
Abstract
Background and Aims:
Appendectomy is a common surgical procedure, but no overview of the long-term consequences exists. Our aim was to systematically review the long-term complications of appendectomy for acute appendicitis.
Materials and Methods:
This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A protocol was registered on PROSPERO (CRD42017064662). The databases PubMed and EMBASE were searched for original reports on appendectomy with n ≥ 500 and follow-up >30 days. The surgical outcomes were ileus and incisional hernia; other outcomes were inflammatory bowel disease, cancer, fertility, and mortality.
Results:
We included 37 studies. The pooled estimate of the ileus prevalence was 1.0% over a follow-up period of 4.6 (range, 0.5–15) years. Regarding incisional hernia, we found a pooled estimate of 0.7% prevalence within a follow-up period of 6.5 (range, 1.9–10) years. Ulcerative colitis had a pooled estimate of 0.15% prevalence in the appendectomy group and 0.19% in controls. The opposite pattern was found regarding Crohn’s disease with a pooled estimate of 0.20% prevalence in the appendectomy group and 0.12% in controls. No clear pattern was found regarding most of the examined cancers in appendectomy groups compared with background populations. Pregnancy rates increased after appendicitis compared with controls in most studies. Mortality was low after appendectomy.
Conclusion:
Appendectomy had a low prevalence of long-term surgical complications. We did not find any significant other long-term complications, though the prevalence of Crohn’s disease was higher and the prevalence of ulcerative colitis was lower after appendectomy than in controls. Appendectomy did not impair fertility.
Keywords
Introduction
Appendicitis is a common disease seen in the emergency department (1). It is normally treated with appendectomy by either a laparoscopic or an open approach. Therefore, appendectomy is a frequent surgical procedure (2). Every operation has potential complications on both short and long term. The main short-term complications of appendectomy such as infections and intra-abdominal abscesses have already been investigated (3). However, it is important to assess the risk of long-term complications for abdominal procedures such as ileus and incisional hernia (4, 5). Finally, also death may be the undesired result of surgery. Appendix is part of the digestive tract, but the exact function of the appendix is yet to be clarified. The appendix might have an immunological role in the intestine (6). Thus, it has been examined whether removal of the appendix could have a role in the development of inflammatory bowel disease or cancer (7–10). Furthermore, the inflammation and possible scarring caused by a ruptured appendix has been suspected as a reason for infertility (11).
No overview of the existing literature regarding the long-term complications of appendectomy for acute appendicitis has been conducted. Therefore, this study aimed to systematically review the long-term surgical complications and other long-term consequences of appendectomy for acute appendicitis.
Material and Methods
Protocol and Eligibility Criteria
Prior to data extraction, a protocol was registered on PROSPERO (registration number: CRD42017064662) (12). This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (13).
There was no limitation set on date of publication. Published studies written in English, German, Danish, Swedish, or Norwegian were included. Studies regarding populations with patients of all ages were included. The intervention was appendectomy for suspected acute appendicitis. The unexposed populations were defined as people, who had not had an appendectomy.
Our outcomes were divided into the long-term surgical complications (ileus and incisional hernia) and the other outcomes (inflammatory bowel disease, cancers, fertility, and mortality). Original reports on prospective cohort studies, retrospective cohort studies, and register-based studies with a study population of at least 500 patients were included. The length of follow-up in the studies had to be more than 30 days.
Literature Search
The search was done in the databases PubMed (1966 to present) and EMBASE (1980 to present) and was conducted on the 24 February 2017 after consulting a medical research librarian.
Search string used in PubMed:((((((“appendectomy”[MeSH Terms] OR “appendectomy”[All Fields]) OR (“appendectomy”[MeSH Terms] OR “appendectomy”[All Fields] OR “appendectomies”[All Fields])) OR (“appendectomy”[MeSH Terms] OR “appendectomy”[All Fields] OR “appendicectomy”[All Fields])) OR (“appendectomy”[MeSH Terms] OR “appendectomy”[All Fields] OR “appendicectomies”[All Fields])) OR (“appendicitis”[MeSH Terms] OR “appendicitis”[All Fields])) AND (((((((cohort[All Fields] OR “register”[All Fields]) OR “follow-up”[All Fields]) OR followup[All Fields]) OR “long-term”[All Fields]) OR longterm[All Fields]) OR “case control”[All Fields]) OR “case controlled”[All Fields])).
