
Abstract
Background
Laparoscopic Surgery is performed using carbon dioxide gas insufflated into the abdominal cavity to create a space for endoscopic visualization. During a laparoscopic surgical dissection plume is formed from electrocautery dissection. This plume contains viruses and sometimes COVID-19 viruses. The plume obscures the visual field. The unfiltered plume release is dangerous to surgeons, nurses, and patients. The loss of visualization during carbon dioxide release delays surgery. The use of carbon dioxide insufflated gas can have side effects such as C02 embolus, pain from diaphragmatic stretching, physiological complications such as respiratory infections and renal problems. The release of carbon dioxide gas into the atmosphere, unfiltered is significant. This accounts for 7% of greenhouse gases globally. This percentage is rising due to expansion of minimally invasive surgery.
Methodology
The proposed system for gasless surgery was designed by algorithms of tensegrity and geodesic dome pressures.
Experiment results
100 simulator studies were performed to develop the device to elevate the abdominal wall to create a gas free (isobaric) space for Laparoscopic Surgery. After design freeze, 4 animal studies were performed using ethical research guidelines at Amsterdam Medical Centre Research Department, Netherlands. 3 cadaveric studies were performed using Ethical guidelines at Hackensack University Medical Centre, New Jersey, USA, to evaluate the device in a human setting.
