
Abstract
Purpose:
Hemiarthroplasty is a common treatment for patient with a fragility displaced femoral neck fracture. We compared lateral and posterior approaches with respect to need for mobility aids, mobility level, living arrangements, pain, hip dislocation, and survival 12 months after hip fracture.
Methods:
A total of 393 fragility femoral neck fracture patients aged 65 years or more who underwent hemiarthroplasty were observed for 12 months. Patient information was collected on admission, during hospitalization, and by telephone interview 1 year after the hip fracture. A total of 269 patients were included in the final analysis.
Results:
At 1 year after hip fracture, more patients undergoing hemiarthroplasty with the posterior approach (22%) survived without mobility aids compared to those with the lateral approach (12%; p = 0.026). Multivariate logistic regression analysis revealed that the need for mobility aids 1 year after hip fracture was significantly predicted by the use of mobility aids before the fracture (odds ratio = 13.46, 95% confidence interval = 4.29–42.25), age ≥85 years (odds ratio = 3.85, 95% confidence interval = 1.09–13.44), male sex (odds ratio = 3.59, 95% confidence interval = 1.05–12.22), and lateral approach (odds ratio 2.73, 95% confidence interval 1.15–6.50). The posterior approach resulted in four (3.4%) dislocated hips, compared with none by the lateral approach. Survival, mobility level, pain in the operated hip, and living arrangements 1 year postoperatively were not significantly different between groups.
Conclusion:
Hemiarthroplasty using a lateral approach predisposed to the need for ambulatory aids 1 year after hip fracture. The posterior approach, however, predisposed to hip dislocation. Patient selection must be considered when deciding the appropriate surgical approach.
Introduction
Hemiarthroplasty (HA) is a common treatment choice for displaced fragility hip fractures. HA enables immediate full weight-bearing without the risk of typical complications related to internal fixation, including avascular necrosis and nonunion. Moreover, in patients older than 60 years, HA results in fewer reoperations compared with internal fixation (1, 2). Furthermore, total hip arthroplasty (THA) is considered a better option for previously independent and healthy patients due to the functional results, despite an increased incidence of hip dislocation (3, 4). The best approach for hip joint arthroplasty, however, remains controversial.
The anterior approach (Smith-Petersen) utilizes the tissue plane between the sartorius and tensor fasciae latae superficially and between the rectus femoris and gluteus medius (5). The anterolateral approach (Watson-Jones) utilizes the intermuscular plane between the tensor fasciae latae and gluteus medius (6). The lateral approach includes separating the gluteus medius and vastus lateralis insertions from the greater trochanteric insertions, which are attached after prosthesis implantation into their original position (7). All modifications of the lateral approach involve the division and later repair of the gluteus medius. The posterior approach includes separating the gluteus maximus muscle following the release of external rotators from the femoral insertion (8). Each approach has advantages and a different spectrum of complications. Previously conducted studies of hip fracture patients treated with HA indicate that the posterior approach increases the risk of hip dislocation and reoperation compared to the lateral approach (9–11).The lateral approach, however, may predispose to hematoma. Rates of infection, seroma, and perioperative fractures are similar after both approaches (11).
Most studies comparing the outcomes between hip arthroplasty approaches have mainly evaluated patients undergoing THA. The study results cannot be directly applied to fragility hip fracture patients, a moribund population with multiple comorbidities, frailty, and a higher risk of altered living arrangements and impaired mobility. Furthermore, most previous studies focused only on the dislocation rate, early complications, and reoperations. Measurements of other important outcomes, such as a change in the living arrangement, need for mobility aids, and mobility level, are crucial among fragility hip fracture patients. Avoiding mortality, immobility, and institutionalization represent essential goals in the comprehensive treatment of fragility hip fracture patients. This study compared HA using the lateral and posterior approaches among fragility hip fracture patients and evaluated the differences in living arrangements, need for mobility aids, mobility level, pain, and survival 1 year postoperatively.
Patients and Methods
This study comprised a prospectively and retrospectively documented cohort including 462 consecutive patients treated with a unipolar hip HA using a lateral or posterior approach in the Department of Trauma and Orthopaedic Surgery at the Seinäjoki Central Hospital between 1 September 2008 and 31 August 2012. The cohort represents a subpopulation of a prospectively collected comprehensive hip fracture database. For this study, only information on the implanted femoral stems (cemented or uncemented) and hip dislocations was collected retrospectively. All patients aged ≥65 years with a low-energy, non-pathological fragility cervical hip fracture treated with HA were included in the study and followed for 1 year postoperatively. Only the first hip fracture in each patient during the follow-up period was included. Exclusion criteria included immobility (mobile with wheelchair or bed bound) before hip fracture and moderate-to-high energy hip fractures; traffic-, bicycle- or pedestrian-accidents, and falling other than at the same level.
