
Abstract
Background and Aims:
This study compared the three most used composite flaps in maxillofacial reconstructions in our institute.
Patients and Methods:
Between 2000 and 2012, a total of 163 patients with mandibular, maxillary, and orbital defects received either scapular, fibular, or iliac crest osseal reconstructions in Helsinki University Hospital, Departments of Plastic Surgery and Maxillofacial Surgery. Data regarding the patient demographics, complications, and outcomes were analyzed.
Results:
There were 92 deep circumflex iliac artery flaps (56%), followed by 42 scapular (26%) and 29 fibular flaps (18%). The rate of flap loss was the highest in the deep circumflex iliac artery group (p = 0.001). Reconstructions using fibula were fastest (p = 0.001) and had lowest perioperative blood loss (p = 0.013). There were no significant differences in the number of early or late complications between the flaps, but donor site complications were more severe in deep circumflex iliac artery. Osteotomies as well as dental implants were safely performed in all flaps with equal results.
Conclusion:
All three flaps of this study can be performed with awareness of the deep circumflex iliac artery flap being the least reliable alternative. The knowledge of the advantages and disadvantages of several osseal-free flap alternatives is beneficial in selecting the best suitable method for each individual patient requiring maxillofacial osseal reconstruction.
Introduction
Free flaps have become an established method in treatment of complex head and neck defects (1, 2). Defects including osseous facial structures still form a surgical challenge. To restore functional and anatomical characteristics of the area, the reconstruction must be performed with suitable tissue, in many cases a composite flap. Composite flaps have been introduced in wide use already decades ago (3). Still, it has been postulated that osseous free flaps carry higher mortality than soft-tissue free flaps (4). Complications related exclusively to maxillofacial reconstructions include osteonecrosis and fistulas. Flap-specific donor site considerations must also be taken in account in case of bone harvesting. The opinions on superiority of the one flap compared to another are divided and the flap selection is often dependent on surgeons’ personal preference.
The fibular free flap is a versatile flap, which due to its many advantages is generally considered the most popular alternative for maxillofacial reconstruction (2). It provides a good length of vascularized bone with possibilities for osteotomies and is easily contoured to fit orofacial bone defects (5). The elevation of the flap can be done simultaneously with reconstruction site preparation without adding extra duration to the operation. In contrary, the soft-tissue component of the flap and the length of the pedicle are limited (6). In addition, in the elderly population, the use of fibular flap may also be compromised by peripheral atherosclerotic disease, and evaluation of the vascular status is essential to prevent donor site morbidity. Otherwise fibular donor site is well tolerated, but chronic pain and reduced mobility and muscle strength can occur (7).
The iliac crest (deep circumflex iliac artery, DCIA) osseal flap harvested from the groin area provides a good stock of bone and soft-tissue material. The bulkiness and limited size of skin island might cause precautions in maxillofacial reconstructions. Occasionally, the pedicle is of limited length and might require additional vein grafting. The donor site complications include chronic pain, hernias, gait problems, and fractures of the anterior superior iliac spine (8).
The scapular osseal flap has a versatile bone stock and can be harvested in different manners to fit wide range of maxillofacial defects. The flap can be elevated with a circumflex scapular pedicle or a thoracodorsal angular pedicle (9). In addition, the scapular flap provides broad alternatives of soft-tissue reconstruction in comparison to fibular and DCIA flaps, and the donor site is well tolerated. The subscapular vasculature is seldom affected by atherosclerotic disease (10). The posterior location of scapula has been considered disadvantageous, as there would be a need for repositioning the patient when harvesting the flap. Anyhow, in our institution, we nowadays perform the procedure positioning the patient in a tilted decubital position, also described by other institutes (11). Concerns have been raised regarding the bone material of the scapular flap, especially when planning dental implant therapy (4, 12).
In this study, we compared retrospectively perioperative factors; donor site morbidity; and complications and outcomes of fibular, scapular, and DCIA osseal flaps in maxillofacial reconstructions in our institution.
Patients and Methods
Between 2000 and 2012, a total of 163 consecutive patients went through microvascular reconstructive surgery due to defects of mandible, maxilla, and orbit. The majority of the patients were treated with oncological intentions, but also traumatic lesions and benign tumors were included. All the oncological patients were evaluated in the multidisciplinary head and neck tumor board in Helsinki University Hospital. The surgeries were performed in the Departments of Maxillofacial Surgery and the Department of Plastic Surgery, by teams comprised of maxillofacial surgeons, plastic surgeons, and ENT doctors. Hospital charts were analyzed regarding the preoperative, postoperative, intraoperative, and follow-up data retrospectively during the years 2014–2016. Patient data are given in Table 1.
