
Abstract
Background:
Blunt pharyngoesophageal injuries pose a management challenge to the trauma surgeon. The purpose of this study was to explore whether these injuries can be managed expectantly without neck exploration.
Methods:
The National Trauma Databank datasets 2007–2011 were reviewed for blunt trauma patients who sustained a pharyngeal injury, including an injury to the cervical esophagus. Patients who survived over 24 h and were not transferred from other institutions were divided into two groups based on whether a neck exploration was performed. Outcomes included mortality and hospital stay.
Results:
A total of 545 (0.02%) patients were identified. The median age was 18 years and 69% were male. Facial fractures were found in 16%, while 13% had an associated traumatic brain injury. Of the 284 patients who survived over 24 h and were not transferred from another institution, 65 (23%) underwent a neck exploration. The injury burden was significantly higher in this group as indicated by the higher median Injury Severity Score (17 vs 10, p < 0.01) and need for intensive care unit admission (75% vs 31%, p < 0.01). The overall mortality was 2%: 3.1% for neck explorations versus 1.6% for conservative management (adjusted p = 0.54). Neck exploration patients were more likely to remain longer in the hospital (median 13 vs 10 days, adjusted p = 0.03).
Conclusion:
Pharyngoesophageal injuries are rare following blunt trauma. Only a quarter require a neck exploration and this decision appears to be dictated by the injury burden. Selective non-operative management based on clinical status seems to be feasible and is not associated with increased mortality.
Keywords
Background
Injuries to the pharyngoesophagus following blunt trauma are extremely rare and constitute a dilemma to the trauma surgeon due to the paucity of available recommendations regarding their management. While surgical repair and drainage was recommended as the therapeutic option of choice (1), over the past several years reports on selective non-operative approach with antibiotics, nasogastric tube, and withholding oral intake have emerged (2–4). This approach has been associated with clinical success in the majority of patients, avoiding the burden of surgery with its associated complications and impact on the patient’s life. Despite these emerging reports, currently there is no consensus regarding the management of pharyngoesophageal injuries and most recommendations originate from studies reviewing penetrating trauma (5–7).
The purpose of this investigation was to review the incidence of pharyngoesophageal injuries in blunt trauma patients. In addition, we sought to document the current state in the management of these injuries by trauma surgeons across the Unites States and report on their outcomes, based on whether a surgical procedure was pursued or not. We hypothesized that selective non-operative management of pharyngoesophageal injuries would result in similar outcomes as the operative approach.
Methods
The National Trauma Databank research datasets 2007–2011 were combined and queried for patients who had a blunt mechanism of trauma and a reported pharyngeal injury, including injury to the cervical esophagus (International Classification of Diseases, 9th Edition (ICD-9) codes: 874.4 and 874.5). Demographics and injury characteristics were abstracted and included age, gender, Injury Severity Score (ISS), Abbreviated Injury Scale (AIS) for all body regions, admission systolic blood pressure (SBP), admission Glasgow Coma Scale (GCS), and emergency department (ED)-assisted ventilation. Additional variables included specific mechanism of injury based on E-code, intention of injury, interfacility transfer, American College of Surgeons (ACS)-level trauma center, and concomitant injuries based on ICD-9 codes. Finally, all procedures for patients who met the inclusion criteria were reviewed and categorized based on body region, type, and timing. Appendix 1 lists all the categories of surgical and non-surgical interventions relevant to the neck, including diagnostic and surgical procedures to the pharynx, esophagus, larynx/trachea, and neck vessels.
A patient was considered to have a neck exploration if any surgical procedure was performed on the pharynx, esophagus, larynx, trachea, thyroid or parathyroid, and/or any neck vessel. Early neck exploration was defined as an exploration performed within 24 h from admission, while delayed neck explorations were those performed in a delayed fashion, after 24 h from admission. All definitions can be found in Appendix 2.
Patients who survived at least 24 h and were not transferred from another facility were then selected and divided into two groups: those who had a neck exploration and those who did not. The two groups were compared using standard statistical tools, including a chi-square or Fisher’s exact test for categorical variables and t-test or Mann–Whitney for continuous variables. The primary outcome was mortality and secondary outcomes included hospital and intensive care unit (ICU) length of stay, ventilation days, ICU-free days, and ventilation-free days. In order to adjust for confounding factors, a multivariate logistic regression model was utilized incorporating all covariates that were different between the two groups at a p level of <0.05.
The IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY) was the software utilized for the purposes of the analysis. Institutional Review Board approval was not required for this study as it involved “the collection or study of existing data, documents, records that are publicly available with the information recorded in such a manner that subjects cannot be identified, directly or through identifiers linked to the subjects.”
Results
A total of 3,313,117 records were reviewed and of them, 545 met the inclusion criteria of a pharyngeal injury due to a blunt mechanism of trauma, translating into an incidence of 0.02% for all blunt traumatic injuries and 4.7% for any blunt trauma involving the neck, defined as AIS neck ≥1 (Fig. 1). The median age was 18 years and 69.4% were male, with a median ISS of 12.7 (Table 1). The most common mechanism of injury was fall (36.0%), followed by motor vehicle crash (23.3%) and blunt assault (9.5%; Fig. 2).