The search string used in PubMed was adapted to EMBASE and is available in the protocol registered on PROSPERO (12).
Study Selection and Data Extraction
Two reviewers (S.F. and T.R.) independently screened the studies according to the eligibility criteria using Covidence (www.covidence.org). The study-selection process was done in three rounds (screening, assessing for eligibility, and snowballing) and is depicted in Fig. 1.
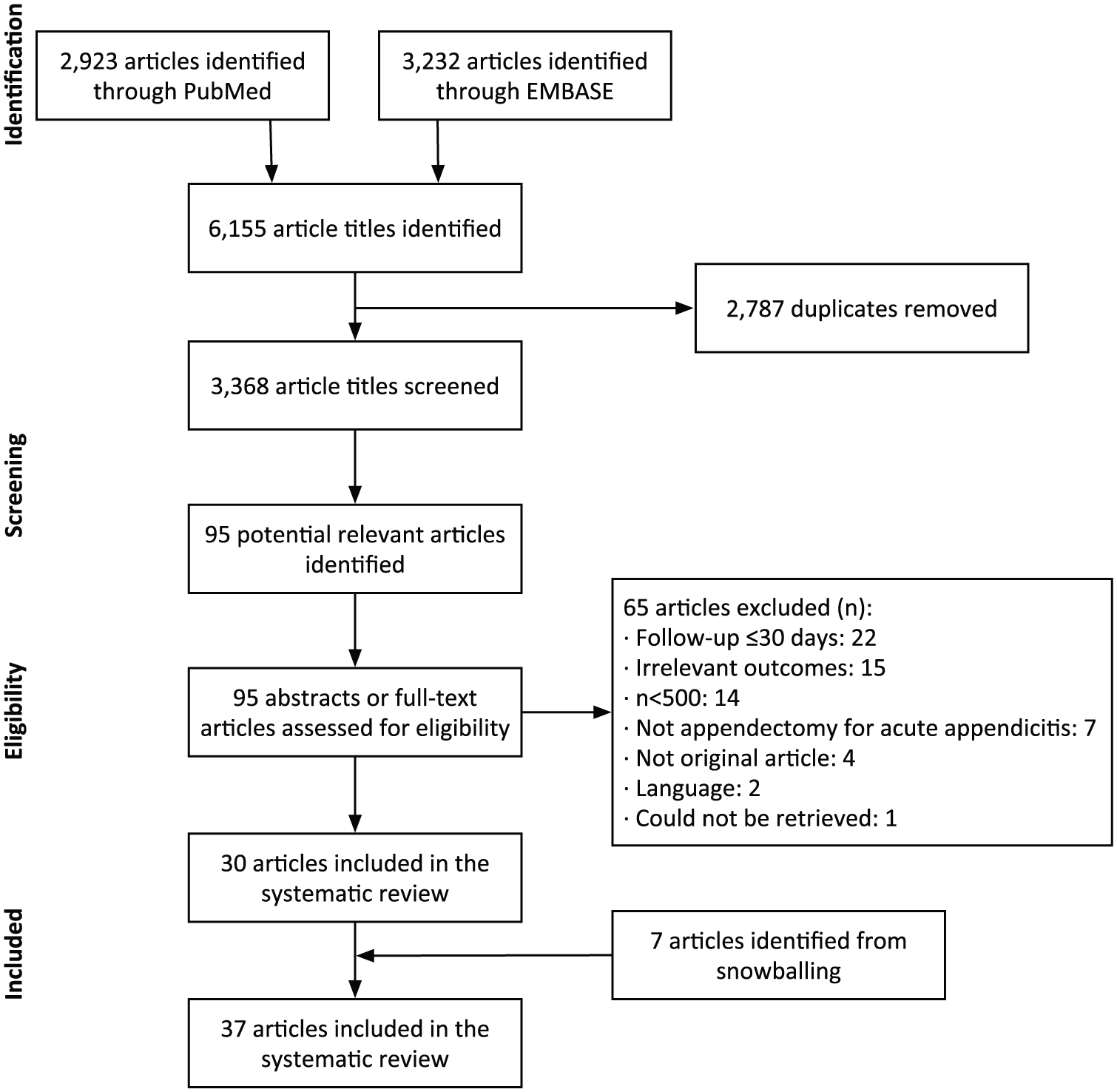
Flowchart of the study-selection process.