The referral area for hip fracture patients was South Ostrobothnia in Finland, which has a population of 193,977. Residents over 65 years of age represent 21% of the total population according to the Official Statistics of Finland, a statutory electronic population register of the country. All patients who sustain a hip fracture or surgical complication after treatment of a hip fracture inside the referral area are admitted and operated on at Seinäjoki Central Hospital. Data on deaths were obtained from the Official Cause of Death Statistics of Finland, which cover ~100% of deaths in Finland.
A flowchart of the patient population is shown in Fig. 1. A total of 269 patients were analyzed in this study, 151 underwent the lateral approach, and 118 underwent the posterior approach. There were no statistically significant differences between groups in age, sex, living with someone, need for mobility aids or extent of need before fracture, previous living arrangements, diagnosis of memory disorder, medications on admission, or American Society of Anesthesiologists (ASA) grade (Table 1).
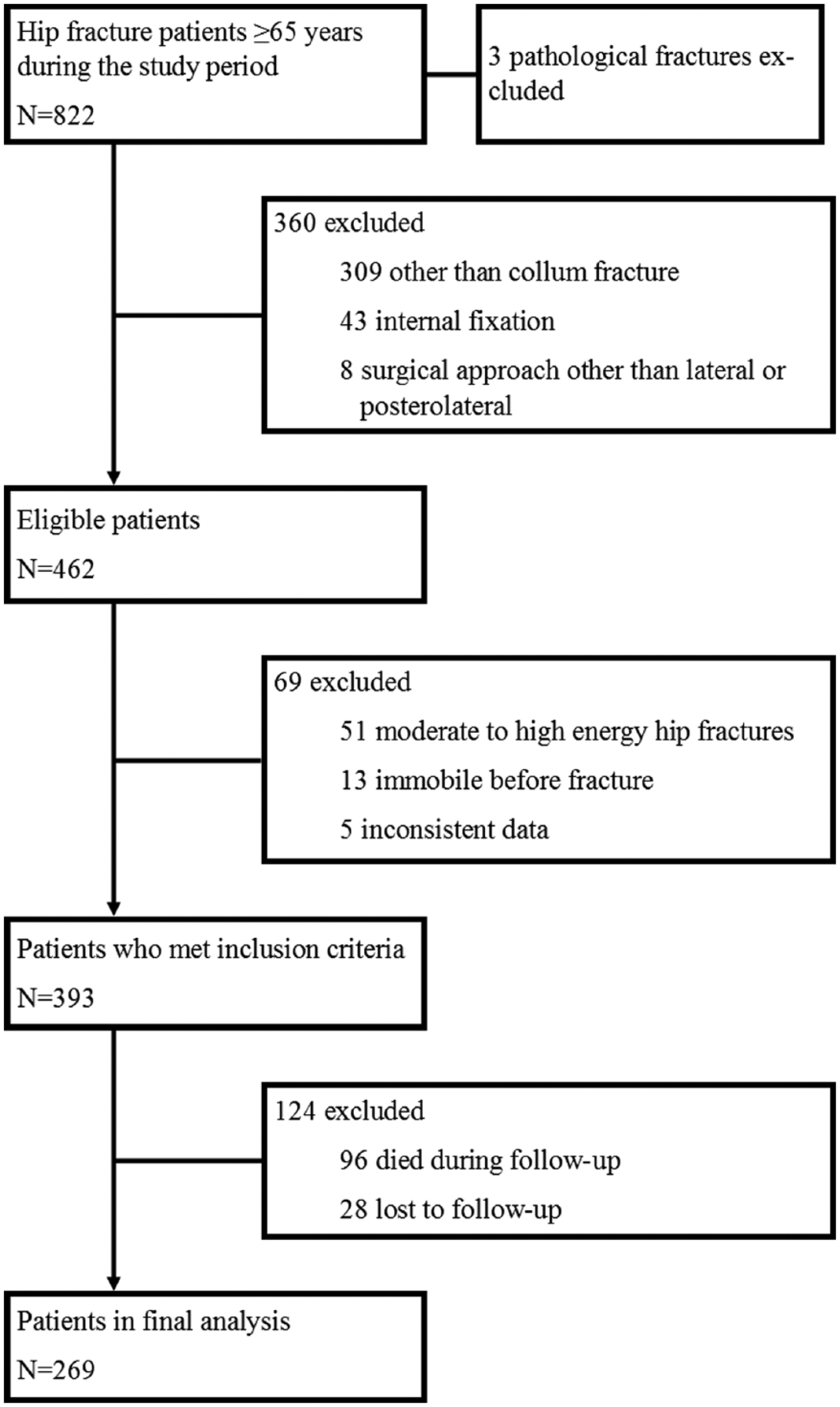
Study flowchart.