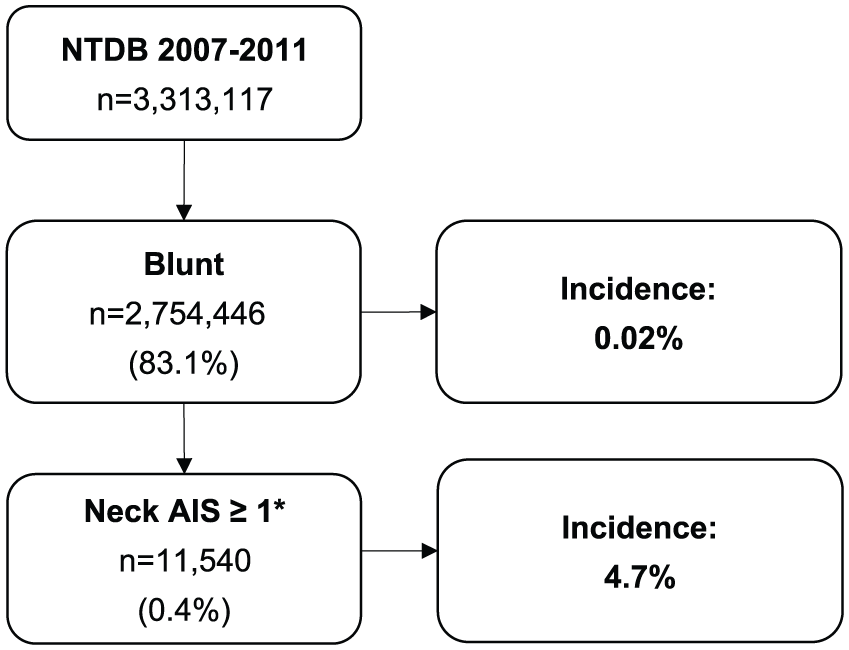
Study outline and incidence of pharyngeal injuries in patients with any neck trauma (defined as AIS neck ≥1).
Demographics, injury characteristics, and gross outcomes of patients with blunt pharyngeal injuries.
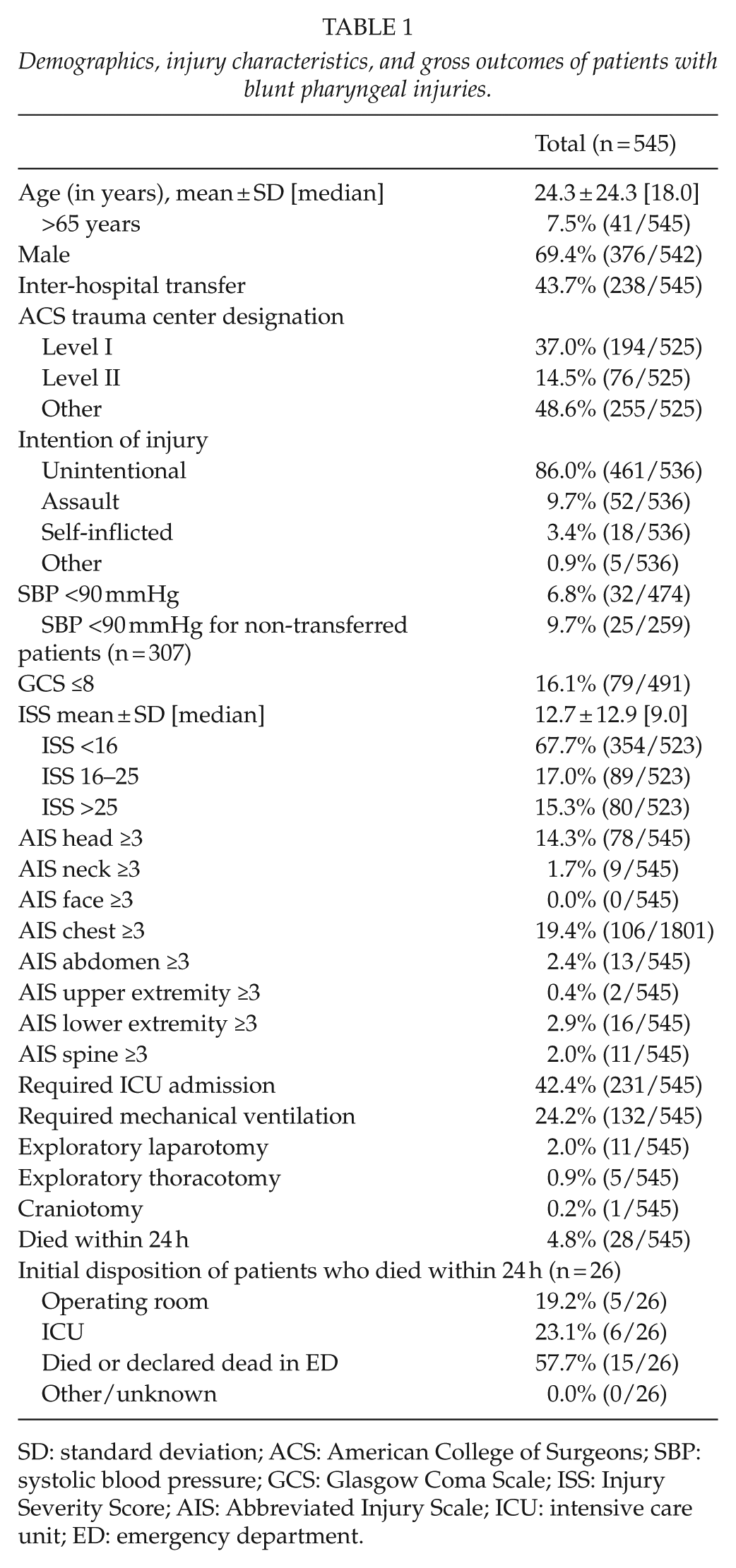
SD: standard deviation; ACS: American College of Surgeons; SBP: systolic blood pressure; GCS: Glasgow Coma Scale; ISS: Injury Severity Score; AIS: Abbreviated Injury Scale; ICU: intensive care unit; ED: emergency department.
