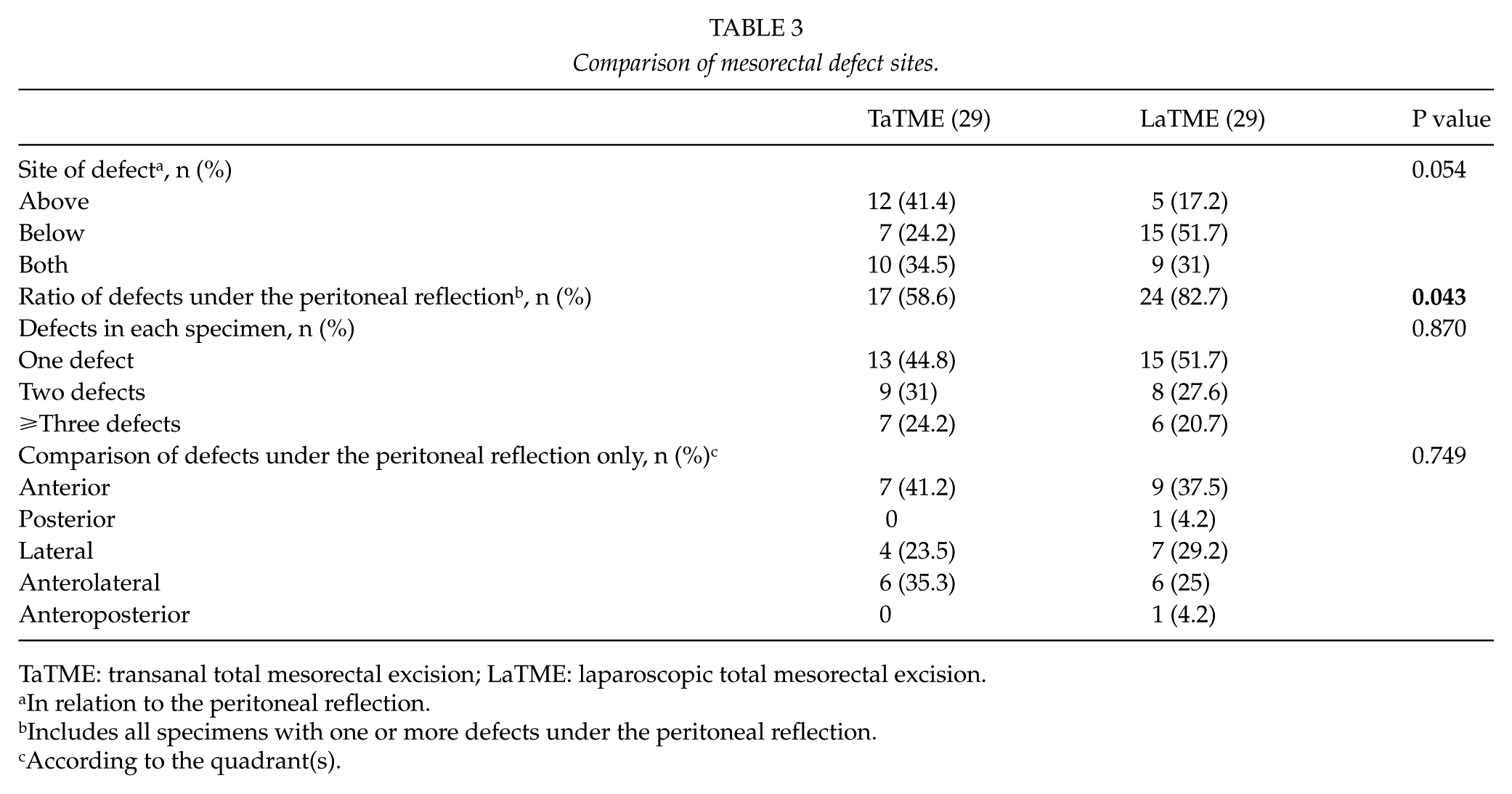
TaTME: transanal total mesorectal excision; LaTME: laparoscopic total mesorectal excision.
In relation to the peritoneal reflection.
Includes all specimens with one or more defects under the peritoneal reflection.
According to the quadrant(s).