One reviewer (T.R.) extracted the data items from every study into an Excel sheet (Excel 2010, Microsoft Office). In cases of doubt regarding the data extraction, the rest of the author group was consulted and consensus reached.
The data items that were extracted from all studies were: authors, publication year, study design, number of patients (and when relevant: number of controls), follow-up time, surgery type (open/laparoscopic/converted), and appendicitis definition (according to diagnostic codes (including which), procedure codes (including which), or medical records). Furthermore, study outcomes were extracted: definition of outcome, and both rate and frequency of outcome including ileus, incisional hernia, inflammatory bowel disease, cancers, fertility, and/or mortality.
It was assumed that appendectomy without any other procedure or surgical code was appendectomy for acute appendicitis. Furthermore, some simplifications were made. Ileus was interpreted as all the following terms: small-bowel obstruction, bowel obstruction, large-bowel obstruction, intestinal obstruction, and ileus. Also, some studies categorized laparoscopic appendectomy as intended laparoscopic appendectomy if the commenced laparoscopic procedure was converted to open appendectomy. We used the same categorization in this study. The age of the population was divided into three age groups: all, adults (>18 years, but sometimes including >15 years or excluding >60 years), and children (<18 years, but sometimes excluding >15 years or including <20 years).
Analysis
Risk of bias in the included studies was assessed with the Newcastle-Ottawa Scale (14) as recommended by the Cochrane collaboration (15). This tool was suitable, since all the studies were observational studies. According to this scale, the studies are graded with a score of zero to nine stars. A low number of stars equal a high risk of bias and vice versa.
Data were examined for normality with histograms and QQ-plots in SAS Enterprise Guide 7.1 (SAS Institute Inc, USA). None of the data were normally distributed; therefore, the medians and ranges (in parentheses) were calculated. When relevant, the hazard ratio (HR), the risk ratio (RR), or the standardized incidence ratio (SIR), including the confidence intervals (CIs), was given.