Conclusions
These devices for Laparoscopic Surgery, Robotic Surgery, and Hand Assisted Laparoscopic Surgery (HALS) successfully proved that a superior intra-abdominal space can be created without carbon dioxide insufflation. The devices are patented in USA and Europe.
Introduction
Laparoscopic Surgery requires carbon dioxide gas insufflation into the abdominal cavity to create a space. The space created allows the surgeon a visual field to perform surgery. The volume of carbon dioxide used to distend the abdomen is significant. This gas is released into the environment unfiltered during and after surgery. This volume of gas release from surgery is globally equivalent to 7% of greenhouse emissions. 1 Laparoscopic Surgery is associated with complications such as C02 embolus, post operative pain and respiratory complications such as pneumonia. Increasingly, older patients are undergoing Laparoscopic Surgery. There are more complications in this group due to carbon dioxide insufflation. 2
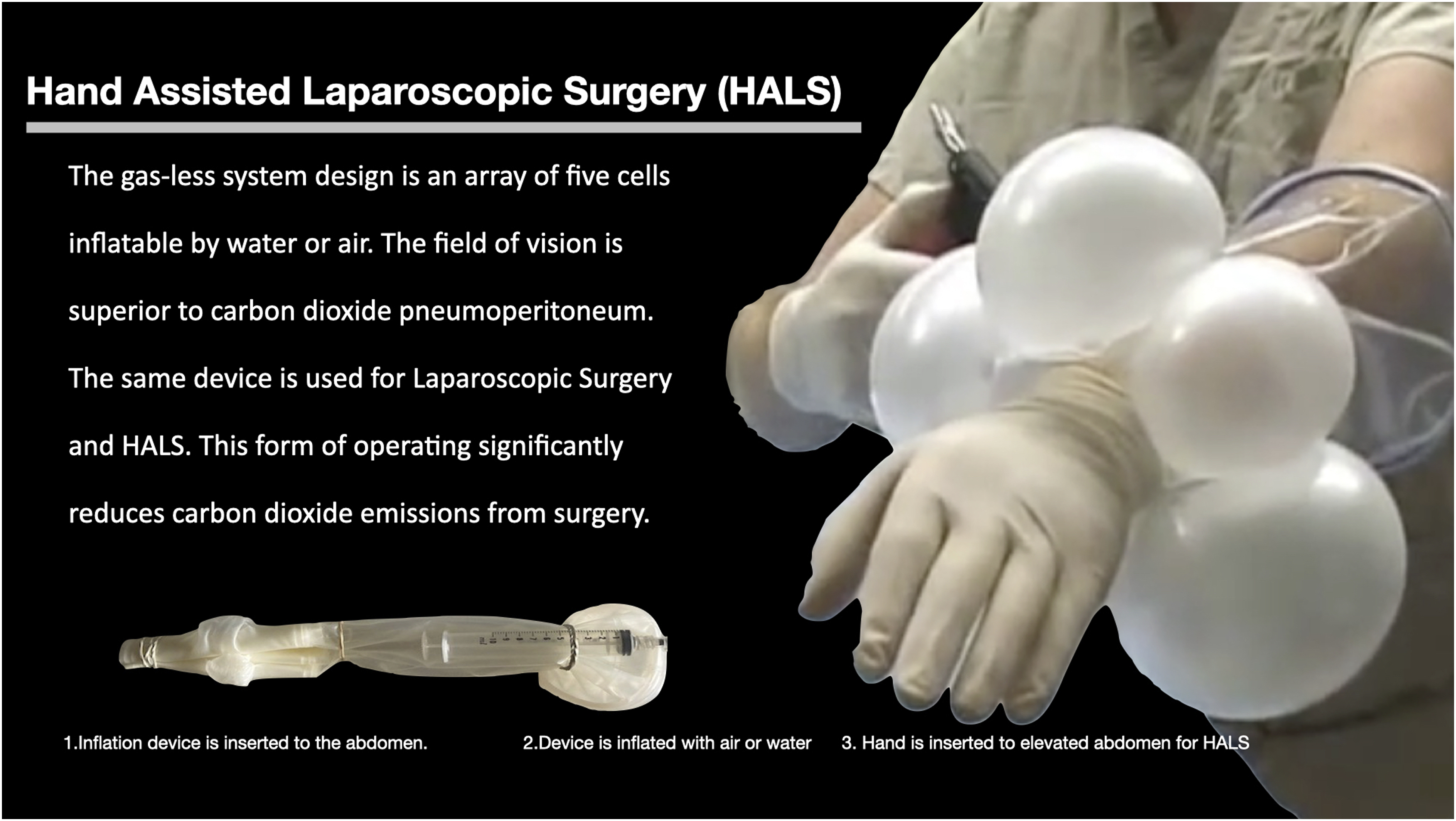
Cancer cells may be spread from carbon dioxide insufflation. 3 Hand Assisted Laparoscopic Surgery (HALS) was introduced in 1991. This development helped to make advanced Laparoscopic Surgeries safer procedures. 4
The interruption of surgery due to plume formation and evacuation, and unfiltered gas release is dangerous to surgeons, nurses, and patients. The unfiltered release of carbon dioxide during surgery is a major environmental concern.
