
Abstract
Background:
Internal fixation of pediatric tibia shaft fractures has become increasingly popular despite the fact that non-operative treatment results in satisfactory outcome with few exceptions. Indications for surgery and benefits of internal fixation are however still debatable.
Materials and Methods:
All 296 less than 16-year-old patients treated for a tibia shaft fracture between 2010 and 2015 in two of the five university hospitals in Finland were included in the study. Patient data were analyzed in three treatment groups: cast immobilization in emergency department, manipulation under anesthesia, and operative treatment. Incidence of operative treatment of pediatric tibia shaft fractures was calculated in the cities of Helsinki and Kuopio.
Results:
A total of 143 (47.3%) children’s tibia shaft fractures were treated with casting in emergency department, 71 (22.3%) with manipulation under anesthesia, and 82 (30.4%) with surgery. Mean age of the patients in these treatment groups was 6.2, 8.7, and 12.7 years. Fibula was intact in 89%, 51%, and 27% of the patients, respectively. All 6 patients with multiple fractures and 16 of 18 patients with open fractures were treated operatively. In eight patients, primary non-operative treatment was converted to internal fixation. Operatively treated patients with isolated closed fractures were more likely to have a fibula fracture (46/66 vs 52/214, p < 0.001), be older in age (13.08 ± 2.4 vs 6.4 ± 3.7, p < 0.001), and have more primary angulation (6.9 ± 5.8 vs 0.48 ± 3.1, p < 0.001). Re-operations were done to eight and corrective osteotomy to two operatively treated children.
Conclusion:
Operative treatment of a pediatric tibia shaft fracture is currently nearly a rule in patients with open or multiple fractures. Surgical treatment of closed tibia shaft fractures is based on surgeon’s personal preference, type of fracture and age of the patient.
Keywords
Background
Tibia is the third most common fracture location in pediatric patients (<16 years) (1–3). Two-thirds of pediatric patients with a tibia shaft fracture have an intact fibula (1, 4). Complete fractures of both bones are usually caused by high-energy trauma, whereas isolated tibia fractures usually result from torsional forces (5, 6).
Children’s tibia fractures have a great healing capacity due to thick periosteum and good blood circulation. As a result, closed tibia fractures in the growing skeleton will heal rapidly (7, 8). Therefore, most tibia fractures in children can be treated non-operatively with cast immobilization (CI) (9).
Internal fixation has been traditionally considered appropriate in patients with open fractures and in polytrauma patients. Osteosynthesis has been performed with flexible intramedullary nails (FIN), rigid intramedullary nails (RIN), plates, screws, pins, or external fixators.
All closed pediatric tibia fractures were treated non-operatively in Helsinki during 1980s (10). Operative treatment, especially flexible intramedullary nailing, has hence gained popularity in treatment of children’s fractures, but there are no studies reporting the ratio of pediatric tibia fractures currently treated operatively (4, 11–14).
Aim of This Study
We wanted to analyze the current treatment methods of pediatric tibia shaft fractures in two of the five tertiary treatment institutions in our country.
Materials and Methods
All under 16-year-old children and adolescents treated for a tibia shaft fracture during a 6-year period between 2010 and 2015 in Children’s Hospital, Helsinki University Central Hospital (204 patients) and in Department of Pediatric Surgery, Kuopio University Hospital (92 patients) were included in this study. Patients with epiphyseal or metaphyseal fractures were excluded (Fig. 1). The number of patients who were residents of Helsinki or Kuopio was registered in order to estimate the incidence of operatively treated pediatric tibia shaft fractures in these two cities (non-operative treatment for pediatric tibia shaft fractures is also given in several private clinics in Finland). Incidence of tibia fractures was counted annually by dividing the number of fractures by the number of children (Statistic Finland®) in both cities, Helsinki and Kuopio. Fracture incidence during study period (2010–15) is expressed as the mean value of the 6 years.

Tibia and fibula shaft fracture. Fractures extending to metaphyses (red boxes) were excluded from the study.