The results in this systematic review are presented as a narrative/qualitative synthesis. Because of the heterogeneity among the studies, no meta-analysis could be made. For didactic reasons, however, we calculated pooled estimates based on the reported prevalence, but without formal statistical comparisons between groups.
When possible, a subgroup analysis was made based on the surgical method for appendectomy: laparoscopic appendectomy (including intended laparoscopic appendectomy) or open appendectomy according to procedure codes (16–18). We also planned to make a subgroup analysis based on the type of the removed appendix, for example, non-perforated, perforated, and normal appendix according to diagnostic codes or medical records (19).
Results
We included 37 articles in this review (20–56). The study-selection process is depicted in Fig. 1. An overview of characteristics of the included studies can be seen in Table 1.
Characteristics of the included studies.
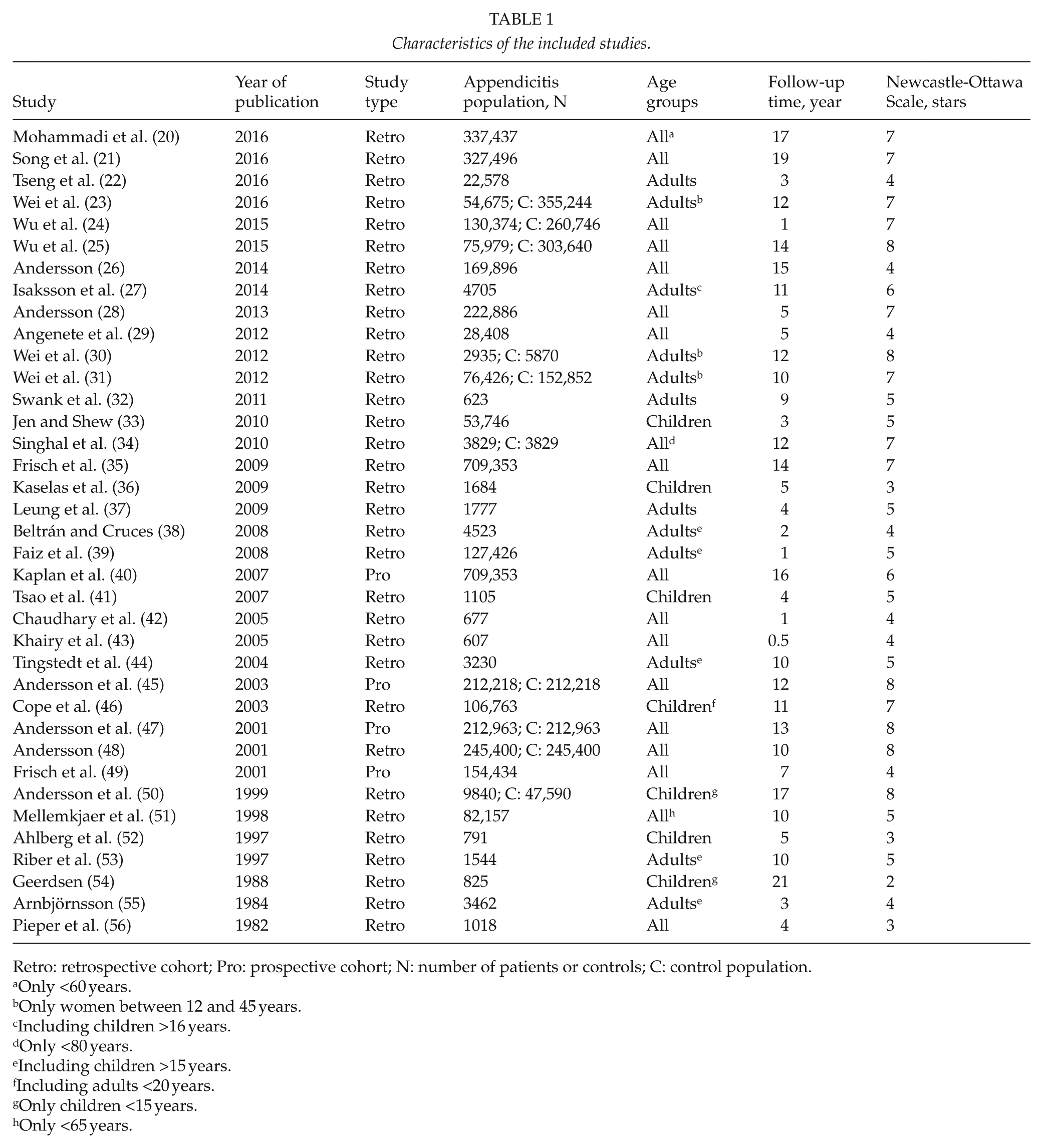
Retro: retrospective cohort; Pro: prospective cohort; N: number of patients or controls; C: control population.
Only <60 years.
Only women between 12 and 45 years.
Including children >16 years.
Only <80 years.
Including children >15 years.
Including adults <20 years.
Only children <15 years.
Only <65 years.
Some of the studies reported more than one outcome. Ileus was the most reported outcome as 16 of the included studies reported on this complication (22, 26, 27, 29, 33, 36, 37, 41–44, 48, 52, 53, 55, 56), whereas only four of the included studies reported on incisional hernia (32, 38, 44, 56). Furthermore, six of the included studies reported on inflammatory bowel disease (34, 35, 40, 45, 47, 49), six on cancer (20, 21, 24, 25, 46, 51), five on fertility (23, 30, 31, 50, 54), and three on mortality (26, 28, 39).
Risk of Bias Within Studies
Of the 37 included studies, there were four prospective cohort studies (40, 45, 47, 49) and 33 retrospective cohort studies (20– 39, 41–44, 46, 48, 50–56). The median risk of bias score was five (range, 2–8) stars in the included studies.
Ileus
A total of 16 retrospective cohort studies reported on ileus (22, 26, 27, 29, 33, 36, 37, 41–44, 48, 52, 53, 55, 56; Table 2). The studies had a median population of 2504 (range, 607–245,400) persons. The median follow-up time was 4.6 (range, 0.5–15) years, and the bias assessment score had a median of four (range, 3–8) stars.
Ileus.
