
Abstract
Background:
Routine prophylactic abdominal drains after laparoscopic appendectomy for perforated appendicitis in children are still controversial. Throughout the history of surgery, potential benefits of the abdominal drains have been described. However, in recent studies, no benefits were observed and serious complications have been reported.
Methods:
From January 2000 to December 2013, all charts of the pediatric patients who underwent laparoscopic appendectomy in our tertiary center were revised. The data from 1736 appendectomies were analyzed. We only included those patients with perforated appendicitis treated with early appendectomy (n = 192). Prophylactic drains were established according to the surgeon’s preference. The sample was divided into two groups, those with drain (n = 117) and those without drain (n = 75). Demographics, operative findings, and postoperative outcomes were analyzed in both groups.
Results:
Of all patients, 121 were male and 71 were female with a mean age of 7.77 ± 3.4 years. There were not statistically significant differences between the groups in gender (p = 0.82) and mean age (p = 0.31). There were no statistically significant differences between the two groups in the rate of intra-abdominal abscess, wound infection, and bowel obstruction. However, the drainage group has been statistically associated with an increased requirement of antibiotic and analgesic medication, fasting time, operative time, and length of hospital stay.
Conclusion:
The prophylactic use of abdominal drainage after laparoscopic appendectomy for perforated appendicitis in children does not prevent postoperative complications and may be associated with negative outcomes. Prospective randomized studies will be necessary to verify this question.
Introduction
The first use of abdominal drainage is attributed to Hippocrates (460–377 BC). Since that time, the use of drains after abdominal surgery has passed through generations of surgeons. In 1887, Lawson Tait defended, “When in doubt, drain.” However, this statement was critically questioned and many surgeons considered more appropriate the words of Halsted in 1898: “The more imperfect the technique of the surgeon the greater the necessity for drainage. No drainage at all is better than the ignorant employment of it.” In 1905, Yates published a study of the use of abdominal drains and he concluded: “Drainage of the peritoneal cavity was physically and physiologically impossible” (1).
During the last decades, surgeons have continued to investigate the utility of drains after gastrointestinal surgery. The postoperative drainage includes therapeutic and prophylactic aspects. The principal functions of prophylactic drains are to remove intraperitoneal fluids like blood, ascites, or intestinal juice and to detect early complications such as postoperative bleed or anastomotic leakage. However, the complications of the drains are numerous: foreign body effects, mechanical problems, physiological issues (pain, emphysema, pneumoperitoneum), or inadequate drainage (2). Hence, the benefits of abdominal drainage still remain controversial.
Perforated appendicitis is more frequent in children than in adults, especially in infants and younger children in whom the rate of perforation can reach 55%–80%. One of the most serious complications of perforated appendicitis is the postoperative abscess formation (3). Several pediatric surgeons are insistent on the use of abdominal drains to avoid these complications. The aim of our study is to assess the efficacy of abdominal drainage to prevent complications after laparoscopic appendectomy for perforated appendicitis in children.
Material and Methods
From January 2000 to December 2013, all charts of consecutive patients who underwent laparoscopic appendectomy in our tertiary medical center were revised. The data from 1736 pediatric appendectomies were analyzed retrospectively. Patients who had an incidental appendectomy during another laparoscopic surgical procedure and those treated with interval appendectomy were excluded. However, patients who needed conversion to open surgery were added. We only included the patients with perforated appendicitis. We defined perforated appendicitis as an identifiable macroscopic hole in the appendix during the surgery.
Laparoscopic findings showed a perforated appendix in 199 cases. From this group, seven patients were excluded because they were treated with drainage and interval appendectomy. The sample was divided into two groups, those with prophylactic drain (n = 117) and those without drain (n = 75). Demographics, operative findings, and postoperative outcomes were analyzed. Both groups were compared for the following operative findings: free purulent fluid, appendiceal phlegmon, generalized peritonitis, surgical technique, operative time, complications, and conversion. The pneumoperitoneum was always established by open approach at the umbilicus. The division of the mesoappendix was performed with electrocautery and the base of the appendix was usually closed extracorporeally or using either endoloops or endostaplers, depending on surgeon’s preference. Free purulent fluid was aspirated and the wounds were primarily closed. Surgery was performed by two pediatric surgeons, usually a resident and a staff. Prophylactic drains were established according to the staff’s choice. When they were used, they were introduced through the right iliac fossa incision into the resection area.
Both groups were compared for the following postoperative outcomes: duration of the use of antibiotic and analgesic medication, timing of oral refeeding, length of hospital stay, and complications such as wound infection, intra-abdominal abscess formation, and bowel obstruction. Upon the recommendations of the Pediatric Infectious Disease Unit, broad-spectrum antibiotics were started at the onset of anesthesia. Intravenous antibiotics were administered for at least 5–7 days postoperatively. The removal of the abdominal drain was determined by the degree of drainage and the surgeon’s preference (usually when it ceased or decreased to 20–30 mL/day). Intra-abdominal abscess was diagnosed by ultrasonography performed by pediatric radiologists. Wound infections were diagnosed by the clinical judgment of the surgeon, on the basis of symptoms such as hyperemia, purulent discharge, swelling, or induration. Bowel obstruction was defined by clinical history, radiological findings, and abnormal physical examination results such as distended abdomen or the absence of flatus.