Hospital records were retrospectively reviewed to register demographic data, injury mechanism, fracture type, other injuries, and type of treatment (casting in emergency department (ED), manipulation under anesthesia (MUA), FIN, RIN, external-, plate-, screw-, or pin fixation). Fracture alignment was re-assessed by the investigators in digital radiographs taken at admission, after reduction, and during follow-ups. Tibia fractures were classified according to AO-classification. Rotational alignment had been clinically assessed and recorded in degrees.
Compartment syndrome (CS) was diagnosed clinically in both institutions without pressure measurements. Primary treatment was deemed unsatisfactory if a redo procedure was performed under anesthesia. Full-thickness skin lacerations caused by casts were registered. Infections were recorded as superficial or deep. Malunion was determined using the criteria presented by Heinrich et al.(9) Delayed union was defined if fracture union exceeded 20 weeks, non-union if surgery was performed to get the fracture to heal. The number of clinical follow-up visits and radiographs per patient was calculated.
Analysis of all data was done in three categories based on patients’ primary treatment: (1) long-leg cast applied in ED, (2) MUA and CI in operative room (OR), and (3) surgical treatment in OR. Minimum follow-up time was 1 year.
Incidence is reported per 1000 children. Poisson distribution was used to calculate the 95% confidence intervals (CIs) for incidence figures reported. Results are presented as medians and means ± standard deviation (SD) for continuous non-skewed variables. The frequency distribution of the categorical variables is compared between the groups with the chi-square test. Statistically significant level is set as p < 0.05. Correlations between continuous parameters were assessed by using Pearson’s correlation analysis. Multinomial logistic regression analysis was performed to determine which parameter (age, fracture type, dislocation, or fibula fracture) was of greatest and independent significance for prediction of operative treatment. Statistical program SPSS 22 (IBM Corp. released 2009. IBM SPSS Statistics for Windows, version 13.0; IBM Corp., Armonk, NY) was used for analyzes. Helsinki University Hospital’s Review Board approved the study protocol.
Results
In total, 166 (81%) of the 204 patients treated in Helsinki University Children’s Hospital were citizens of Helsinki and 28 (30%) of the 92 patients treated in Kuopio University Hospital were citizens of Kuopio. Pediatric population varied between 81.453 and 88.407 in Helsinki and 15.380 and 18.150 in Kuopio during the study period 2010–2015. The incidence of tibia shaft fracture was thus at least 0.33/1000 (CI: 0.25–0.38) in Helsinki and 0.27/1000 (CI: 0.22–0.29) in Kuopio. There were no significant changes in fracture incidence during the study period. Etiology of fractures in both cities is presented in Fig. 2.
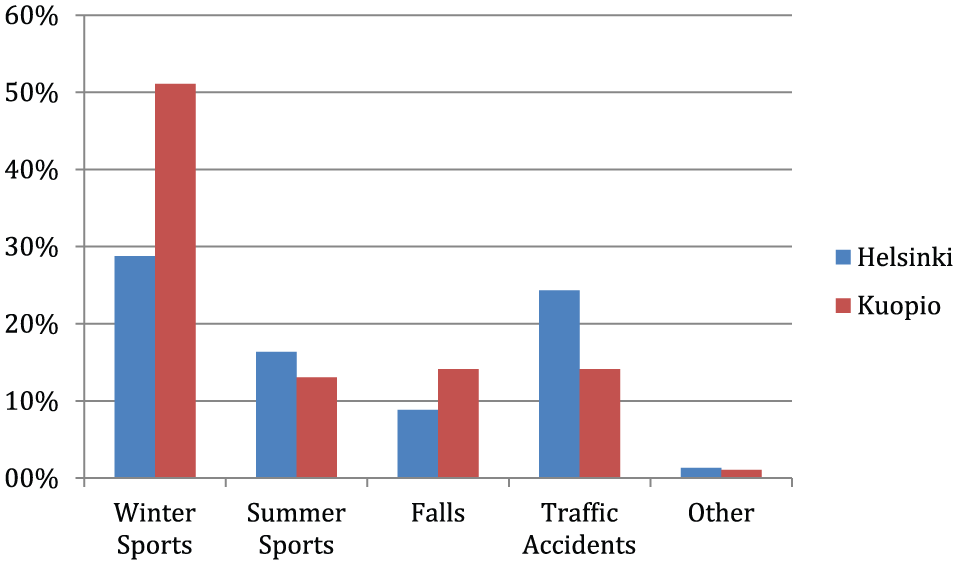
Ratio of different etiologies in pediatric tibia shaft fractures in Helsinki (n = 204) and in Kuopio (n = 92). Playground injuries are included in summer sports.