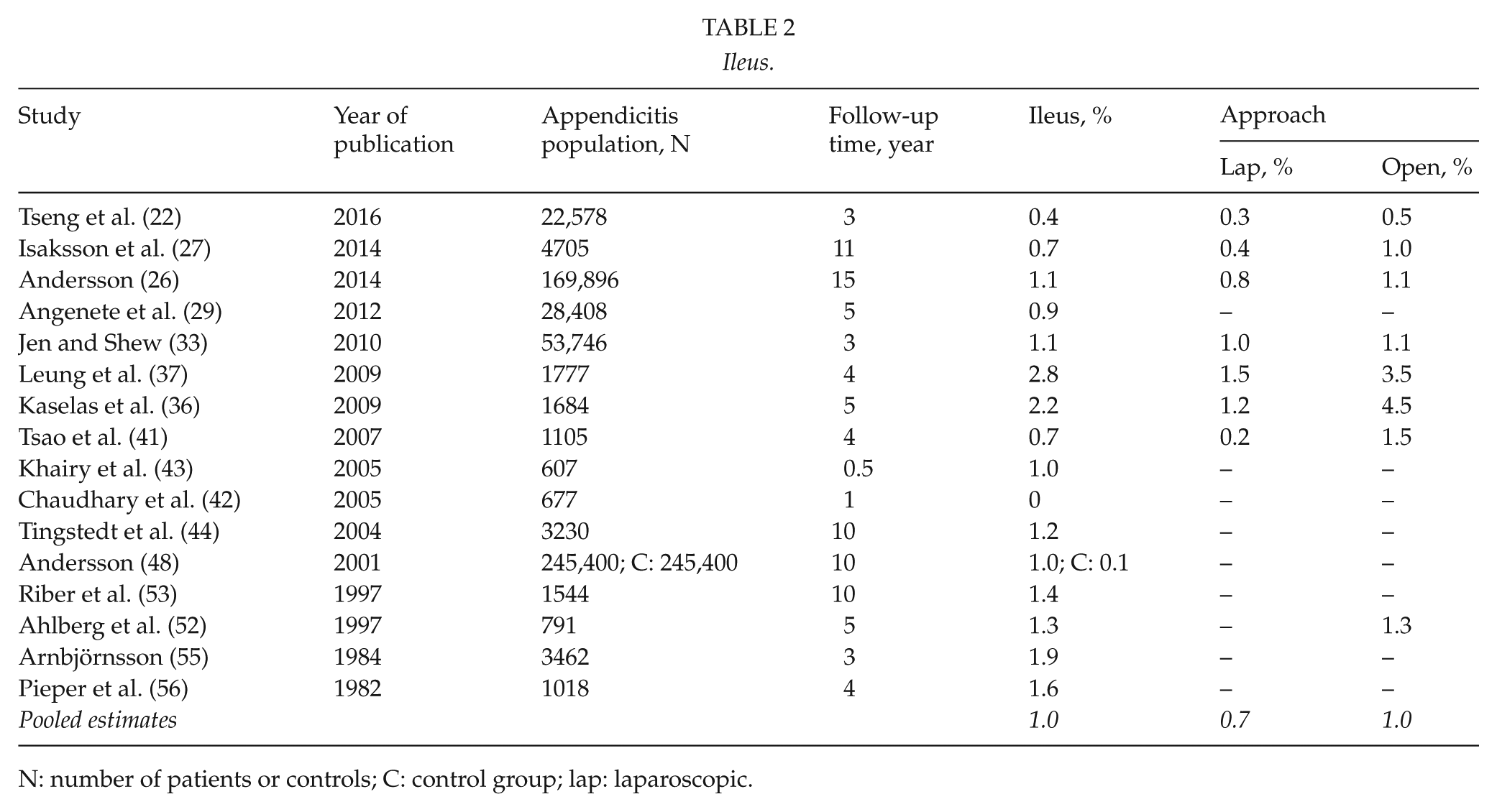
N: number of patients or controls; C: control group; lap: laparoscopic.
Most of the studies examined both surgically and conservatively treated mechanical ileus (26, 27, 29, 36, 37, 41, 44, 55). Three studies only included surgically treated bowel obstruction (48, 52, 53), and five studies did not state the definition of bowel obstruction (22, 33, 42, 43, 46).
Overall, the median prevalence of ileus was 1.1% (range, 0%–2.8%). Seven studies compared a laparoscopic approach with an open approach (22, 26, 27, 33, 36, 37, 41). The median prevalence of ileus was 0.8% (range, 0.2%–1.5%) for the laparoscopic approach and 1.2% (range, 0.5%–4.5%) for the open approach. One study reported only on an open approach and found a prevalence of ileus of 1.3% (52). Pooling the prevalence showed an estimate of overall prevalence of ileus of 1.0% altogether, 0.7% after laparoscopic appendectomy, and 1.0% after open appendectomy.