Patient characteristics for baseline population and survivors at the time of hip fracture.
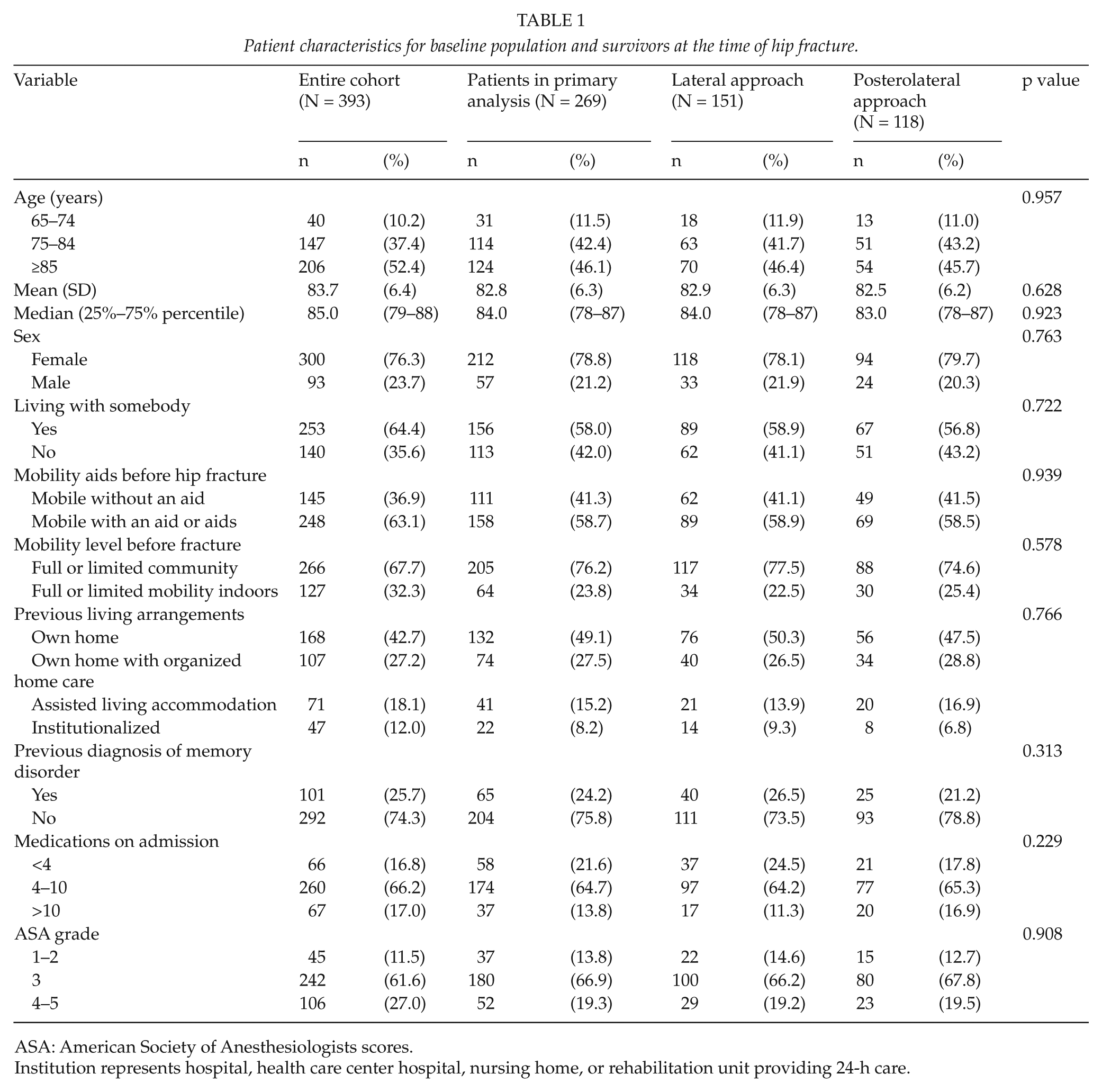
ASA: American Society of Anesthesiologists scores.
Institution represents hospital, health care center hospital, nursing home, or rehabilitation unit providing 24-h care.