Patient data.
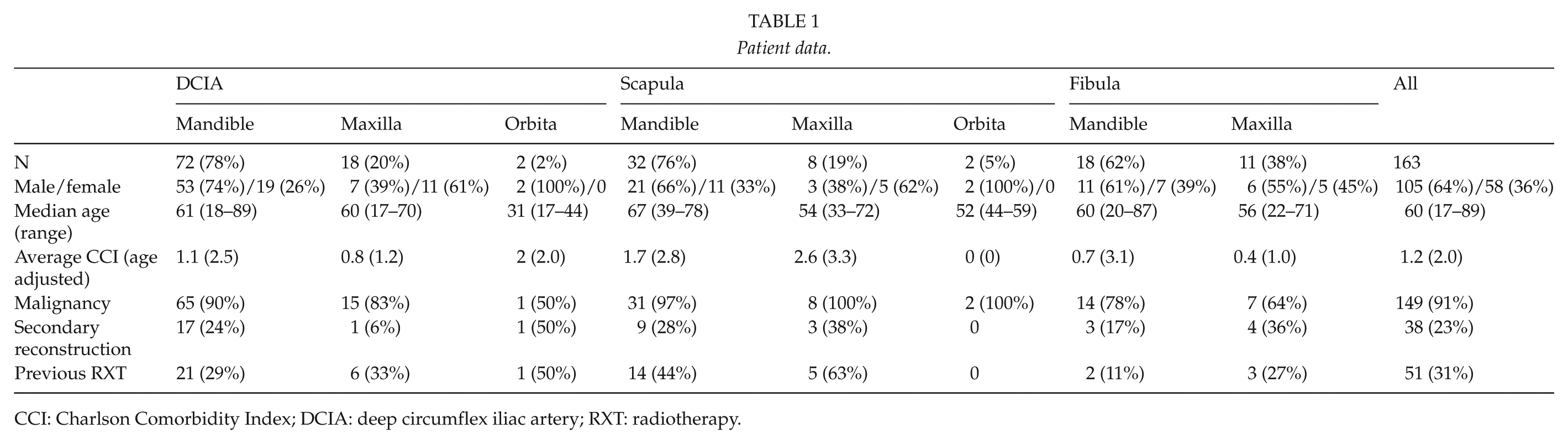
CCI: Charlson Comorbidity Index; DCIA: deep circumflex iliac artery; RXT: radiotherapy.
Preoperative data regarding patient demographics, smoking, previous oncological treatment, comorbidities, and previous microvascular reconstruction was assessed. Perioperative data were collected featuring operation time, blood loss, and surgical technique. We recorded the formation of early reconstruction site complications with vascular re-operation, wound dehiscence, postoperative hematomas, and infections leading to possible partial or total flap necrosis, early donor site–specific complications and late reconstruction, and donor site–related complications appearing more than 30 days after the initial operation. Postoperative oral function was recorded regarding speech and oral feeding.
The Institutional Research Ethics Board of the Helsinki University Hospital approved this study.
Statistical Methods
Data were statistically analyzed with SPSS 21 (IBM, Armonk, New York, USA). We used Kruskal–Wallis and chi-square test to analyze categorical data and Mann–Whitney U-test for assessments for comparison of groups of continuous data. Results are given in median and range.
Results
Preoperative Results
A total of 163 patients received microvascular osseous composite reconstructions during the follow-up period. Of the reconstructions, 122 were performed for mandibular, 37 for maxillary and 4 for orbital defects. In both mandibular and maxillary reconstructions, DCIA was the most frequently used flap (59% and 49% of the patients, respectively), followed by scapula (26% and 30%, respectively), and fibula (15% and 21%, respectively). Four orbital defects were reconstructed with two DCIA and two scapular flaps (Table 1).
There were no statistically significant differences found between demographic data and the three different flaps. Patients with mandibular reconstructions (median, 61 years; range, 18–89 years) were slightly older than patients with maxillary reconstructions (57 years, 17–72 years) or orbital reconstructions (44 years, 17–59 years), p = 0.01. The average Charlson Comorbidity Index (CCI) for all patients was 1.2 and the age adjusted CCI was 2.0. There was a tendency for lower CCI in fibula group and higher CCI in scapula group, p = 0.076 (Table 1).