Incisional Hernia
Four studies reported on incisional hernia (32, 38, 44, 56). The bias assessment resulted in a median of five (range, 3–5) stars. All the studies were retrospective cohort studies with a median population size of 2124 (range, 755–4523) patients and a median follow-up period of 6.5 (range, 1.9–10) years.
The median prevalence of incisional hernia in the studies was 0.7% (range, 0.5%–0.8%). In all four studies, the data were based on review of medical records and not on any surgical or medical coding system. Three of the studies only investigated surgically treated incisional hernia after open appendectomy (38, 44, 56). The last study compared the two surgical methods, but all the incisional hernias that occurred in the laparoscopic group were after converted appendectomies and occurred in the McBurney incision (32). Pooling the prevalence showed an estimate of overall prevalence of incisional hernia of 0.7%.
Inflammatory Bowel Disease
The results of the six studies reporting on inflammatory bowel disease are presented in Table 3 (34, 35, 40, 45, 47, 49). The studies had a median bias assessment score of seven (range, 4–8) stars and a median follow-up time of 13 (range, 7–16) years. The median number of patients was 212,591 (range, 3829–709,353) patients, and three studies had comparison groups, in which the median number of controls was 212,218 (range, 3829–212,963) persons.
Inflammatory bowel disease.
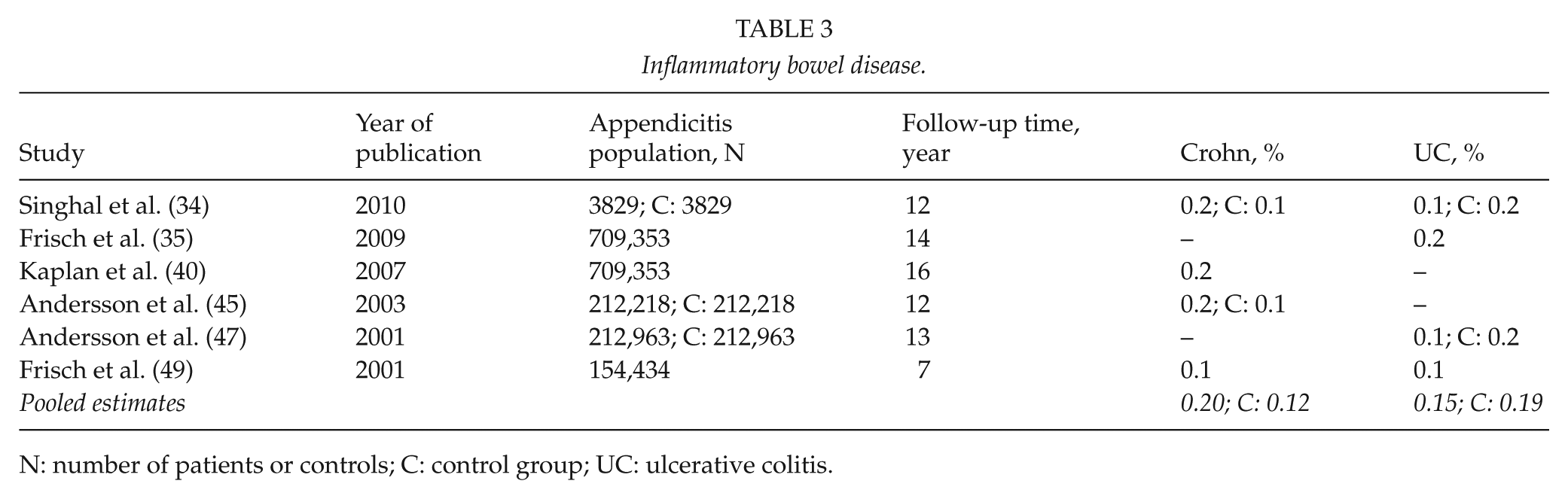
N: number of patients or controls; C: control group; UC: ulcerative colitis.