The surgeon on duty selected whether to use a lateral (modified Hardinge) or posterior approach with repair of the posterior capsule and external rotators (7, 8). Regardless of the surgical approach selected, every patient was positioned laterally on the operating table. In the modified Hardinge approach, access to the hip joint was achieved through an abductor muscle split; the gluteus medius was split longitudinally at the junction of the anterior third to posterior two-thirds of the muscle width and the split was not extended more than 3 cm superior to the trochanter insertion. The split flap (gluteus medius and minimus and vastus lateralis) was repaired to the greater trochanter with a tendon-to-tendon or tendon-to-bone attachment. In the posterior approach, the hip joint was revealed by detaching the short external rotators from femur insertion with preservation of the piriformis tendon. The joint capsule was incised to expose the femoral neck fracture. After prosthesis implantation, detached posterior structures were fixed to the original position with bone sutures. Registrar surgeons were supervised by consulting orthopedic surgeons. All patients received a single shot of antibiotics as prophylaxis against infection unless ongoing antibiotics for other reasons were administered 1 h before operation. The orthopedic surgeon in charge decided whether to use an uncemented or cemented stem. Patients were mobilized allowing for full weight-bearing as soon as possible.
Patient characteristics were collected on admission, during hospitalization, and 12 months after hip fracture by phone interview. If a patient was unable to provide information due to health or cognitive problems, data were acquired from a proxy who knew the patient, such as family members, friends, and nurses from a health care institution. During the study period, predefined inquiries modified from British hip fracture register were used to obtain as accurate data as possible (12).
The need for ambulatory aids, mobility level, pain in operated hip, HA dislocation, and living arrangements were variables of interest 12 months after hip fracture. Mobility aids were registered in the database as follows: independent, cane, canes, folding walker or rollator, wheelchair, or immobile. The need for mobility aids was categorized into two groups: mobile without aids and mobile with aids or immobile, because groups of patients who needed a cane, canes, or were immobile were too small to be analyzed separately (Fig. 2A and B). Mobility level was classified as unassisted or assisted outdoors, unassisted or assisted indoors, and unable to move. Pain was handled as a dichotomous variable. Patients were categorized as ASA grade I to II and ASA grade IV to V, because ASA group I (n = 3) was too small to be analyzed separately and ASA groups IV and V were combined in the hip fracture database due to the small number of patients with ASA grade V.
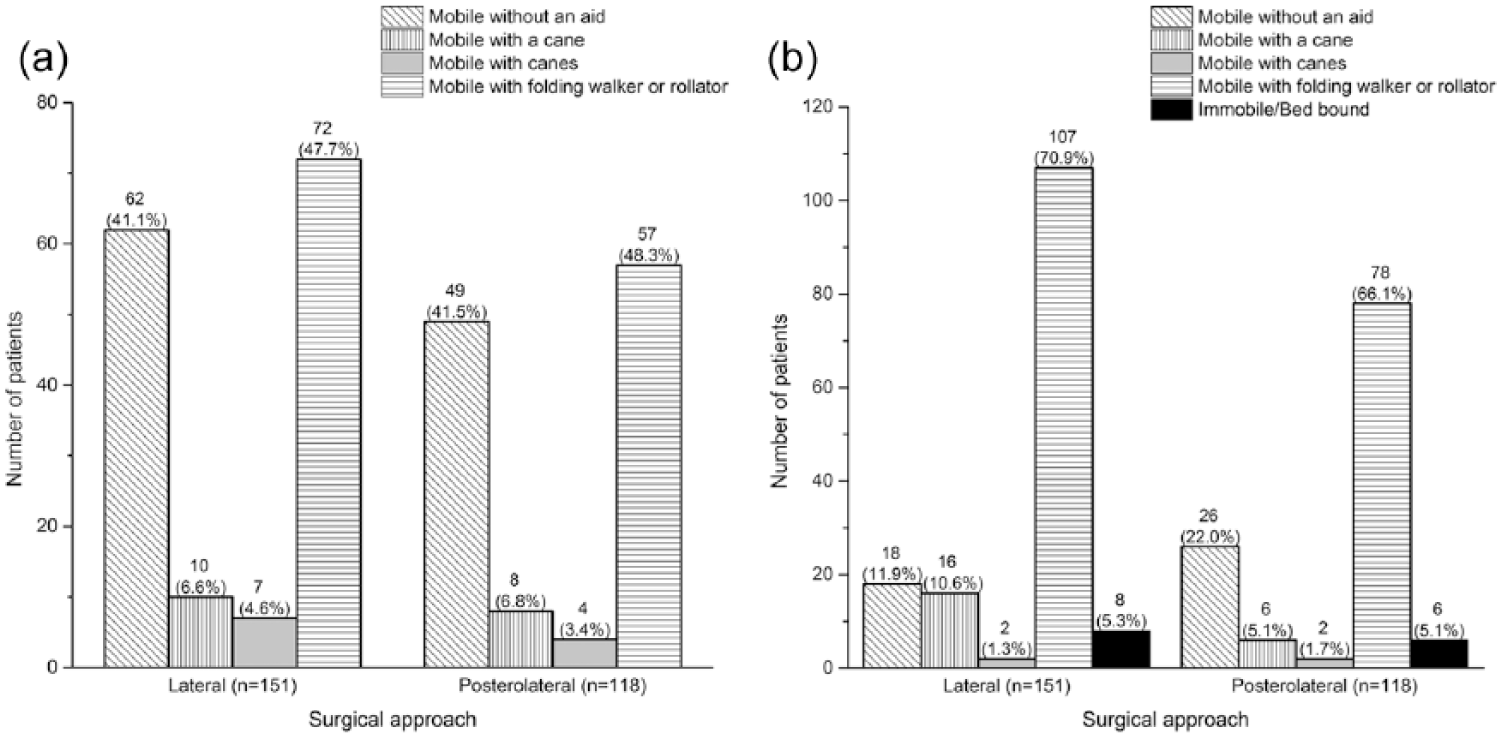
Details of ambulatory aids required at baseline and one year after hip fracture.