A total of 143 (48%) patients were treated in ED without anesthesia with a long-leg cast (Figs 3 and 4). Mean age of these patients was 6.2 years (±SD: 3.6 years, range: 1–14 years) of whom 127 (89%) had no fibula fracture (Table 1). Median primary angulation of their tibia fractures was 0° (range: 0°–5°). Seven patients with an intact fibula developed varus malalignment exceeding 5° during early follow-up, which was corrected in the outpatient clinic in four patients and by FIN in three patients. One patient sustained full-thickness skin laceration from inappropriate casting. All but one (12° external rotation malunion in 3-year-old boy) fractures healed in good alignment (Table 2).
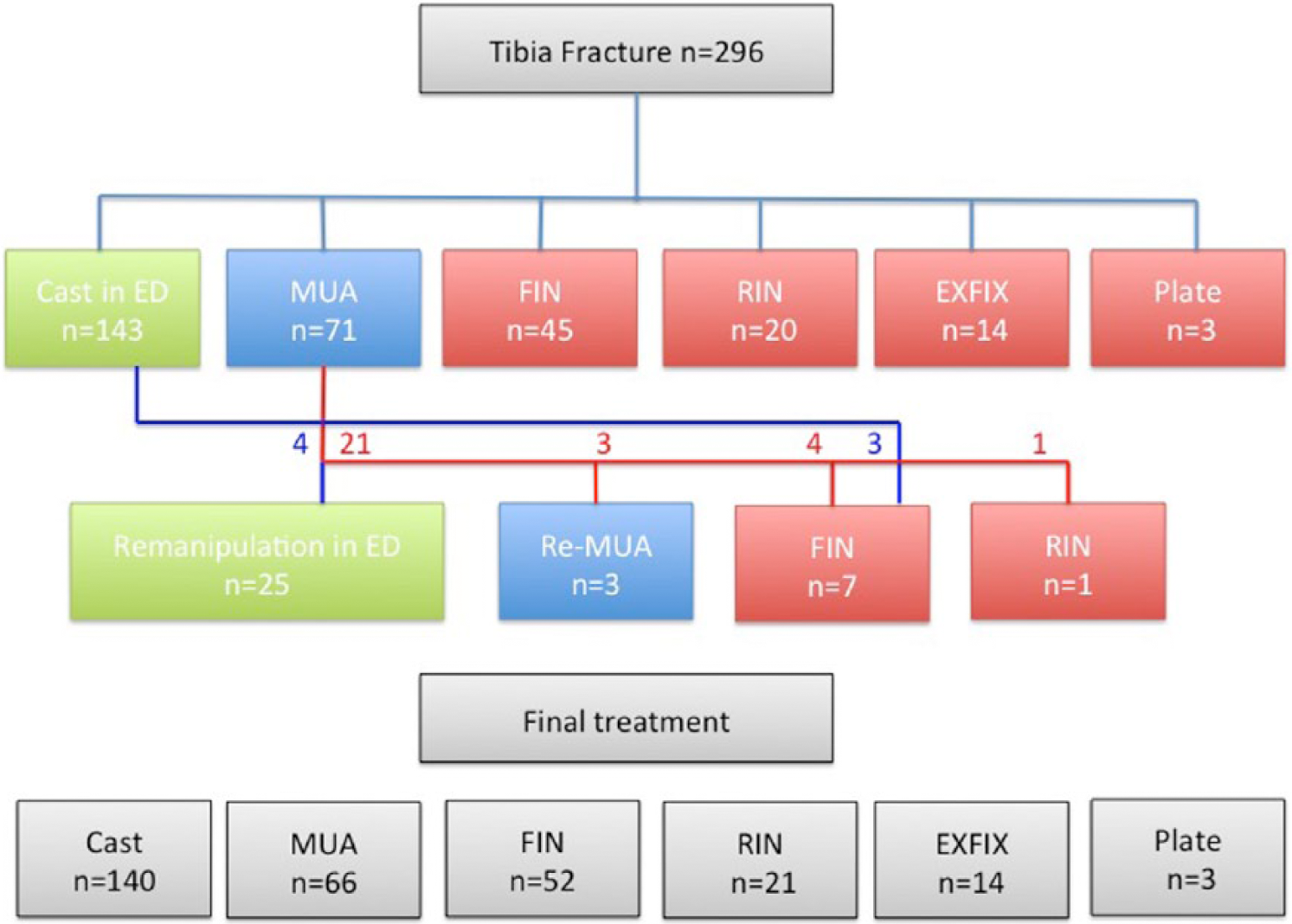
Treatment of 296 pediatric tibia shaft fractures in Helsinki and Kuopio during 2010 and 2015.
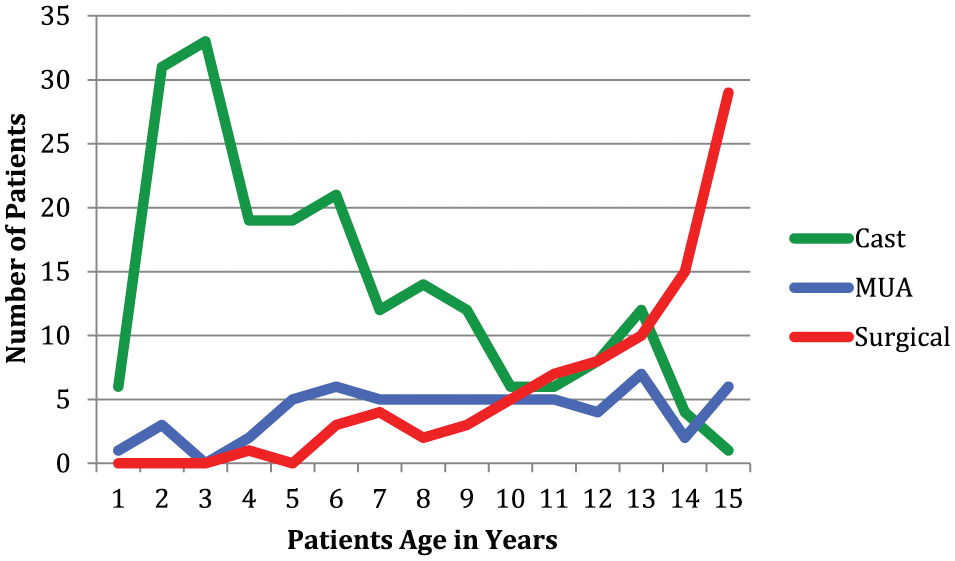
Treatment of pediatric tibia shaft fractures in Helsinki and in Kuopio in relation to the age of the patient.
Types of fractures in different treatment groups.