To address these concerns, we have developed a system of inflatable cells that can create a space for all Laparoscopic, Thoracoscopic surgery, Robotic and Hand Assisted Laparoscopic Surgery without using carbon dioxide gas.
Consequently, the proposed system can replace carbon dioxide use to create a space in the abdominal or thoracic cavity for all Laparoscopic surgery.
System Design
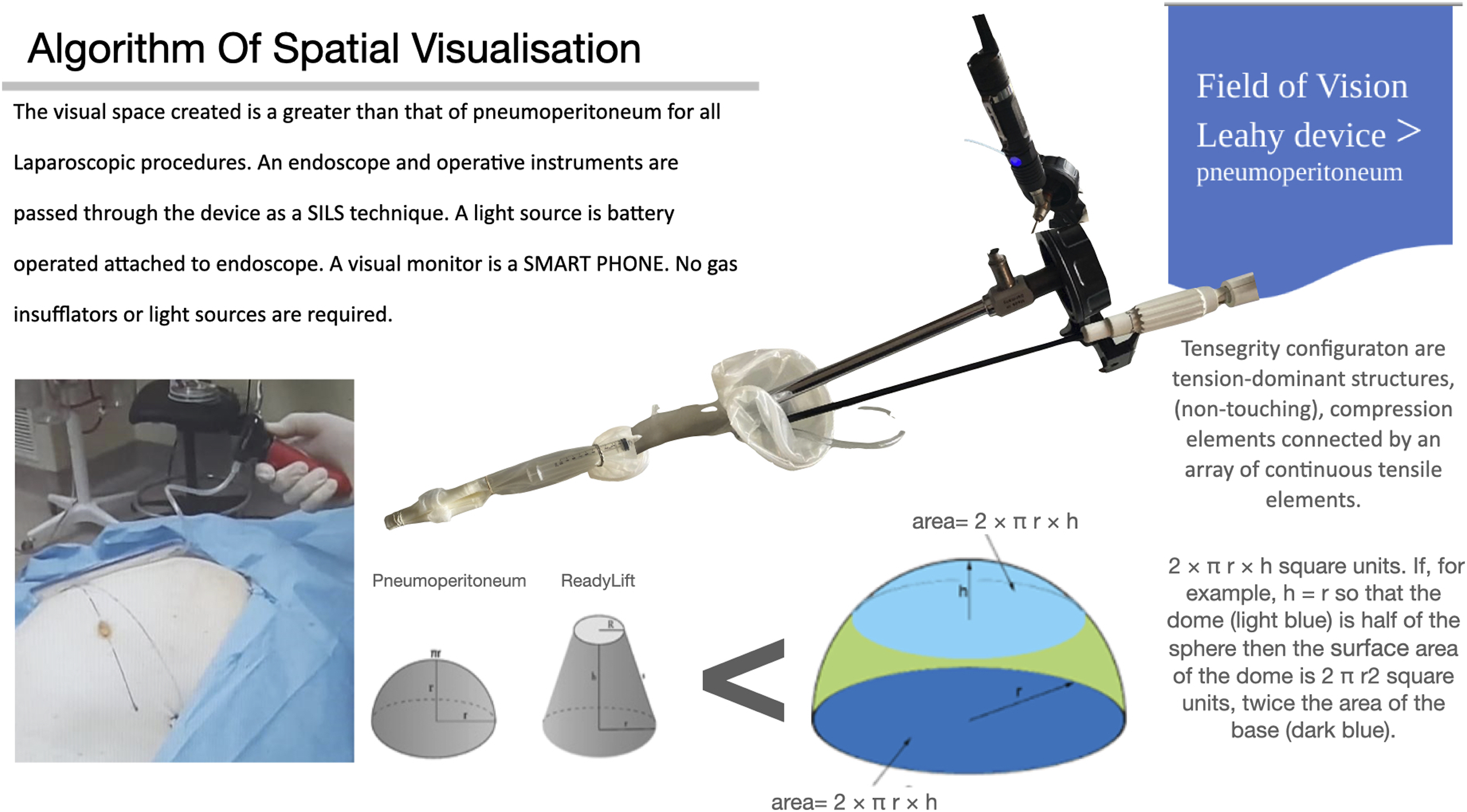
The figures below show the attributes of the system design, such as the single incision, the inflated gas-less Hand Assisted Laparoscopic application and the geodesic design equations providing a greater volume of spatial visualization of the inflated abdomen. An array of five cells inflatable by water and air/inert gas distends the system to allow the cells to gently elevate the overlying abdominal wall. The space created gives the visual field for Laparoscopic procedure. The space created by pneumoperitoneum is semicylindrical. The space created by the isobaric device is based on formulae of geodesic dome formation and tensegrity.
The inflating water or air is never in contact with bodily secretions or organs. The inflatable cells also function as retractors. The dome shaped device has low pressure coefficients to minimize pressure on the abdominal wall and organs. The device is designed for Single Incision Laparoscopic Surgery (SILS). The field of vision is superior to carbon dioxide pneumoperitoneum. It has a greater space than Keyloop, mechanical elevator. 5