SAS 9.3 software was used for all statistical analyses. Continuous variables were compared between the groups using Wilcoxon rank-sum test and categorical variables were compared using Pearson chi-square test. A p value < 0.05 defined statistical significance.
Results
Of the 192 pediatric patients, 121 were male and 71 were female with a mean age of 7.77 ± 3.4 years (range 0–15 years). There were 48 boys and 27 girls in the drainage group, and 73 boys and 44 girls in the no-drainage group. In the drainage group, the mean age of the patients was 7.57 ± 3.5 years and in the no-drainage group it was 8.07 ± 3.2 years. There were not statistically significant differences between the groups in gender (p = 0.82) and mean age (p = 0.31).
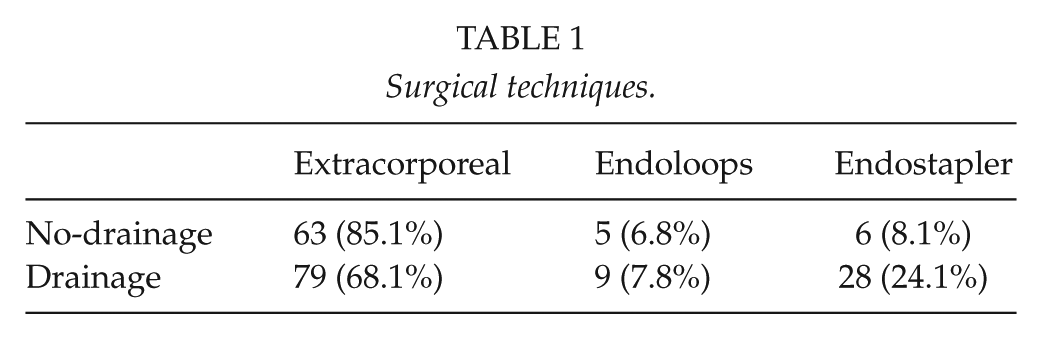
In the no-drainage group, there were 36 patients with an appendiceal phlegmon (48%), 56 patients with free purulent fluid (74.6%), and 44 patients with generalized peritonitis (58.6%). In the drainage group, the values were 72 (62%), 91 (77.7%), and 95 (81.9%), respectively. The rate of generalized peritonitis was the only parameter that was significantly different between the groups (p = 0.0004). No statistical differences were observed between the groups in the rate of appendiceal phlegmon (p = 0.055) and free purulent fluid (p = 0.61). In the no-drainage group, there were eight ruptures of the appendix (10.6%) and one appendiceal bleeding (1.3%), while in the drainage group the numbers were 13 (11.1%) and 2 (1.7%), respectively. No statistical differences were found between the groups in the rate of these intraoperative complications (p = 0.92 and p = 0.83, respectively). The rate of conversion was 2.6% in the no-drainage group and 1.7% in the drainage group (p = 0.65). The operative time was statistically significantly longer in the drainage group (p < 0.0001), with a median of 60.3 min in the no-drainage group and 79.3 min in the drainage group. The surgical techniques employed, when available, are shown in Table 1. There were statistically significant differences between both groups in extracorporeal technique (no-drainage group: 85.1% and drainage group: 68.1%; p = 0.015) and also in the use of endostaplers (no-drainage group: 8.1% and drainage group: 24.1%; p = 0.005).
Surgical techniques.
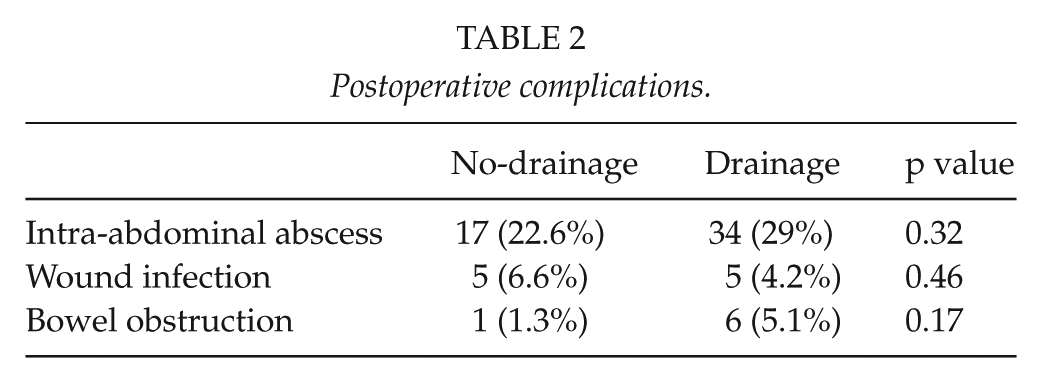
The antibiotic therapy was longer in the drainage group as compared to the no-drainage group, with a median of 7.51 and 6.61 days, respectively (p = 0.01). The analgesic medication use was also longer in the drainage group, with a median of 6.19 and 4.37 days (p < 0.0001). The mean postoperative onset of oral feeding was 3.32 days in the drainage group and 1.95 days in the no-drainage group (p < 0.0001). The length of postoperative hospital stay in the two groups was significantly different (p = 0.002), with a median of 11.55 and 9.2 days in patients with and without drainage, respectively. The postoperative complications are presented in Table 2. There were no statistically significant differences between the two groups in the rate of intra-abdominal abscess, wound infection, and bowel obstruction.