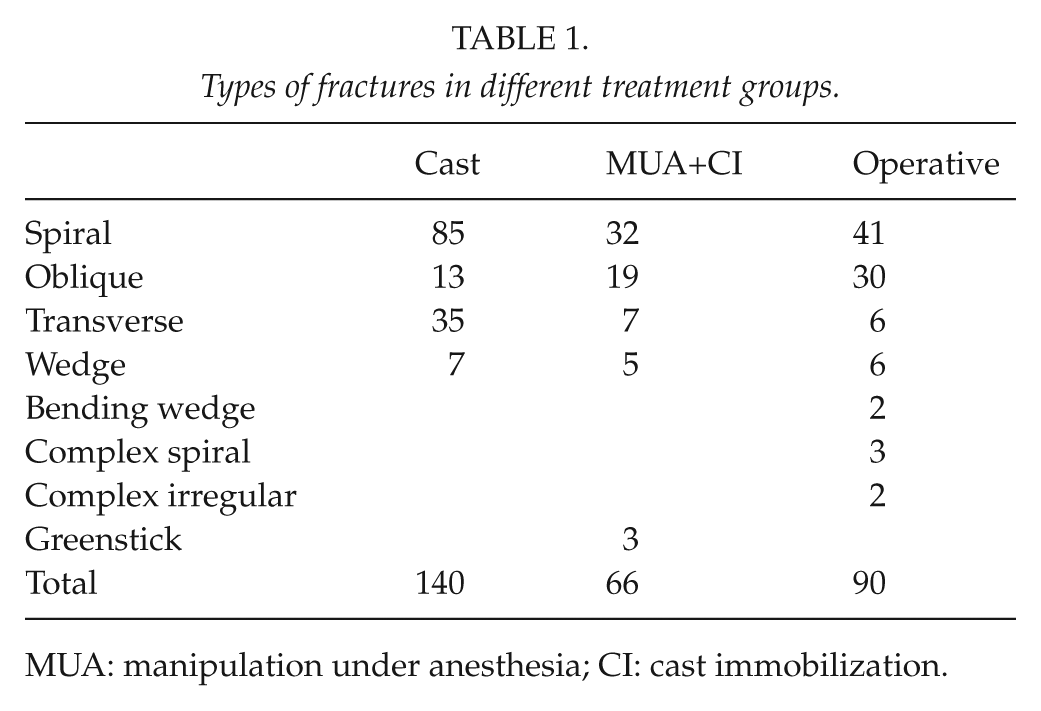
MUA: manipulation under anesthesia; CI: cast immobilization.
Comparison of treatment methods. Values are given as medians, range in parenthesis.
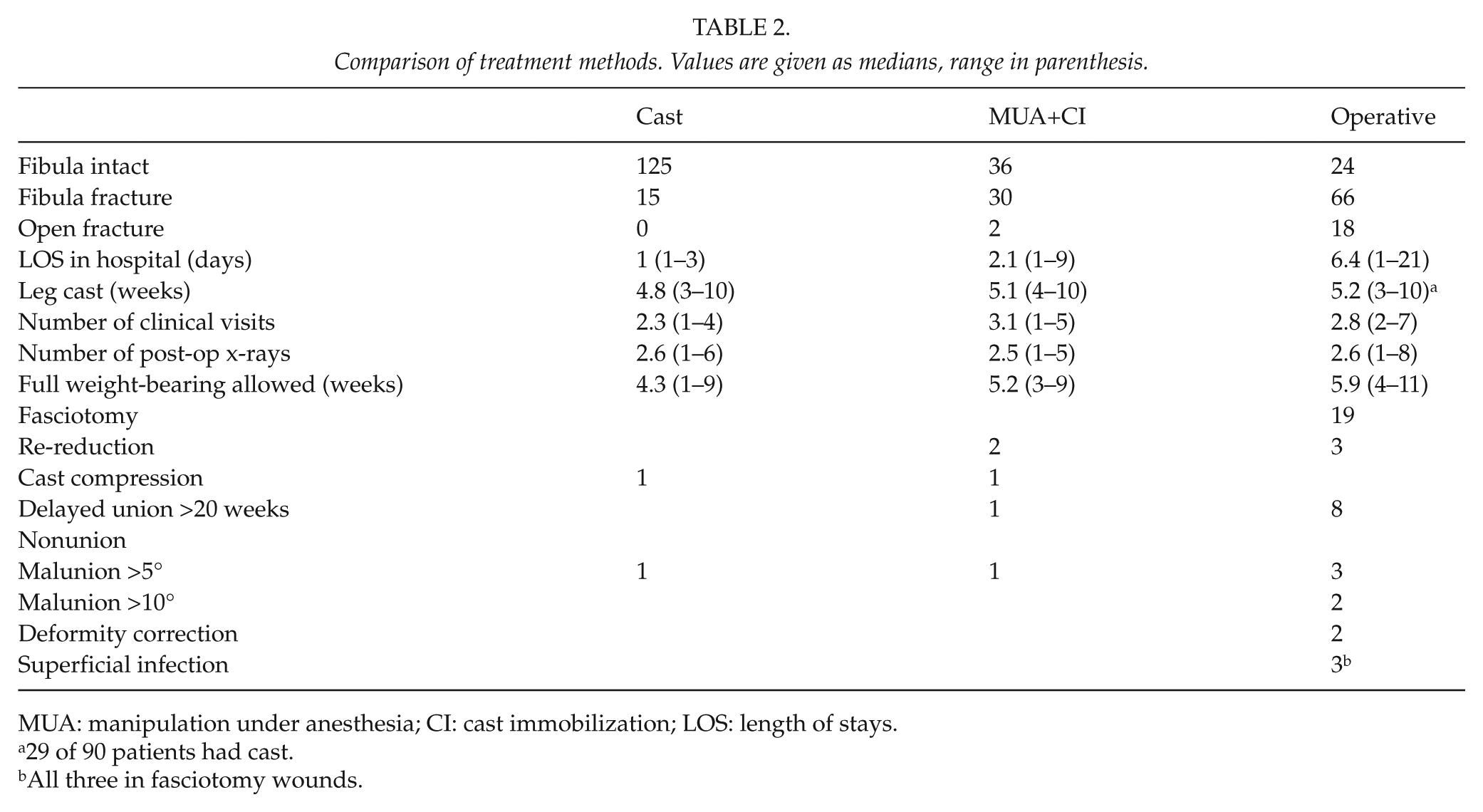
MUA: manipulation under anesthesia; CI: cast immobilization; LOS: length of stays.
29 of 90 patients had cast.
All three in fasciotomy wounds.
Overall, 71 (24%) patients were treated in OR with MUA+CI (Figs 3 and 4). Mean age of these patients was 8.7 years (±SD: 3.2 years, range: 2–15 years) and 36 of 71 of them had no fibula fracture. Two patients’ fractures were open (both Gustilo type I). One patient had bilateral fractures and another child had multiple fractures due to child abuse. Median angulation of their tibia fractures in primary radiographs was 3° (±SD: 4.6°, range: 0°–14°) and median displacement 3 mm (±SD: 3.3 mm, range: 0–17 mm). Two patients had a re-reduction of the fracture under anesthesia the following day after primary MUA due to unsatisfactory fracture alignment. Fracture alignment was partially lost in 29 of these 71 patients who developed 5°–12° angulation (varus or recurvatum) during the first 3 weeks of follow-up. Satisfactory alignment was retained in the outpatient clinic in 21 cases (re-manipulation: 11, wedging the cast: 10). Three patients required MUA. The remaining five patients were treated surgically (FIN: four, RIN: one). All fractures except one (6° varus malunion in a 11-year-old boy) healed in satisfactory alignment (Table 2).