An endoscope and operative instruments are passed through the device as a SILS technique. A light source is battery operated attached to endoscope. A visual monitor is Smart phone. No gas insufflators/light sources are required. This method permits Laparoscopic/Thoracoscopic surgery in all operating rooms and Mobile Army Surgical Hospital (MASH). The plume caused by dissecting electrocautery is rapidly evacuated using a filtered plume evacuator. There is no loss of visual field because the abdominal space is Gas-Less Figures 1-3. Isobaric laparoscopic surgery. Hand Assisted Laparoscopic Surgery (HALS). Algorithm of spatial visualisation.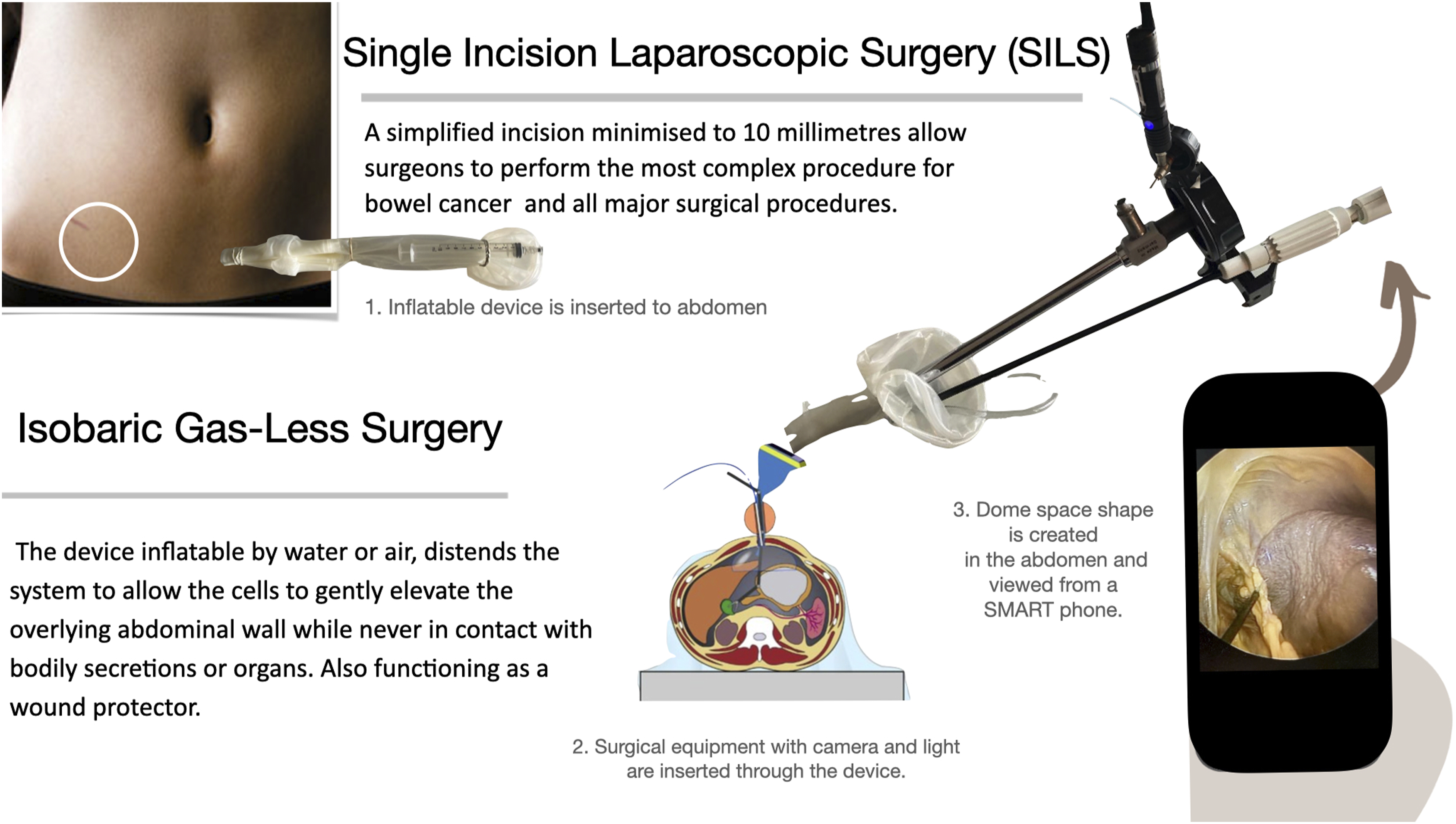
Conclusion
In this study we proposed an alternative to carbon dioxide insufflation to create a pneumoperitoneum. The resulting success of a Gas-Less (isobaric) system has achieved two patent grants in USA and two patent grants in Europe. The system is for all Laparoscopic/Robotic/Thoracoscopic surgery, the other is for Hand Assisted Laparoscopic Surgery (HALS). The use of Smart Phone technology to visualise and record reduces the dependence on dedicated operating rooms. Surgical cost reduction up to 60% is achievable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
US Patent Number: 8,192,358.
US Patent: 8579989.
Europe Patent Number: 1742586.
European Patent Number: 1617770.
Clinical Trials
Clinical trials commence in September 2023.