Discussion
This study was designed to test the theory of the impact of TaTME on sites and pattern of defects in patients with “incomplete” or “nearly complete” mesorectal specimens. We have found that defects in TaTME more often than in LaTME are located above the peritoneal reflection, the finding is statistically significant, and a higher ratio of below-reflection defects were found in the LaTME group. Defects—regardless of the technique—are more predominant in the anterior and lateral quadrants. This emphasizes once again the difficulties encountered on both sides of the mesorectum while striving to stay in the embryological plane. In addition, scarcity of tissue anteriorly might have a role in that Denonvilier’s fascia is not always removed during rectal resection to avoid nerve injury.
To our knowledge, this is the first study that focuses solely on the subject of the defect distribution and pattern in rectal cancer surgery. The plane of surgery is a significant factor in determining long-term prognosis (2). However, it is not clear whether minor defects in the mesorectum affect the oncological outcomes. In a recent meta-analysis of four randomized controlled trials comparing laparoscopic and open approaches for rectal cancer (19), the superficial defects (nearly complete specimens) were more common in the laparoscopic group. Thus, minimal invasive surgery could result in a larger number of defects due to handling the tissue with relatively sharp instruments.
Laparoscopic surgery for rectal cancer has been questioned in two recent randomized controlled trials (13, 14). In both studies, laparoscopic surgery failed to be “noninferior” to open surgery. The so-called composite outcome was used in both studies and included a combination of involved resection margins and specimen quality. The issue of conversion to open surgery is also well known. In a randomized trial comparing the laparoscopic and open surgeries, a conversion rate of 17% was found (8), mainly in patients with lower tumors. Conversion can be attributed to limitations of laparoscopic instruments, which in turn might produce more defects as the dissection progresses downward in the pelvis.
It was mainly due to the limitations of laparoscopy that TaTME was introduced. At this time, the bulk of published case series and comparative studies of TaTME and LaTME suggest obvious short-term benefits (15, 17, 20–22). The main source of optimism lies in the abolished need for conversion in TaTME, as compared to LaTME. The transanal dissection option allows for a more precise tissue removal and—theoretically—lower number of mesorectal defects below the peritoneal reflection. The dissection from below is not easy, though is easier than dissection of the lower rectum from above, as in LaTME (23). As a very promising method, TaTME has gained huge interest and several technological modifications since the first human case publication in 2010 (24). Method-driven developments included (a) changing the CO2 insufflator to one that could deliver a stable flow and provides a stable operative field (25), (b) technical tips of how to fashion anastomosis (26), (c) operative tips (27, 28), and (d) methods of navigation in the pelvis (29, 30). The aim of the ongoing efforts to optimize dissection is an improvement in the oncological quality, which is measured by the quality of the removed mesorectum. The published series to date have suggested that TaTME results in high number of “complete” and “nearly complete” mesorectal specimens. The question is whether TaTME has changed the pattern of tissue removal at the lower part of the rectum. To answer this question, we need to study the mesorectal quality and the number and location of the defects in the lowermost part. In our hands, transanal dissection involved the part of the mesorectum that is below the peritoneal reflection. Thus, defects in this area are of special interest when studying the impact of TaTME.
There are several limitations of our study. First, it is retrospective in that the control group was found through search in the historical data to find patients with suboptimal mesorectal quality. Second, although the assessment of all patients undergoing rectal cancer surgery is standardized, the initial assessment of neither group has focused on the main end-point of this study. In a prospectively designed study of the mesorectal quality, information that is more detailed can be collected and the dissection “field” belonging to the abdominal or transanal part can be marked already intraoperatively. Furthermore, it is our experience that the evaluation of the resection plane is subjective, and the evaluation of specimen photos will always be inferior compared with evaluation of the specimen itself. We tried though to overcome these limitations through a systematic review of the mesorectal specimens by two independent colorectal pathologists. Third, the sample size is small and it is obviously due to the limited number of cases who have suboptimal specimen quality reflecting the case volume of TaTME achieved to date.
Future studies have to focus on the precise number and location of defects, preferably in a protocolled systematic way combining the information gained preoperatively through imaging, operative details, and pathologic assessment.
Conclusion
This study suggests that the pattern of defects in the retrieved mesorectal specimens differs according to the operative technique (TaTME vs LaTME). When the sites of defects are analyzed according to the anatomical location (above or below the peritoneal reflection), the ratio of defects below the peritoneal reflection is lower in the TaTME group compared to the LaTME group. Thus, TaTME has the potential to improve rectal cancer surgery through improvement in the quality of dissection in the lower rectum.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.