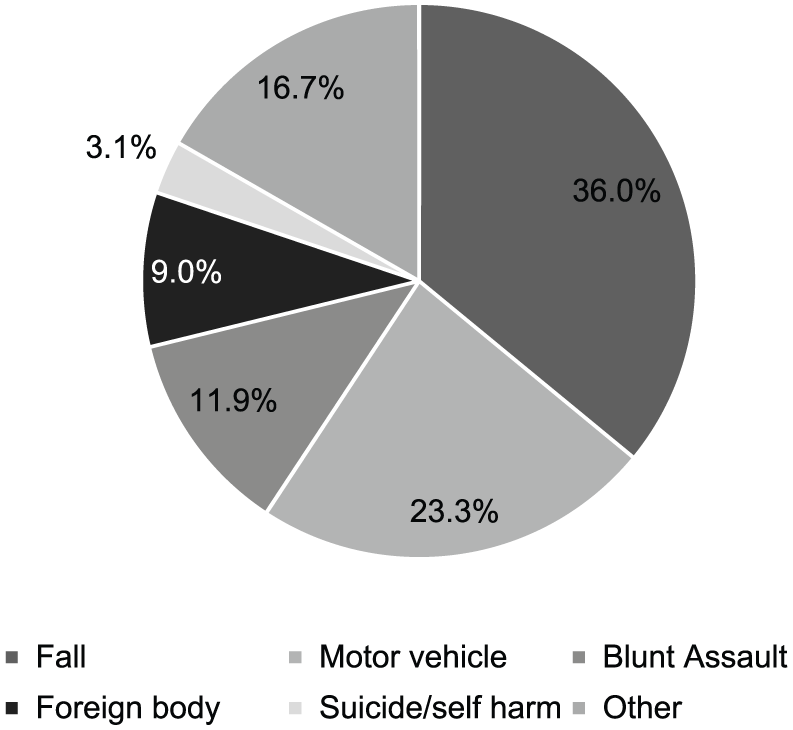
Mechanism of injury.
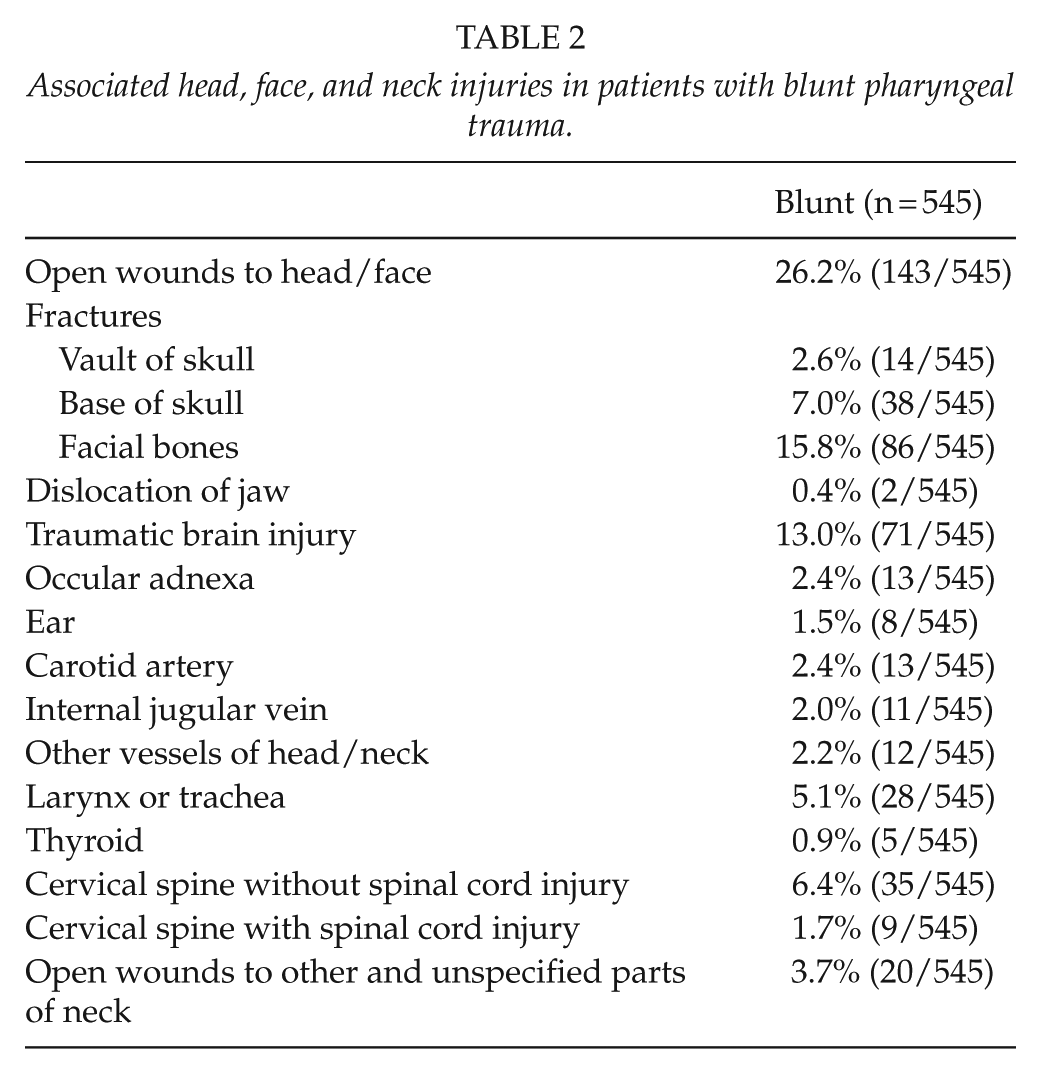
Hypotension, defined as SBP <90 mmHg on admission, was present in 6.9% of patients, while 16.1% had a GCS ≤8 and 11.7% required assisted ventilation in the ED (Table 1). The majority of patients (67.7%) had an ISS <16, however, 42.4% required admission to the ICU and 24.2% required mechanical ventilation more than 24 h. Associated injuries included severe head (defined as AIS head ≥3) in 14.3% and severe chest trauma (defined as AIS chest ≥3) in 19.4%. When examining associated injuries to the face, neck, and head, facial fractures were common and were found in 15.8% of patients (Table 2). Other injuries included traumatic brain injury in 13.0% and injury to the cervical spine, with (1.7%) or without (6.4%) spinal cord injury (Table 2).