Almost every fourth reconstruction in all groups was a secondary microvascular reconstruction. Indication for the re-reconstructions was mostly recurrent malignancy. Malignant diseases covered over 90% of all the reconstructions, and approximately one-third of the patients had received previous radiotherapy. Fibula was the most commonly used flap in non-malignant cases (Table 1).
Peri-And Postoperative Results
The fibula had the shortest and scapula the longest median operation time (p = 0.001). The operations with fibula had also the least blood loss during the operation (p = 0.013; Table 2).
Perioperative results.
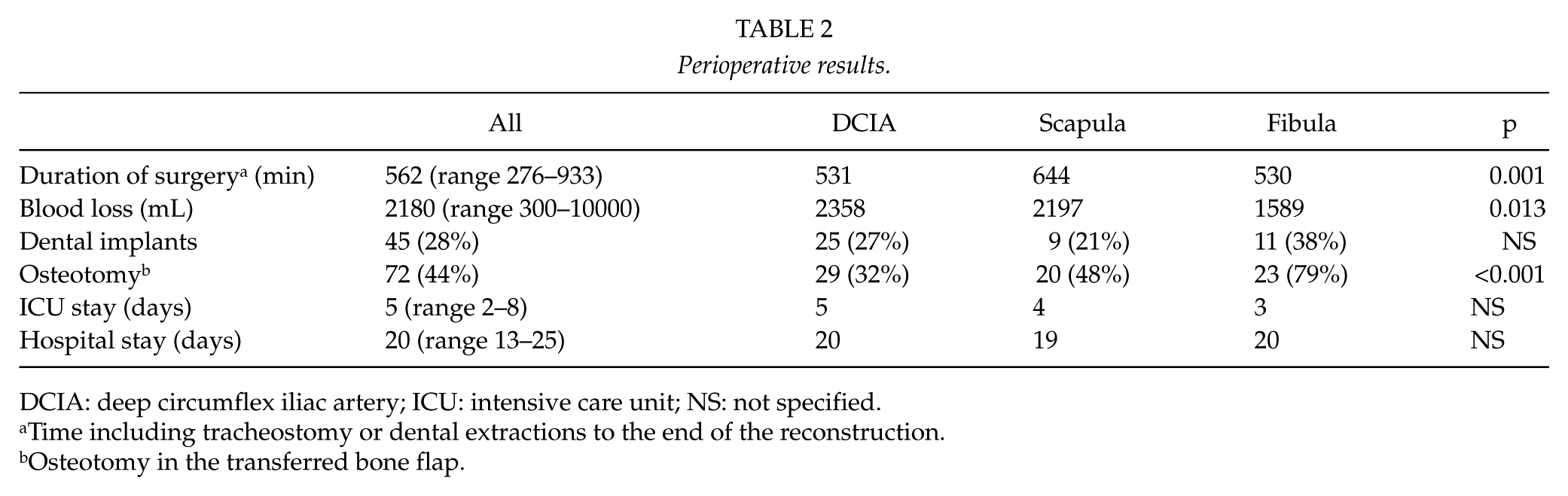
DCIA: deep circumflex iliac artery; ICU: intensive care unit; NS: not specified.
Time including tracheostomy or dental extractions to the end of the reconstruction.
Osteotomy in the transferred bone flap.
Osteotomies were performed in 44% of the flaps, and 15 flaps (9%) had multiple osteotomies. Osteotomy was performed most often in fibula and the least in DCIA. Dental implants were applied for every fourth patient, and there was no significant difference between flap type and implantation rate. Moreover, there was no significant difference between the length of ICU and hospital stay between flap types (Table 2).
Complications
There were 14 total flap failures during the study period (8.6%). Most of the failures were DCIA flaps (n = 13, 14%), and DCIA failed more often in maxillary (5/18, 27.8%) than mandibular position (7/72, 9.7%), p = 0.025. In addition, one orbital DCIA failed. Six of the flap failures occurred during the year 2004, one fibula and five DCIA flaps. Excluding the year 2004, the flap failure rate was 5% (n = 8). The difference in DCIA flap losses compared to other flaps was statistically significant (p = 0.001), also excluding the year 2004 (p = 0.038).