Eighty-two (28%) fractures were primarily treated surgically (Figs 3 and 4). An additional eight patients were operated after initial non-operative treatment. Mean age of these 90 patients was 12.7 years (±SD: 2.8 years, range: 4–15 years). The majority (66) of these 90 patients had a concomitant fibula fracture. Median initial angulation was 6.7° (±SD: 6.3°, range: 0°–27°) and median initial displacement 7 mm (±SD: 5.7 mm, range: 0–28 mm). Eighteen fractures were open (grade I: seven, grade II: three, and grade III: eight), and three of these 18 patients had sustained polytrauma (injury severity score (ISS) >15). Thirteen of these tibia fractures were treated with internal fixation (FIN: seven and RIN: six) and five with external fixation. Six patients with 1–3 additional fractures were all treated operatively (FIN: four, RIN: one, and external fixation: one). Logistic regression analysis indicates that internal fixation of closed tibia fractures was also based on the age of the patient (older than 11 years) in addition to the presence of a concomitant fibula fracture.
Fasciotomy was done to 19 surgically treated patients (external fixation: eight, FIN: six, and RIN: five) of whom three developed superficial infections. Two of these 19 fasciotomies were performed after the primary procedure requiring an additional anesthesia (FIN: one and RIN: one). All but one of these patients had a concomitant fibula fracture and eight had an open fracture. Normalization of muscle color was registered intraoperatively in all 19 cases and no permanent injuries developed. One patient suffered peroneal palsy from an open fracture. A 15-year-old boy with previously undiagnosed hereditary S-protein deficiency developed deep vein thrombosis after RIN.
Three re-operations were performed in patients treated with FIN (unsatisfactory standard of primary surgery: two; nails bent from a new injury: one). In three patients, RIN was dynamized due to delayed union. Rotational deformity was corrected by osteotomy 13 months after the primary operation in two patients (primarily treated with RIN: one and external fixation: one).
Calculated incidence of operatively treated pediatric tibia shaft fracture was 0.06/1000 (CI: 0.03–0.07) in Helsinki and 0.03/1000 (CI: 0.01–0.06) in Kuopio. Operatively treated patients with isolated closed fractures were more likely to have a fibula fracture (46/66 vs 52/214, p < 0.0001), be older in age (13.08 ± 2.4 vs 6.4 ± 3.7, p < 0.0001), and have more primary angulation (6.9 ± 5.8 vs 0.48 ± 3.1, p < 0.001). Logistic regression analysis indicates that internal fixation of closed tibia fractures was also based on the age of the patient (older than 11 years) in addition to the presence of a concomitant fibula fracture. The rate of operative treatment in patients with closed tibia shaft fractures without other injuries was higher in Helsinki (66/177) than in Kuopio (10/86); p < 0.001. Statistically significant differences were not found between non-operatively and operatively treated children in fracture type, frequency of concomitant fibula fracture, or delay of treatment which did not thus explain the higher rate of complications associated with operative treatment.
Discussion
Current treatment methods and results of pediatric tibia shaft fractures were analyzed in two of the five tertiary pediatric trauma centers in Finland. These two centers differ in two aspects that can potentially affect fracture treatment: In Helsinki Children’s Hospital, which is the biggest pediatric hospital in our country, orthopedic surgeons are in-charge of all fracture treatments, whereas in Kuopio, pediatric surgeons treat most children’s fractures. Second, in Helsinki, pediatric tibia shaft fractures are more often caused by traffic accidents than in Kuopio where winter sports dominate as the cause of these injuries. Conclusions about the comparison should however be made with caution because of the retrospective nature of the study.
The reported incidence of tibia fractures in children is 1.0–1.06/1000 (10, 15–17) of which 19%–39% are located in the diaphysis 1 . According to previous studies, most tibia fractures in the pediatric population are caused by sporting or traffic accidents (4, 5, 10, 16, 18). Our findings are consistent with these previous studies since incidence of tibia shaft fractures was at least 0.33/1000 in Helsinki. Winter sports and traffic accidents were the two most common reasons for the fractures in our study. High number of skiing accidents in Kuopio can be explained by the geographical location of the city close to skiing resorts.