Associated head, face, and neck injuries in patients with blunt pharyngeal trauma.
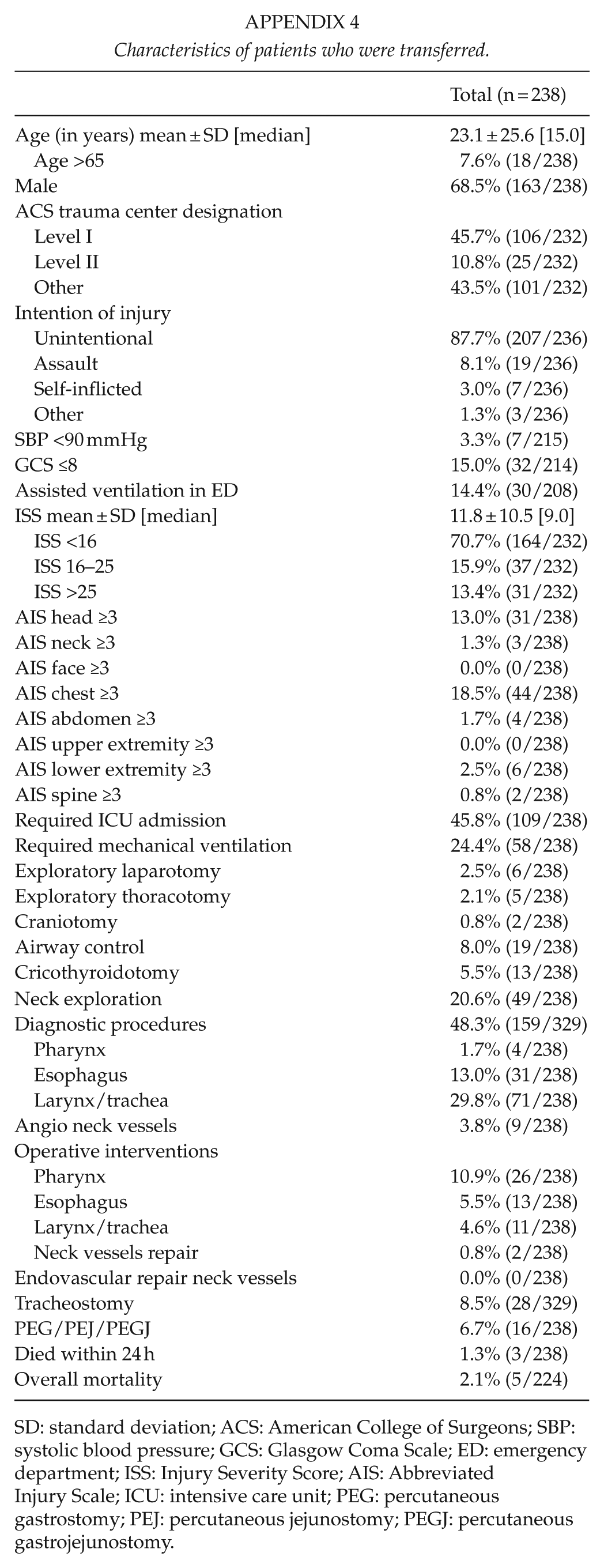
After excluding patients who died within 24 h from admission (4.8%) and/or those who were transferred from other facilities (43.7%), a total of 284 patients (52.1%) were left for analysis. Appendices 3 and 4 outline the characteristics of the excluded patients. Of note, 11.5% of those who died within 24 h and 20.6% of those who were transferred from other facilities underwent a neck exploration.
Patients were then divided into two groups based on whether they underwent neck exploration (22.9%) or not (77.1%). Those who did were significantly more likely to be older (median age 35 vs 15 years, p < 0.001) and to be admitted with a self-inflicted injury (8.1% vs 1.4%, p < 0.038). The injury burden was significantly higher for patients who underwent a neck exploration as indicated by a higher median ISS (17.1 vs 9.7, p < 0.001), a higher rate of severe chest trauma defined as AIS chest ≥ 3 (35.4% vs 11.9%, p < 0.001), and the need for ICU admission (75.4% vs 31.1%, p < 0.001) and mechanical ventilation (55.4% vs 14.2%, p < 0.001; Table 3).
Comparison of patients who received a neck exploration with those who did not (patients who died within 24 h from admission and those who were transferred were excluded from this analysis).