The complications were analyzed as early (within 30 days postoperatively) and late (later than 30 days). Early reconstruction site complications, including total flap failures, occurred in approximately every fourth mandibular (n = 34, 28%) and maxillary reconstruction (n = 10, 27%). The DCIA early complications included 13 total flap failures (14%), 7 partial flap necrosis (8%), 2 postoperative bleedings (2%), 2 saved anastomosis occlusions (2%), and 1 early infection (1%). Scapular early complications were two partial skin island losses (5%), six fistulas (14%), two bleedings (5%), and three saved anastomosis occlusions (7%). Fibular flap early complications were one total flap loss (3%) and three partial skin island losses (10%), and one saved arterial occlusion (3%; Tables 3 and 4).
Mandibular reconstruction site complications.
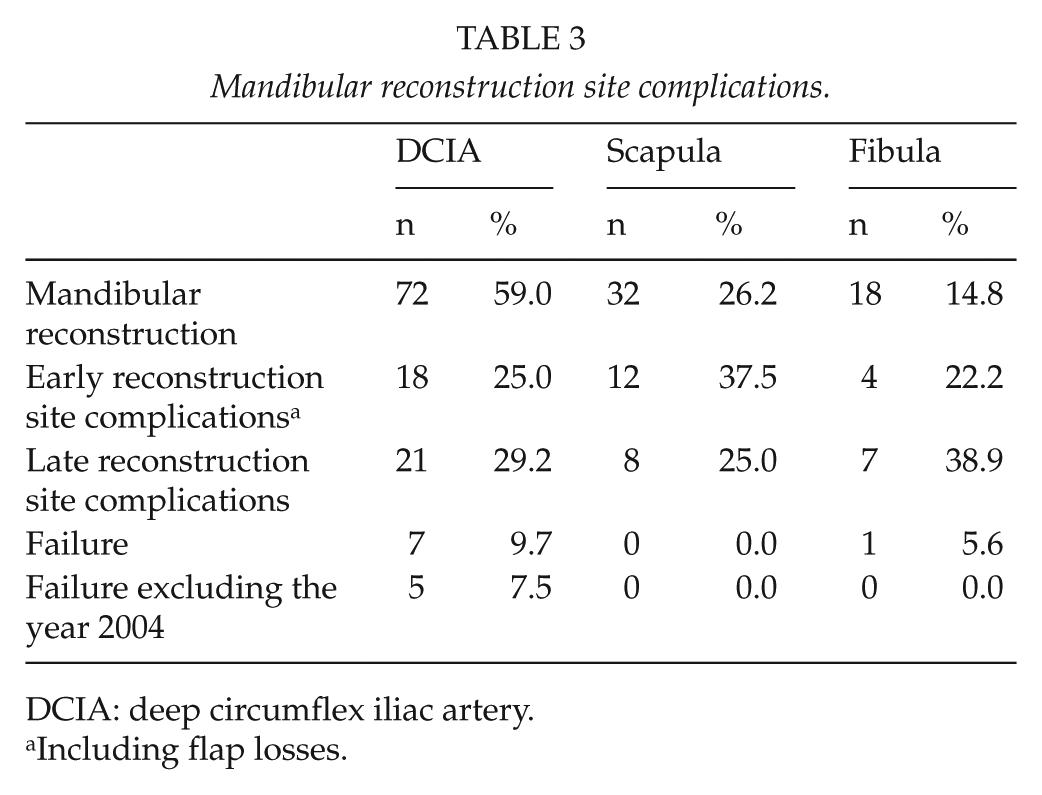
DCIA: deep circumflex iliac artery.
Including flap losses.
Maxillar reconstruction site complications.