In the growing skeleton, periosteum is thick and strong, which decreases shortening and displacement of the fracture fragments and shortens healing time (5). Therefore, most diaphyseal fractures can be treated by reduction, if necessary, and CI (3, 10, 19, 20). Nevertheless, since 1990s, when practically all tibia shaft fractures in Helsinki were treated non-operatively (10), surgical treatment of pediatric tibia shaft fractures has become more common mainly for non-medical reasons, for example, activities in daily living are easier to handle without a long-leg cast (3, 21, 22). However, implant removal, if necessary, has to be done under another anesthesia (23–25). FIN is currently probably the most popular method of internal fixation in the Western world (3, 26, 27). Nearly one-third (30%) of all fractures in this study were treated operatively, 52 of 90 with FIN. There are no previous population-based reports of the incidence of operatively treated tibia shaft fractures, which was twice as high among citizens of Helsinki (0.07/1000) compared to children from Kuopio (0.03/1000) during the study period in 2010 and 2015.
Patients with open-, comminuted-, or instable fractures or with associated injuries can benefit from surgical treatment (3, 28). Furthermore, satisfactory alignment of tibia shaft fractures in some patients with an intact fibula can be difficult to control with a cast (5). In a recent study, Canavese et al.(14) found that the results of non-operative and operative treatment of diaphyseal fractures of tibia in patients with an intact fibula were essentially the same and considered both treatment methods satisfactory. In our study, all patients with polytrauma and with associated injuries, as well as all but 2 of the 20 patients with open tibia fractures, were treated surgically. The rate of operative treatment in patients with isolated closed tibia fractures was much higher in Helsinki (37%) than in Kuopio (12%). Internal fixation of an isolated closed tibia shaft fracture was more likely in older patients with an unstable tibia fracture and an ipsilateral fibula fracture. Mean time to full weight-bearing was longer in operatively treated patients, which can be at least partially explained by the operatively treated patients being older and having unstable fractures more often than patient treated non-operatively.
Reduced but instable tibia shaft fractures have a 28%–44% risk to develop malalignment during first weeks of CI (5, 10, 29). The results of this study are in accordance with these earlier findings. Primary satisfactory fracture alignment worsened in 5% of our patients treated in ED and 41% of patients who had MUA for primary treatment. Satisfactory fracture alignment was restored in outpatient clinic without anesthesia in most (25/36) of these patients. Re-MUA was done in two patients. Primary non-operative treatment was converted to internal fixation in 8 of 214 (5%) patients.
Complication rate in non-operatively treated tibia fractures in pediatric patients has been reported to vary between 1% and 26% and after operative treatment between 15% and 26% (5, 10, 11, 14, 26, 30). The 206 non-operatively treated patients in this study had no injury-related complications and 4 (2%) complications of treatment (cast compression sores: 2; clinically insignificant deformity: 2). However, 19 of 90 (21%) of the operatively treated patients had a CS and 4 of the 7 patients had clearly treatment-related complications (8%) which resulted in further surgery (redo FIN because of unsatisfactory standard of primary osteosynthesis: 2; rotation osteotomy: 2). The clearly lower rate of complications in non-operatively treated children in this study can be explained by a more benign fracture type compared to the patients treated surgically. It is thus unclear if the overall complication rate could have been decreased by treating all patients with closed fractures non-operatively. The current quality of non-operative treatment can be regarded satisfactory in both institutions, but the quality of both intramedullary nailing and external fixation should be better.
Conclusion
The majority of pediatric tibia shaft fractures are still treated non-surgically with few complications. Surgical treatment is preferred in patients with open or multiple fractures, but decision to internally fix an isolated closed tibia shaft fracture seem to be based on surgeon’s personal experience, stability of the fracture, and age of the patient. Quality of operative treatment should be improved to such a level that no re-operations or deformity corrections are necessary.
Footnotes
Acknowledgements
A.S. contributed to planning of the study design, data collection and analysis, and preparation of manuscript; T.L. contributed to planning of the study design and data collection; N.N. contributed to data collection and preparation of manuscript; J.J. contributed to data collection, statistical analysis, and planning of the study design; and Y.N. contributed to planning of the study design, and data and preparation of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.