Four studies examined ulcerative colitis, two retrospective and two prospective cohort studies (34, 35, 47, 49). The median prevalence of ulcerative colitis was 0.1% (range, 0.1%–0.2%). Two of the studies had control groups (34, 47). One reported a protective effect of appendectomy with a HR of 0.74 (95% CI: 0.64–0.86) (47), and the other reported twice as many cases of ulcerative colitis in the control group compared with the appendectomy group (34). Pooling the prevalence showed an estimate of overall prevalence of ulcerative colitis of 0.15% after appendectomy and 0.19% in the studied controls.
There were four studies reporting on Crohn’s disease, one retrospective (34) and three prospective cohort studies (40, 45, 49). The median prevalence of Crohn’s disease in the appendectomy group was 0.2% (range, 0.1%–0.2%). Two studies had control groups (34, 45). One of them showed an incidence rate ratio of 1.47 (95% CI: 1.24–1.73) in the appendectomy group compared with the control group (45). The other study showed 2.3 times as many cases of Crohn’s disease in the appendectomy group compared with the control group (34). Pooling the prevalence showed an estimate of overall prevalence of Crohn’s disease of 0.20% after appendectomy and 0.12% in the studied controls.
Cancer
Six retrospective studies focused on cancer (20, 21, 24, 25, 46, 51). The studies had a median bias assessment score of seven (range, 5–8) stars, a median follow-up time of 12.6 (range, 1–18.6) years, and a median population of 118,569 (range, 75,979–337,437) patients. Two studies had comparison groups, in which the median number of controls was 282,193 (range, 260,746–303,640) people.
Two studies had matched comparison groups (24, 25). A study with follow-up ranging from 0 to 12 months found an HR on all types of cancers of 4.6 (99.9% CI: 3.81–5.55) in favor of the control group (24). Another study with a follow-up period of 15 years (thus excluding the first 18 months) found an HR of colorectal cancers of 1.14 (95% CI: 1.02–1.28) in favor of the control group (25).
The four other studies did not have matched comparison groups, but they all used the background population to calculate standardized incidence ratios (20, 21, 46, 51). In those four studies, no difference was found regarding the prevalence of the vast majority of the examined cancers in the appendectomy groups compared with the background populations.
Fertility
The five studies reporting on fertility (23, 30, 31, 50, 54) were retrospective cohort studies. The median population in the studies was 9840 (range, 825–76,426) patients, and the median follow-up time was 12.4 (range, 9.6–21) years. The median bias assessment was seven (range, 2–8) stars.
Four of the studies had comparable outcomes and showed an increased pregnancy rate (first birth or first pregnancy) in the appendectomy groups compared with controls. Three of those four studies assessed the adjusted HR for first pregnancy event showing increased pregnancy rates for the appendectomy groups with HRs of 1.20 (95% CI: 1.10–1.31) (30), 1.34 (95% CI: 1.32–1.35) (23), and 1.54 (95% CI: 1.52–1.56) (31), respectively. None of these studies compared perforated and non-perforated appendicitis. In another study, increased pregnancy rate was shown after appendectomy for non-perforated appendicitis with an HR of 1.11 (95% CI: 1.07–1.15) and after removal of a normal appendix with an HR of 1.48 (95% CI: 1.42–1.54), while perforated appendicitis did not show a change in pregnancy rate with an HR of 0.95 (95% CI: 0.88–1.04) (50).
Mortality
There were three retrospective cohort studies reporting on mortality (26, 28, 39). The bias assessment score had a median of five (range, 4–7) stars. The median population size in the mortality studies was 169,896 (range, 127,426–222,886) patients, and the median follow-up time was 5 (range, 1–15) years.
The study with the shortest follow-up (1 year) had the lowest mortality (0.6%) (39), the study with a follow-up of 5 years showed the midmost mortality (1.8%) (28), while the study with the longest follow-up (15 years) had the highest mortality (7.6%) (26).
All three studies compared laparoscopic with open approach. Altogether, the mortality in the studies was median 1.7% (range, 0.6%–7.6%). The study with 5 years of follow-up calculated standardized mortality ratios by using expected survival estimates from the Swedish population (28). They found a lower than expected number of deaths for the exposed cohort (appendectomy) compared with the background population. The difference in mortality was most distinct for non-perforated appendicitis with a standardized mortality ratio of 0.71 (95% CI: 0.67–0.75).