Pearson’s chi-square or Fisher’s exact test was used to compare the difference between categorical variables and Mann–Whitney U-test with continuous variables. A p value ≤0.05 was considered statistically significant. Predictive variables for the need of mobility aids 12 months after hip fracture were analyzed with age-adjusted univariate logistic regression analysis, and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. A multivariate logistic regression model was built using the enter method (all variables entered simultaneously into the model); variables with a p value ≤0.25 were included into the multivariate model, because more traditional levels (e.g. 0.05) can fail to identify variables known to be important (13).
A Cox regression model was built to compare survival between patients operated on using the lateral or posterior approach. For this model, we used a patient sample of 393, all of whom met the inclusion criteria. Age, sex, and delay to surgery represented covariates. All statistical analyses were performed using IBM SPSS Statistics version 23.
Results
Mean age of the 269 patients was 82.8 (standard deviation (SD) 6.3) years and 212 (79%) were women. The lateral and posterior surgical approaches were used in 151 (56%) and 118 (44%) patients, respectively. Prior to the hip fracture, 111 (41%) were able to ambulate without mobility aids, 205 (76%) moved unassisted or assisted outdoors, and 206 (77%) were living in their own home with or without organized home care (Table 1).
Table 2 shows the operative information and outcomes of several measured variables 1 year after hip fracture; the posterior approach was most often selected (p < 0.001). An uncemented stem was used more often in patients operated on using the lateral approach compared to the posterior approach (93% vs 80%; p = 0.002). No significant differences between groups were detected in the operation delay or need for blood transfusion. From 118 patients operated on using the posterior approach, 26 (22%) were able to ambulate without aids 1 year after hip fracture, but only 18 (12%) of 151 patients who were operated on using the lateral approach were able to ambulate without aids (p = 0.026). Furthermore, dislocations occurred in four (3.4%) patients in the posterior approach group compared with no patients in the lateral approach group. There was no difference in between groups in mobility level, pain in operated hip, and living arrangements 1 year postoperatively.