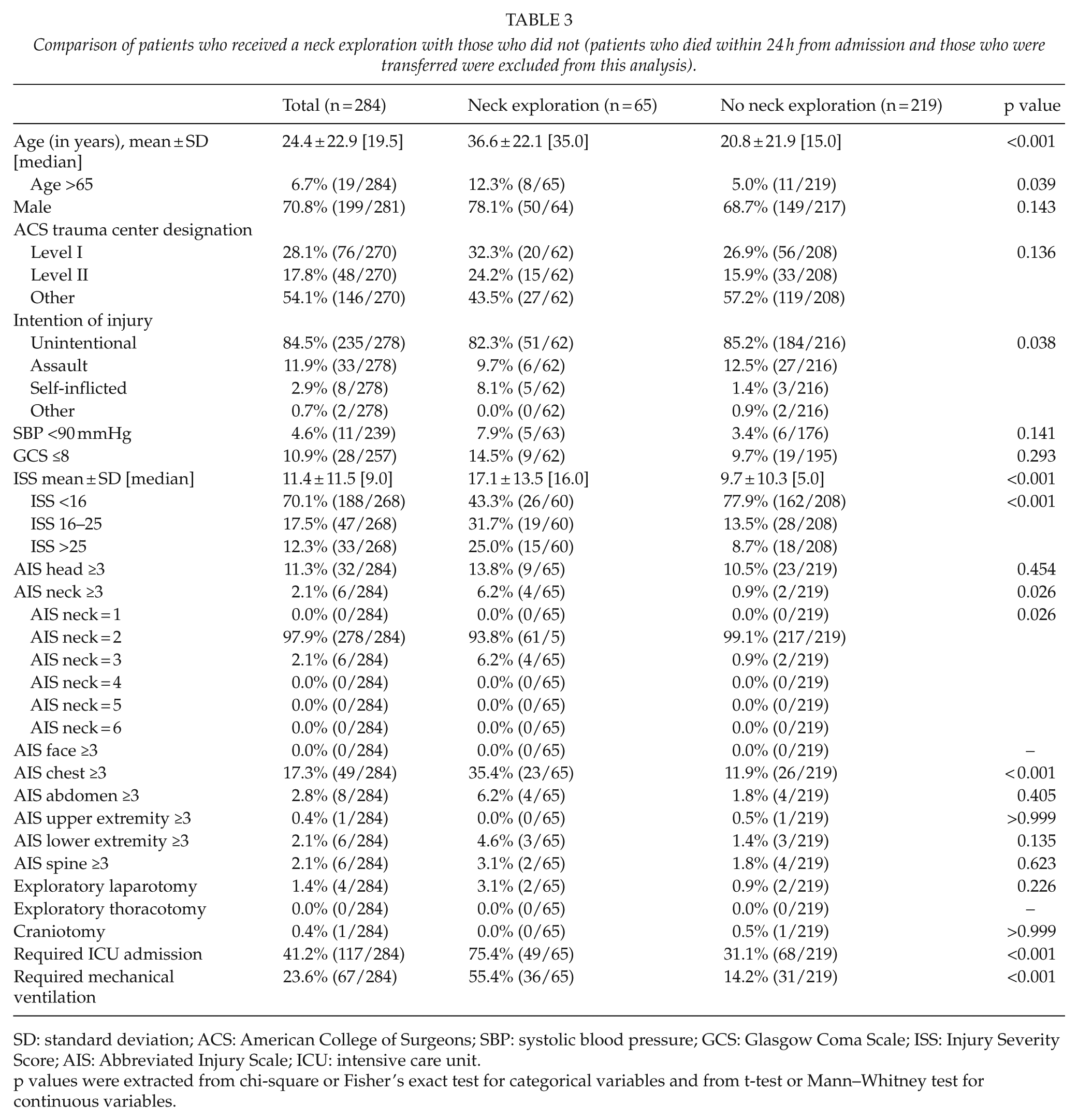
SD: standard deviation; ACS: American College of Surgeons; SBP: systolic blood pressure; GCS: Glasgow Coma Scale; ISS: Injury Severity Score; AIS: Abbreviated Injury Scale; ICU: intensive care unit.
p values were extracted from chi-square or Fisher’s exact test for categorical variables and from t-test or Mann–Whitney test for continuous variables.
The majority of patients who underwent a neck exploration did so within the first 24 h from admission (75.4%). In reviewing relevant neck procedures, 16.4% of patients who did not have a neck exploration underwent a diagnostic pharyngeal, esophageal, and/or laryngeal/tracheal procedure within the first 24 h and 4.1% underwent these procedures thereafter (Table 4). In addition, tracheostomy was required in only 4.1% of cases and a percutaneous gastrostomy/jejunostomy/gastrojejunostomy (PEG/PEJ/PEGJ) in 2.7%. Early neck explorations required repair of the pharynx in 69.4%, while with delayed exploration this was required in 43.8% . Tracheostomy was required in 8.2% of early and 25.0% of delayed exploration, while PEG/PEJ/PEGJ was required by 26.5% and 12.5%, respectively (Table 4).
Relevant procedures performed in patients who underwent early (within 24 h from admission), delayed (after 24 h from admission), and no neck exploration (patients who died within 24 h and those who were transferred were excluded from this analysis).