The median mortality was 0.9% (range, 0.3%–3.6%) for the laparoscopic approach and 1.8% (range, 0.6%–8.6%) for the open approach. In two of the studies, the mortality was significantly lower in the laparoscopic group compared with the control group (28, 39). In the last study, the difference in mortality between laparoscopic and open approach was only significant for the long-term mortality up until 5 years of follow-up (26).
Discussion
We found that ileus and incisional hernia were uncommon long-term surgical complications after appendectomy, but the results may point at a lower risk of ileus after laparoscopic appendectomy compared with open appendectomy. The few available studies on incisional hernia did not uniformly include clinical examination of patients and the reported prevalence should therefore be interpreted with caution. Still, the results showed a low prevalence of incisional hernia after open appendectomy, which is in line with the findings after laparoscopic appendectomy (4). Appendectomy increased the prevalence of Crohn’s disease but reduced the rate of ulcerative colitis, though none of these results were significant. This is in line with previous studies (57, 58). Since the appendix is an organ with a large number of immune cells (6), it seems possible that an appendectomy can impact the development of inflammatory bowel diseases, though the reason for the contradictory effects on the pathogenesis still is not uncovered. It is suspected that the higher prevalence of Crohn’s disease, especially shortly after appendectomy, might be due to difficulties diagnosing an incipient Crohn’s disease (49).
Most of the studies that focused on cancer after appendectomy showed no increase in prevalence of the cancers that were examined. One study that examined all types of cancers showed a significantly higher prevalence in the appendectomy group but had the shortest follow-up time of 1 year and thereby no washout-period. This suggests that appendectomy in these patients did not treat appendicitis but instead was a warning of a cancer elsewhere.
Appendectomy did not impair fertility, not even in perforated disease. Fertility has also been examined in a previous review, with which our findings agree. Furthermore, we found the mortality after appendectomy to be low, though increasing with longer follow-up. Over time, more people in a given group will die, which reflected our findings. Furthermore, as more time passes after the appendectomy, the risk of dying from other reasons than appendectomy increases.
This systematic review has several strengths. The search was conducted systematically, and a medical research librarian was consulted. A protocol was registered at PROSPERO to keep stringency and thoroughness throughout the study. Furthermore, the screening was conducted by blinded reviewers, who solved discrepancies as they were encountered. We followed the PRISMA guidelines to ensure transparency of the methods of our systematic review. The risk of bias was medium to low, which suggested our conclusions from this systematic review to be reliable. However, our study had some limitations as well. Because some of the studies lacked a precise definition of appendicitis, it is possible that there could have been other reasons for appendectomy than acute appendicitis. Also, the studies that had a precise definition of appendicitis used different coding systems due to differences of time periods and countries. The main coding systems used in the studies were the International Classification of Diseases, 9th Revision; the International Classification of Diseases, 10th Revision; and Nordic Medico-Statistical Committee (NOMESCO) (16–18), which on the other hand is a strength because of the generalizability between the studies using coding systems. The studies’ definitions of some of our outcomes varied among the included studies. In some studies, ileus was limited to only surgically treated cases of ileus, and in other studies, all types of ileus were included. Another limitation was that the report on incisional hernias did not uniformly examine the patients clinically for a hernia, which may have underestimated the prevalence of hernias considerably (59). Furthermore, there is a risk of language bias in our systematic review, since we only included articles written in Danish, English, German, Norwegian, and Swedish. When conducting a systematic review, there is always a risk of publication bias, as inconclusive or negative results may not be published, and therefore, we could have missed some studies.
In conclusion, our systematic review found a low prevalence of long-term complications after appendectomy for acute appendicitis. Most of the included studies focused on obstructive ileus after appendectomy and showed a low prevalence, though it was not possible to demonstrate a significant difference between laparoscopic and open approach based on the available studies. We also found a reduced prevalence of ulcerative colitis and an increased prevalence of Crohn’s disease, respectively, that might indicate differences in underlying pathogenesis of the diseases, which is an interesting subject for further research. Finally, the fear of impaired fertility especially after perforated appendicitis may not be justified based on the available data.
Supplemental Material
Supplementary_material – Supplemental material for Long-Term Complications of Appendectomy: A Systematic Review
Supplemental material, Supplementary_material for Long-Term Complications of Appendectomy: A Systematic Review by T. Rasmussen , S. Fonnes, J. Rosenberg in Scandinavian Journal of Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.