Comparison between direct lateral and posterior approaches with regard to operative information and outcomes 1 year after hip fracture.
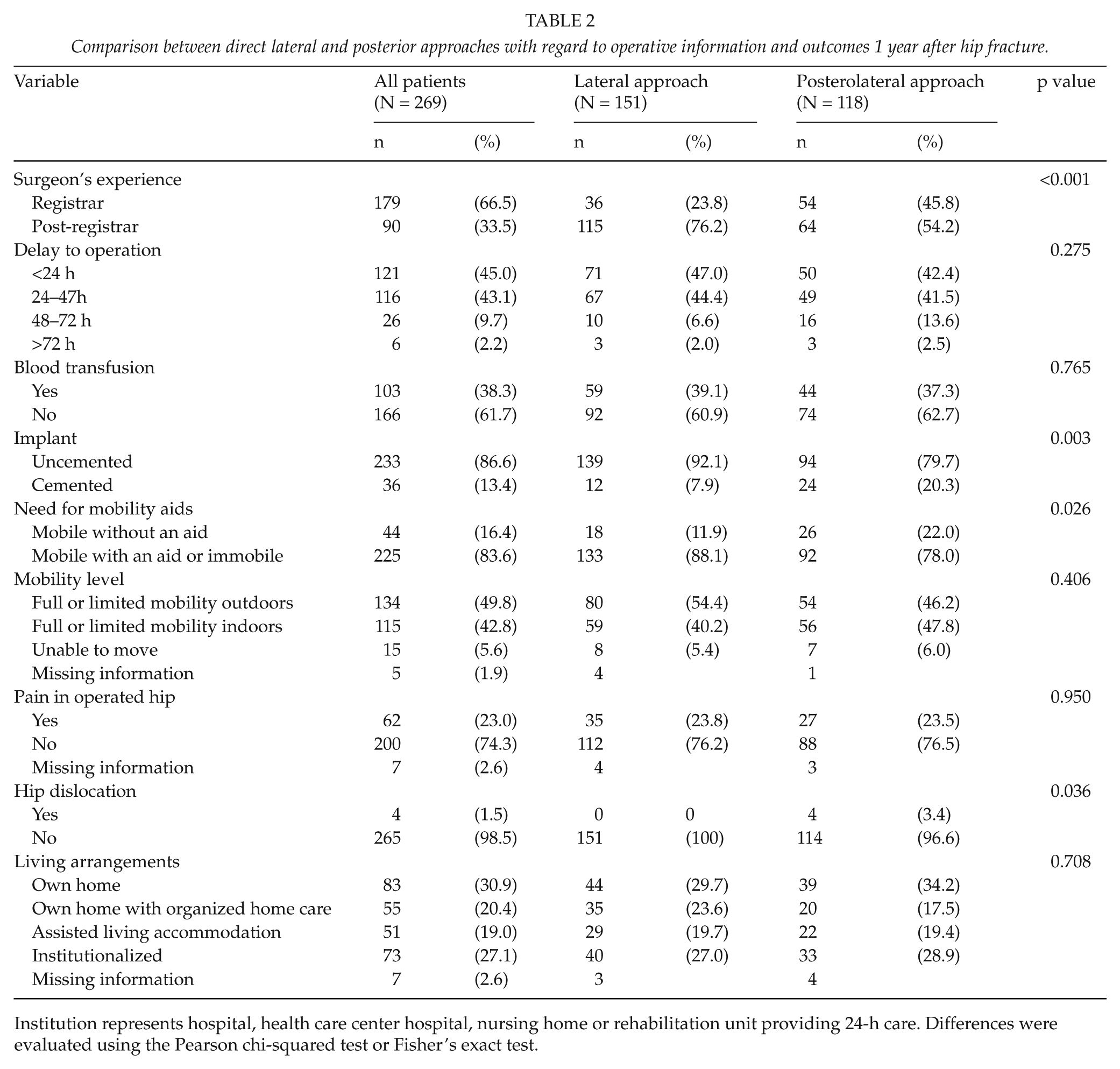
Institution represents hospital, health care center hospital, nursing home or rehabilitation unit providing 24-h care. Differences were evaluated using the Pearson chi-squared test or Fisher’s exact test.
Age-adjusted univariate logistic regression analysis revealed increased age, male sex, lateral approach, uncemented stem, previous need for ambulatory aids or immobility, mobility level, and previous living arrangements influence the need for mobility aids or immobility 1 year after hip fracture (Table 3). Multivariate logistic regression analysis indicated previous use of mobility aids or immobility (OR = 13.46, 95% CI = 4.29–42.25), age >85 years (OR = 3.83, 95% CI = 1.09–13.44), male sex (OR = 3.59, 95% CI = 1.05–12.22), and lateral approach (OR = 2.73, 95% CI = 1.15–6.50), as independent risk factors regarding the need for ambulatory aids or immobility (Table 3).
Age-adjusted logistic univariate and multivariate analysis regarding need for ambulatory aids 1 year after hip fracture.
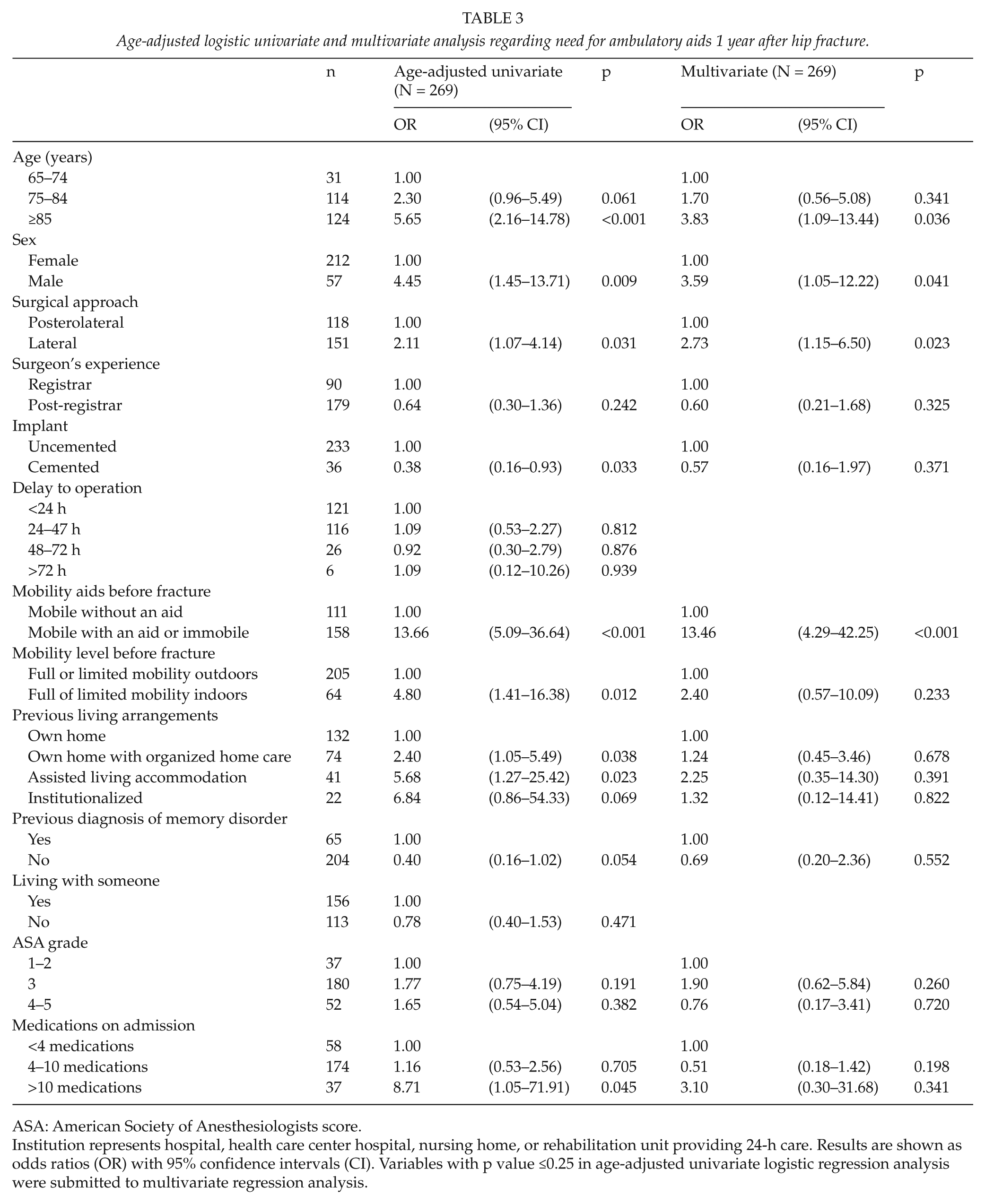
ASA: American Society of Anesthesiologists score.
Institution represents hospital, health care center hospital, nursing home, or rehabilitation unit providing 24-h care. Results are shown as odds ratios (OR) with 95% confidence intervals (CI). Variables with p value ≤0.25 in age-adjusted univariate logistic regression analysis were submitted to multivariate regression analysis.
The survival rates in postoperative months 1, 3, 6, and 12 were 91%, 84%, 81%, and 76%, respectively. In multivariate Cox regression analysis, death during the 1-year follow-up was predicted by age ≥85 years (hazard ratio (HR) = 2.56, 95% CI = 1.10–5.97), male sex (HR = 1.65, 95% CI = 1.08–2.54), and delay to surgery more than 72 h (HR = 2.65, 95% CI = 1.31–5.39), but lateral versus posterior approach had no statistically significant effect on the 1-year survival (HR = 1.36, 95% CI = 0.88–2.10; p = 0.166).