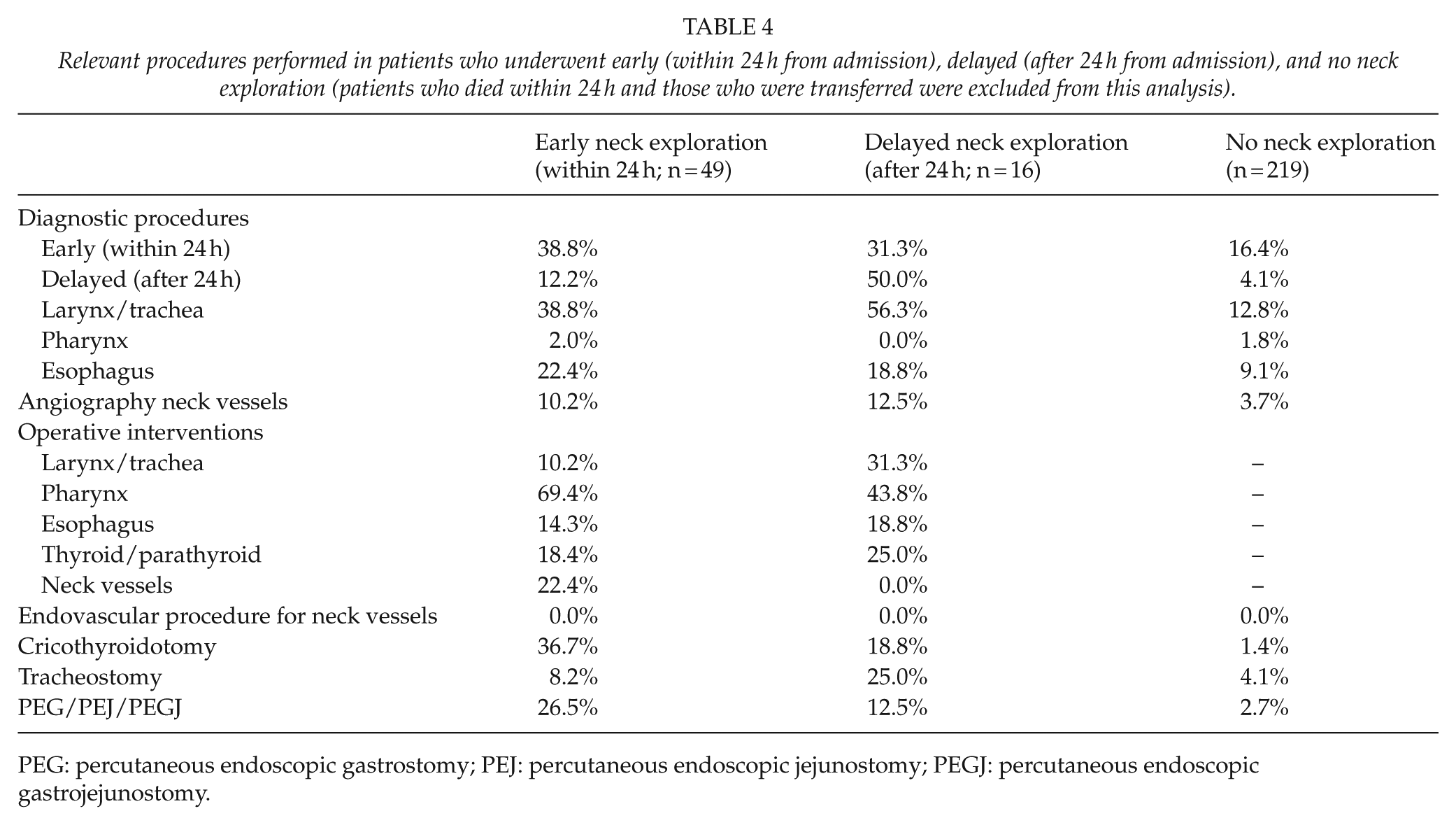
PEG: percutaneous endoscopic gastrostomy; PEJ: percutaneous endoscopic jejunostomy; PEGJ: percutaneous endoscopic gastrojejunostomy.
The overall mortality was 2.0%; 3.1% in patients who had a neck exploration and 1.6% in those who did not (Table 5). After adjusting for age, intention of injury, ISS, ICU admission, and need for mechanical ventilation, there was no statistically significant difference between the two groups in regard to mortality (adjusted odds ratio (AOR): 0.54; 95% confidence interval (CI): 0.07, 4.07); adjusted p value: 0.536). Although there was no difference in ICU or ventilation days, patients who underwent neck exploration had a longer overall hospital stay (adjusted mean difference (AMD): 2.99 days; 95% CI: 1.00, 4.99; adjusted p value: 0.003; Table 5).
Comparison of outcomes between patients who underwent neck exploration and those who did not (patients who died within 24 h and those who were transferred were excluded from this analysis).