Postoperative complications.
Discussion
Throughout the history of surgery, controversy surrounds the use of abdominal drains after gastrointestinal surgery (1, 2). Theoretically, abdominal drains have the potential to evacuate intra-abdominal fluids and reduce surgical site infections. In addition, they may detect postoperative bleed or anastomotic leakage. However, abdominal drains may have a lot of complications. They may become blocked or kinked and, therefore, ineffective. Moreover, they would not be able to drain the whole peritoneal cavity because their tip is in a localized area. Additionally, abdominal drains expose the peritoneal cavity to the outside environment and may increase the risk of surgical site infection (2). The abdominal drain itself may impair the natural immune system of the peritoneal cavity to clear infections (4). Occasionally, serious complications of the abdominal drains have been reported in the literature such as small bowel evisceration or enteric fistula (5, 6).
Among pediatric patients with acute appendicitis, the rate of perforated appendicitis varies from 20% to 76%, which may lead to a significantly increased morbidity and postoperative complications (7, 8). This rate can reach 55%–80% of the appendicitis in patients younger than 6 years (3). In our series of 1736 pediatric patients, the rate of perforated appendicitis was 11.46%, which is lower than those reported in the literature. One of the reasons for this result may be the strict definition of perforated appendicitis in our study. There continues to be a debate about the practice and outcomes of perforated appendicitis. Recent studies have compared early versus delayed appendectomy in children (8–10). It appears that early appendectomy may improve outcomes in patients without an intra-abdominal abscess at the time of diagnosis (8). Additionally, these patients will have fewer radiological exams and healthcare visits (9). Complications such as intra-abdominal abscess or readmission prior to planned occurred in up to one-third of the cases of delayed appendectomy (10).
There are a few reports, which support the use of prophylactic abdominal drainage after appendectomy in the literature (11, 12). However, there are more studies published indicating that prophylactic drainage is not required after open or laparoscopic appendectomy in both adults and children (13–19). In fact, according to the level of evidence and grade of recommendation proposed by the Oxford Centre, there is evidence of level 1A that drains do not reduce complications after appendectomy for any stage of appendicitis (13) and recent guidelines supported that drains are not recommended in complicated appendicitis in pediatric patients (evidence of level 3B) (14).
It has been reported that the rate of intra-abdominal abscess after laparoscopic approach for perforated appendicitis may reach 32% (3). In our study, we had a similar rate of intra-abdominal abscess in patients with abdominal drainage (29%), while in the patients without drainage this rate decreases to 22.6% (p = 0.32). Several studies have shown an increased rate of intra-abdominal abscess and wound infection in the drainage group with statistically significant difference (15, 16). Our rate of wound infection was slightly higher in the no-drainage group than in the drainage group (6.6% versus 4.2%, respectively), but this difference was not statistically significant (p = 0.46). This could be because in the no-drainage group we performed more extracorporeal appendectomies and in these cases the appendix is usually extracted through the incision, whereas if we use an endostapler the appendix is usually extracted through the trocar.
The rate of bowel obstruction was higher in the drainage group than in the no-drainage group in our study as well as others (16, 17). Several authors have demonstrated that it is more likely that the cases of generalized peritonitis have an increased rate of bowel obstruction (11). In our series, the rate of generalized peritonitis is statistically higher in the drainage group than in the no-drainage group (81.9% versus 58.6%, p = 0.0004). However, some publications defend that drains may act as a foreign body and generate obstruction (2, 17).
Abdominal drainage has been statistically associated with an increased requirement of intravenous antibiotics (15, 16), late onset of oral feeding (15), longer operative time (17), and increased length of hospital stay (15–19). We have also found statistically significant differences between the two groups in these parameters, and in addition there was a statistically higher use of analgesic medication in the drainage group in our study (6.19 versus 4.37 days, p < 0.0001). Based on these observations, we agree with other authors that prophylactic abdominal drains are not necessary in children with perforated appendicitis (13–19).
Conclusion
In conclusion, the prophylactic use of abdominal drainage after laparoscopic appendectomy for perforated appendicitis in children does not prevent postoperative complications and may increase the use of analgesic and antibiotic medication, the fasting time, and the length of hospital stay. This combination of factors seems to tilt the risk–benefit balance in favor of abandoning prophylactic abdominal drains. However, prospective randomized studies will be necessary to verify this question.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.