Discussion
Our findings revealed that fragility hip fracture patients who underwent HA using a posterior approach required fewer ambulatory aids 1 year after hip fracture than those who underwent HA using a lateral approach. The difference was mainly due to the increased use of a cane (5.1% vs 10.6%) and folding walker or rollator (66% vs 71%) by patients operated on using the lateral approach. No differences in survival, mobility level, living arrangements, and pain were established. The posterior approach, however, might predispose to hip dislocation compared with the lateral approach.
A previous study demonstrated that the lateral approach increases the risk of damage to the superior gluteal nerve and the gluteus medius muscle, which leads to limping secondary to abductor weakness in 4%–20% THA patients, but dislocation rate was only 0.55% (14). Furthermore, worse patient-reported outcome after the lateral approach compared to the anterior or posterior approach in primary hip arthroplasty is reported (15). Abductor weakness may increase the need for ambulatory aids among hip fracture patients operated on using the lateral approach. Moreover, fragility hip fracture patients may be more prone to abductor weakness compared with THA patients due to multiple comorbidities and impaired health condition, frailty, and sarcopenia in particular, which may attenuate tissue regeneration and healing processes of the re-attached gluteus medius insertion.
An interesting finding of this study is that regardless of the increased need for ambulatory aids among patients operated using the lateral approach, there was no significant difference in mobility level or pain between groups. Our results are consistent with those of a recent randomized controlled trial, which reported no notable differences in the pain and mobility outcomes between the two approaches (16). Furthermore, a prospective observational study found no difference between approaches in patient-perceived health-related quality of life (HRQoL), residual pain, or patient satisfaction 1 year after surgery on patients aged >70 years (17).