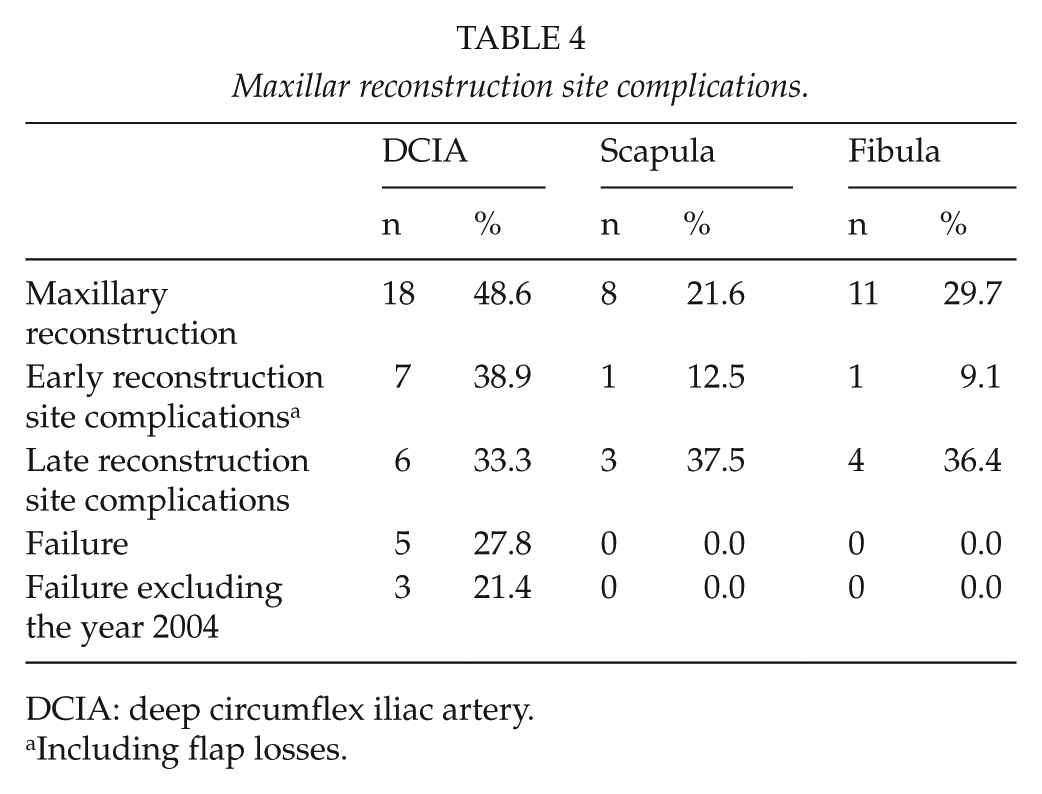
DCIA: deep circumflex iliac artery.
Including flap losses.
Late reconstruction site complications presented in 30% of mandibular reconstructions (n = 36) and 35% of maxillary reconstructions (n = 13). In DCIA, there were 23 fistulas (25%), 2 flap osteonecrosis (2%), and 2 non-unions (2%). Scapular flaps had 10 fistulas (24%) and 1 mandibular osteonecrosis (2%). In fibular flaps, there were five fistulas (17%), four non-unions (14%), and two flap osteonecrosis (7%; Tables 3 and 4).
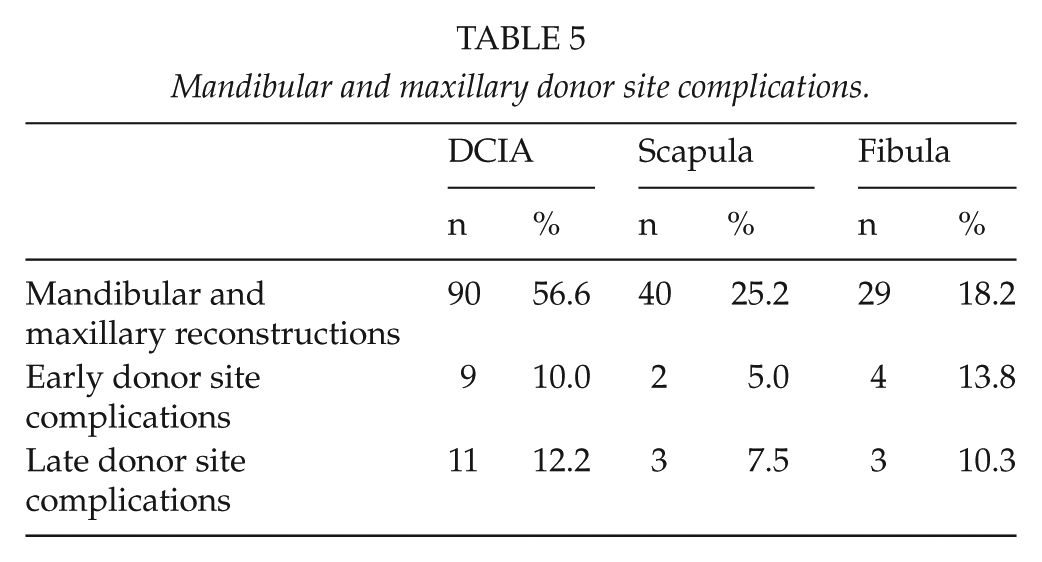
Early donor site complications occurred in 26% of reconstructions (n = 43). DCIA harvesting resulted in three bleedings, three hernias, two anterior iliac spine fractures, and one partial femoral nerve paresthesia. In the scapular donor area, there were one seroma formation and one severe postoperative pain. Fibular flaps had four early donor site complications, of which two were infections, one lower leg ischemia due to an undetected vascular anomaly, peroneus magna, and one compartment syndrome due to over-tight wound closure (Tables 3 and 4).