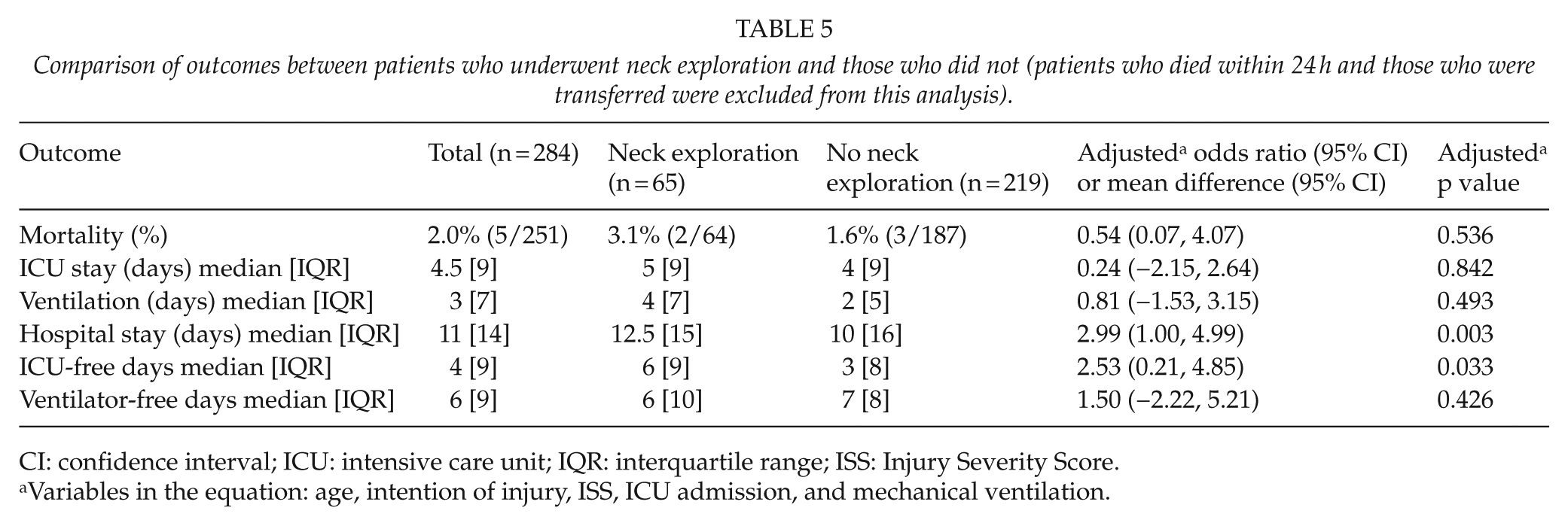
CI: confidence interval; ICU: intensive care unit; IQR: interquartile range; ISS: Injury Severity Score.
Variables in the equation: age, intention of injury, ISS, ICU admission, and mechanical ventilation.
Discussion
This study comprises the largest series to date examining pharyngoesophageal injuries resulting from a blunt force and reflects the current management of these patients by trauma surgeons in the United States. Our results indicate that only 2 out of every 10,000 victims of blunt trauma encountered a pharyngoesophageal injury. The majority of these patients presented to trauma centers with normal hemodynamics. Associated severe head (14.3%) and facial fractures (15.4%) were common with severe chest trauma present in almost one out of five (19.4%). More than three out of four of these patients did not undergo neck exploration (77.1%) and were managed expectantly. Those who required neck exploration were significantly younger, had a significantly higher injury burden, and required more frequent admission to the ICU (75.4%), in addition to mechanical ventilation (55.4%). Conservative management of these injuries was not associated with a higher mortality risk or prolonged hospital stay, indicating the feasibility of selective non-operative management without adversely affecting outcomes.
Data regarding blunt pharyngoesophageal injuries are scarce and typically available only in case reports and small case series, such that their true incidence is largely unknown. The incidence of esophageal injuries in blunt trauma patients was reported at 0.08% by Demetriades et al. (8), while in a review of over 4400 children, only 9 had a blunt injury to the cervical region with no pharyngeal and a single esophageal injury encountered (9). Although the National Trauma Databank (NTDB) does not contain a nationwide representative sample of trauma patients, the study period of 5 years encompasses over 3.3 million records from over 800 trauma centers. Therefore, our reported incidence of 0.02% for blunt trauma patients and 4.7% for patients with a blunt injury to the neck is likely representative of the true incidence.
Most pharyngeal injuries are known to be iatrogenic occurring during instrumentation of the pharyngoesophagus or during cervical discectomy and/or fusion (10). The presence of foreign bodies in this region is another described mechanism (11). In blunt trauma patients, the mechanism of injury varies in the literature and includes motor vehicle or motorcycle collision, fall, or direct impact during sports activities (2–4, 12, 13). In our series, the most common mechanism for pharyngoesophageal injury was fall, followed by motor vehicle crash. Blunt assault was reported in 11.9% of cases and these included strangulation. The mechanism of injury by itself may not aid the trauma surgeon in ruling out a pharyngoesophageal injury; however, clinical signs and the presence of associated injuries such as facial fractures, cervical spine fractures, traumatic brain injuries, and open wounds in the cervical region should raise the index of suspicion and prompt further investigation.
The absence of management guidelines for pharyngoesophageal injuries is due to the paucity of available literature, particularly in regard to operative intervention. Most recommendations originate from studies on penetrating neck trauma (6–8, 14–16). In a review of eight studies with 179 patients that included penetrating, blunt, and iatrogenic injuries, 105 underwent surgical management and the remaining 74 were observed. Treatment failures were reported in 13% and 12% of cases, respectively (10). Based on these findings, Zenga et al. (10) recommended conservative management with antibiotics for all patients who remain nil per os (NPO) in the interval between their injury and their presentation to the hospital and who do not show any signs of systemic infection. For the remaining patients, surgical exploration and repair was encouraged. Stanley et al. (7) reviewed 70 patients with a penetrating trauma to the hypopharynx and cervical esophagus. In this series, none of the patients who had an injury above the level of the tips of the arytenoids developed any complication, independent of whether the injury was managed surgically or not. Demetriades et al. (8) cautioned against this generalization and recommended that only small injuries of the hypopharynx be managed conservatively.