A recent register-based study, however, revealed that patients have more pain and are less satisfied with the operated hip after the direct lateral approach than after the posterior approach at 4, 12, and 36 months postoperatively. Furthermore, patients reported having more walking problems after the direct lateral approach even 36 months after surgery (18).
The posterior approach predisposes the patient to hip dislocation, but has fewer adverse effects on gait (14). The hip dislocation rate is reported to range from 5.1% to 16% among femoral neck fracture patients undergoing HA using the posterior approach, depending on whether or not posterior structures are repaired (19–21). Dislocation after hip HA is a rare complication that may increase mortality (22). Furthermore, even a single dislocation temporarily decreases the HRQoL, while recurrent dislocation results in a persisting deterioration of the HRQoL during the first year after the primary operation (23). In our study, the dislocation rate was relatively small compared to that in previously reported studies, which may be related to preservation of the piriformis tendon and repair of the posterior structures. All hip dislocations occurred in patients that underwent the posterior approach. Of the four hip dislocations, closed reduction successfully prevented additional surgery in only one patient.
Several risk factors affect discharge to own home after hip fracture, including age at admission, concomitant chronic systemic diseases and dementia, and walking disability before injury (24). The relationship between the surgical approach used among hip fracture patients undergoing HA and residential location postoperatively is not well studied. Abram and Murray (25) reported that increased age, male sex, cognitive impairment, dislocation, and delay to surgery represented risk factors for failure to return to own home within 30 days; surgical approach, however, was not a significant factor. Our study indicates that the posterior and lateral approaches produce similar outcomes with regard to residential location 1 year after hip fracture.
If the surgeon in charge is familiar with both approaches, careful patient selection may result in a favorable outcome. The complication rates are similar, but the posterior approach will result in a more than eight-fold risk of dislocation compared with the lateral approach. In contrast, the lateral approach may increase the risk of bleeding five-fold compared with the posterior approach (11). Postoperative hematoma was not a recorded variable in our study, but differences between groups in the need for blood transfusion during hospitalization were small and statistically non-significant. This may reflect the similar incidence of clinically relevant postoperative bleeding. Some risk factors for hip dislocation after HA are reported: posterior approach, cognitive impairment, and delay to surgery >24 h (10, 26, 27). A subpopulation of patients will benefit from either approach; patients with risk factors for hip dislocation may benefit from the lateral approach compared with the posterior approach. The surgeon’s use of a familiar approach, however, will most likely result in lower complications.
This study has several limitations. First, the patients were not randomized and the approach used depended on the respective surgeon’s preference, which may distort the results. Generally, patients with low compliance may be operated more often using Hardinge approach. However, in this study, patients who were immobile or bed bound before hip fracture were excluded. Moreover, the baseline characteristics did not differ according to surgical approach. Second, the sample size differed between groups. Third, data on implanted femoral stems and hip dislocations were retrospectively collected—all hip dislocations inside the referral area were admitted and treated at Seinäjoki Central Hospital. Hip dislocations occurring outside the hospital district, however, may not be part of the hip fracture database. Fourth, the use of uncemented femoral stems for the treatment of fragility hip fracture patients contradicts recent scientific evidence (28, 29). Uncemented stems were used more often in the lateral approach. Finally, because the number of patients using a cane, canes, or who were immobile was too small, we had to categorize the need for ambulatory aids in a dichotomous manner to perform the statistical analysis. At the beginning of the study, however, the proportional rates of uncategorized mobility aids did not differ comprehensively between groups. A major strength of this study is that patients represent a real-life population and the only exclusion criteria were age <65 years, pathological fracture, moderate-to-high energy hip fractures, and immobility. Second, new surgical protocols were not implemented and patients were provided similar postoperative care during the study period. Third, only 7.1% of patients were lost to follow-up.
In conclusion, HA using the lateral approach will increase the need for ambulatory aids at 1 year after hip fracture compared to the posterior approach 1 year, whereas the posterior approach increases the risk of hip dislocation. This study revealed no significant differences between the lateral and posterior approaches in the outcomes of survival, mobility, pain, and living arrangements 1 year after hip fracture.
Footnotes
Acknowledgements
Ms Kaisu Haanpää, RN, is also gratefully acknowledged for her expert collection and storage of the data. M.T.H., M.S.N., and H.K.P. were in charge and contributed to all stages of the study. O.V. contributed to reviewing the accuracy of the data and writing the final manuscript. T.L. contributed to the data interpretation. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Competitive State Research Financing of Seinäjoki Central Hospital.