Late donor site complications were present in 10% of cases (n = 17). In DCIA flaps, there were four late hernias (4%), three anterior iliac spine fractures (3%), one seroma (1%), and one chronic pain syndrome (1%). In scapular flaps, impaired range of motion of the scapula was seen in four patients (10%). Fibular reconstructions with late donor site complications included two cases of chronic pain (7%) and one exposure of peroneal tendon (3%). There were no statistically significant differences between the groups in donor site complications (Tables 5).
Mandibular and maxillary donor site complications.
Dental implants were installed in 25 DCIA reconstructions, and five patients had a single implant failure (20%). Of nine scapular implantations, one implant failed (11%), and of the 11 fibular implantations, three failed (27%). There were no statistical differences between the flap type and implant failure (p = 0.38).
Complication-Related Factors
All patient and reconstruction site complications were analyzed against preoperative risk factors including age, gender, CCI score, smoking, previous microvascular reconstructions, and radiotherapy. Perioperative factors such as duration of surgery, bleeding, and osteotomies of the microvascular flap were recorded. Previous radiotherapy significantly correlated with postoperative complications (p = 0.009). Comparing the rate of overall complications to the age of the patient, a statistically significant relation was found between the groups, but the age was higher in the non-complication group (p = 0.028). The duration of the operation, perioperative bleeding, osteotomy in the flap bone, CCI score, previous microvascular reconstruction, gender of the patient, or smoking did not correlate with complication.
There was no difference in number of osteonecrosis, fistulas, or non-unions between the non-osteotomized flaps and single osteotomy flaps (25% vs 23%, respectively). However, there was a tendency for risk of complications in flaps with more than one osteotomy, since 47% of these flaps developed some of the abovementioned complications. The sample size was limited in this group (n = 15, p = 0.616).
Discussion
In this study, we compared the use of three different composite free flaps, fibula, scapula, and DCIA, in maxillofacial reconstructions in 163 patients. To our knowledge, this is the first study to compare clinical findings between these three most commonly used free flaps in maxillofacial reconstructions. In previous reports, the comparison has been limited to two different flaps, most commonly to fibula versus scapula or fibula versus DCIA (13–15).
In our material, the DCIA flap was the most used flap, especially in the beginning of this series because it was the first microvascular reconstruction used in the Department of Maxillofacial surgery, where the majority of the mandibular reconstructions were done. In contrast, in the Department of Plastic Surgery, the scapula has been the most commonly used flap. There are major differences between different centers in the practice of selecting a flap (16). Oncological indications dominated in our data, and 90% of the cases were for cancer surgery. This is in line with other maxillofacial centers (1). We used the fibula more often in non-oncological cases and for maxillary reconstructions. However, some centers prefer using the angle of the scapula in anterior maxillary reconstructions (17, 18). The decision-making of which composite flap to choose for facial reconstruction, has often been based on subjective preferences of the surgeon and not scientific facts.
The shortest duration of surgery was in the fibular reconstructions and the longest in the scapular reconstructions. The fibula and the DCIA are all harvested in a two-team approach, whereas the scapula is often, but not always raised simultaneously with the resection. Moreover, the close proximity of the resection team makes the two-team work more crowded and slower. Perioperative blood loss was lowest in the fibular group, partly explained by the possibility to raise the flap using a tourniquet. In the scapula, the largest blood loss in our series is probably related to the larger resections and in using more often chimeric flaps with muscular or fasciocutaneous component.
The year 2004 was an outlier regarding the flap losses. The majority of the losses during 2004 were due to late arterial thrombosis. The suddenly increased presentation of this rare complication was found to be associated with the use of a COX-2-selective painkiller (19). Overall flap survival in this study was 91.4% and excluding the year 2004 95.1%, which are in line with generally presented survival rates in modern head and neck microsurgery. Excluding the DCIA, the flap survival rate for the fibulas and the scapulas was 98.6%. We have previously reported in our institution a flap survival rate of 96.9% in head and neck reconstructions in 594 flaps including all flap types (20). Therefore, the survival rate for osseal flaps is within the same range as for fasciocutaneous flaps.