For blunt traumatic injuries to the pharyngoesophagus, Niezgoda et al. reviewed 11 case reports published before 1990 and found that 5 were managed conservatively and 6 required surgical repair. Their recommendations were to repair any injury exceeding 2 cm in length and observe smaller injuries with antibiotics and NPO status. A number of case reports on non-operative management of these injuries refer to both adult (2–4) and pediatric patients (12, 17). In our series, we found that three out of four patients did not require surgical intervention by means of a neck exploration and those who did had a significantly higher injury burden. The decision for surgical management in these patients could be due to the severity of injury, the associated clinical signs, and the imaging or endoscopic findings. Unfortunately, our study design cannot determine the main factors leading to the decision for surgery, however, our findings highlight the feasibility of expectant management in the majority of these cases with no adverse effect on outcomes.
Despite being the largest study to date reviewing blunt pharyngoesophageal injuries, there are inherent limitations related to the retrospective design, the NTDB itself which does not contain a nationwide representative sample population, and the under-reporting of data elements in the dataset. Even with the rigorous review of surgical procedures, these might have been omitted or reported under different ICD-9 codes. Complications could not be reviewed and the hospital length of stay was used as a marker of complicated hospital course. Specific injury characteristics including level, length or diameter, imaging findings, and clinical signs of aerodigestive trauma could not be obtained. Finally, in analyzing the outcomes for these injuries, we excluded patients who died within 24 h from admission (4.9%) as they represent an outlier subset of this population as well as those transferred from other institutions as the interval from injury to transfer could vary significantly. In addition, transferred patients could have procedures performed prior to transfer that would not be available for review. Despite these limitations, the large sample size of this study provides insight into the current management of pharyngoesophageal injuries by trauma surgeons throughout the United States and provides a comprehensive overview of the incidence, demographics, and clinical outcomes.
In conclusion, pharyngoesophageal injuries are rare following blunt trauma. Only one out of four patients requires a neck exploration and this decision appears to be dictated by the injury burden. Selective non-operative management of these injuries based on clinical status seems to be feasible and does not affect mortality. A high index of suspicion should be maintained by the trauma surgeon to identify occult injuries in patients who present with direct impact on the neck region and associated facial, head, and cervical trauma.
Footnotes
Appendix
Characteristics of patients who were transferred.
| Total (n = 238) | |
|---|---|
| Age (in years) mean ± SD [median] | 23.1 ± 25.6 [15.0] |
| Age >65 | 7.6% (18/238) |
| Male | 68.5% (163/238) |
| ACS trauma center designation | |
| Level I | 45.7% (106/232) |
| Level II | 10.8% (25/232) |
| Other | 43.5% (101/232) |
| Intention of injury | |
| Unintentional | 87.7% (207/236) |
| Assault | 8.1% (19/236) |
| Self-inflicted | 3.0% (7/236) |
| Other | 1.3% (3/236) |
| SBP <90 mmHg | 3.3% (7/215) |
| GCS ≤8 | 15.0% (32/214) |
| Assisted ventilation in ED | 14.4% (30/208) |
| ISS mean ± SD [median] | 11.8 ± 10.5 [9.0] |
| ISS <16 | 70.7% (164/232) |
| ISS 16–25 | 15.9% (37/232) |
| ISS >25 | 13.4% (31/232) |
| AIS head ≥3 | 13.0% (31/238) |
| AIS neck ≥3 | 1.3% (3/238) |
| AIS face ≥3 | 0.0% (0/238) |
| AIS chest ≥3 | 18.5% (44/238) |
| AIS abdomen ≥3 | 1.7% (4/238) |
| AIS upper extremity ≥3 | 0.0% (0/238) |
| AIS lower extremity ≥3 | 2.5% (6/238) |
| AIS spine ≥3 | 0.8% (2/238) |
| Required ICU admission | 45.8% (109/238) |
| Required mechanical ventilation | 24.4% (58/238) |
| Exploratory laparotomy | 2.5% (6/238) |
| Exploratory thoracotomy | 2.1% (5/238) |
| Craniotomy | 0.8% (2/238) |
| Airway control | 8.0% (19/238) |
| Cricothyroidotomy | 5.5% (13/238) |
| Neck exploration | 20.6% (49/238) |
| Diagnostic procedures | 48.3% (159/329) |
| Pharynx | 1.7% (4/238) |
| Esophagus | 13.0% (31/238) |
| Larynx/trachea | 29.8% (71/238) |
| Angio neck vessels | 3.8% (9/238) |
| Operative interventions | |
| Pharynx | 10.9% (26/238) |
| Esophagus | 5.5% (13/238) |
| Larynx/trachea | 4.6% (11/238) |
| Neck vessels repair | 0.8% (2/238) |
| Endovascular repair neck vessels | 0.0% (0/238) |
| Tracheostomy | 8.5% (28/329) |
| PEG/PEJ/PEGJ | 6.7% (16/238) |
| Died within 24 h | 1.3% (3/238) |
| Overall mortality | 2.1% (5/224) |
SD: standard deviation; ACS: American College of Surgeons; SBP: systolic blood pressure; GCS: Glasgow Coma Scale; ED: emergency department; ISS: Injury Severity Score; AIS: Abbreviated Injury Scale; ICU: intensive care unit; PEG: percutaneous gastrostomy; PEJ: percutaneous jejunostomy; PEGJ: percutaneous gastrojejunostomy.
Acknowledgements
The study conception and design of this article was formulated by G.B. and P.N. Acquisition of data was done by G.B., D.S.-G., and A.A.S. Analysis and interpretation of data was carried out by G.B., P.N., and D.S.-G. The literature review was undertaken by G.B., P.N., and D.S.-G. Drafting of the article was done by G.B., P.N., and E.J.L. Critical revision was undertaken by P.N., A.N., S.E., D.R.M., and E.J.L.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.