In previous reports, the scapula has been shown as a reliable flap, and we had the same finding with no lost scapular flaps (21, 22). The DCIA flap was lost significantly more frequently than scapula and fibula. In a review of mandibular free flaps by Markiewicz in 2015 analyzing 1221 patients with 1262 flaps, the total flap survival was 94.8%. In their study, the DCIA had the highest odds ratio (OR) for flap losses of all flaps with OR = 1.73 compared to all other flaps and OR = 7.4 comparing to the radial forearm (23). On the basis of our results and the literature, we conclude that DCIA flap is not as reliable as the fibula or the scapula.
There were no statistical differences between fibula, scapula, or DCIA in the number of early or late reconstruction site-specific complications. There was a tendency for less early reconstruction site complications for fibula, but this may be related to fibula group having more non-oncological cases and lowest median CCI-index in our series. In addition, there were no significant differences in the number of reconstruction site complications between mandibular and maxillary reconstructions. Winters et al. (24) compared DCIA to fibula in mandibular reconstructions and concluded that both donor and recipient site outcomes favor fibula over DCIA. Hasan et al. (18) concluded, based on complications, that the scapula is the most favorable option. On the other hand, Brown et al. (25) and Urken et al. (26) prefer the DCIA with few complications, and Takushima (27) and Frederick et al. (28) stated that all flaps are good candidates with similar rates of complications and reliable results.
There were no statistical differences between the groups in the number of early or late donor site complications, but there was a tendency for less early donor site complications in the scapula group. However, there were differences between severities of the donor site complication between the groups. There were two major lower leg sequels in the fibula group with ischemia and compartment syndrome. These complications could have been prevented with computed tomography (CT)-imaging which is routine nowadays and with more careful postoperative monitoring. The complications associated with DCIA were more severe including anterior iliac spine fractures and hernias. In the scapula group, the donor site complications were overall less severe than in the other groups. In our series, we report that the number of donor site complications is in the same range in all three flaps but less severe in scapula.
In our study, previously irradiated patients had significantly more complications as also shown by others (29, 30). In addition, age of the patient correlated statistically significantly with complications. Surprisingly, patients without complications were older than those having a complication. We conclude that elderly patients altogether tolerate large reconstructions with good postoperative treatment in the recovery, and advanced age is generally no longer an independent contraindication for extensive reconstructive surgery (31, 32). Several pre- and perioperative parameters including gender, previous microvascular reconstructions in the same area, duration of the surgery, blood loss during surgery, and performed osteotomy in the osseous flap were analyzed in relation to flap survival and complications, but no statistical significances were found. Our findings demonstrate that most significant risk factor for a complication is previous radiotherapy.
There has been ambiguity regarding relation between complications and osteotomies (9, 26, 33). In our study, the performance of osteotomy did not affect general flap survival. However, in the group of several osteotomies, there was a tendency for higher incidence of osteonecrosis, fistulas, and non-unions. Most of the flaps with several osteotomies were fibulas, and it is generally postulated that segments should be at least 3 cm of size, which is also the general practice in our institute. Conclusions regarding differences between the flaps concerning multiple osteotomies are not possible to make based on this study, due to the heterogeneity of the three groups.
Based on our data, all three flaps seem to perform well with dental implants. The proportion of implants installed and lost was similar between groups and shows that implants can be used in any of the presented flaps as also stated in the literature (9, 16, 34).
Conclusion
This work describes the results of fibula, scapula, and DCIA in maxillofacial reconstructions in a single-center setting. In our series, DCIA was less reliable and had more flap losses than fibula or scapula, which were extremely reliable. Reconstructions with fibula were faster and bled less than reconstructions with scapula or DCIA. There were no differences between frequency of early or late complications in reconstruction site or donor site between these flaps, but donor site complications were less severe in scapula. We conclude that knowledge of these three different alternatives ensures the optimal flap choice in osseal maxillofacial reconstructions for individual patient, but there should be caution when choosing DCIA.
Footnotes
Acknowledgements
T.W. and A.H. contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Research Ethics Board of the Helsinki University Hospital approved this study (reg. no. 123/13/03/02/2011).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.