
Abstract
Background and Aim:
During the last decade urban skiing and snowboarding has gained a lot of popularity. In urban skiing/snowboarding riders try to balance on handrails and jump off buildings. Previous studies in skiing and snowboarding accidents have mostly been conducted at hospitals located close to alpine terrain with big ski resort areas. The aim of this study is to evaluate the types and severity of traumatic brain injuries occurring in small, suburban hills and in urban environment, and to characterize injury patterns to find out the specific mechanisms of injuries behind.
Materials and Methods:
This study included all patients admitted to the Helsinki University Hospital Trauma Unit from 2006 to 2015 with a head injury (ICD 10 S06-S07) from skiing or snowboarding accidents in Helsinki capital area. Head injuries that did not require a CT-scan, and injuries older than 24 hours were excluded from this study.
Results:
There were a total of 72 patients that met the inclusion criteria Mean length of stay in hospital was 2.95 days. According to the AIS classification, 30% had moderate, 14% had severe, and 10% had critical head injuries. Patients who got injured in terrain parks or on streets where more likely to be admitted to ICU than those injured on slopes. Based on GOS score at discharge, 78% were classified as having a good recovery from the injury, 13% had a moderate disability, 5% had a severe disability and 3% of the injuries were fatal. There were no statistically significant differences in decreased GOS between the accident sites.
Conclusion:
Head injuries occurring in small suburban hills and in urban environments can be serious and potentially fatal. The profile and severity of skiing injuries in urban environments and small, suburban hills is comparable to those on alpine terrain.
Background and Aim
Alpine skiing and snowboarding share the hazards of high speed and both have a reputation of a risky sport due to frequent head injuries (1, 2) These head injuries can cause severe debilitation or even death, and also result in a high financial burden to society and to individuals.
During the last decade urban skiing and snowboarding has gained a lot of popularity. In urban skiing/snowboarding riders try to balance on handrails and jump of buildings. Urban riding tricks are similar to riding in terrain parks with jumps and manmade obstacles, but take place in residential and industrial urban areas. Major difference is that often tricks are performed on stairs and nearby standing stationary objects. Urban skiing and snowboarding combine high speed with the potential for collision with stationary objects, and risk of falling from heights.
Head injuries are the leading cause of death in downhill skiing and snowboarding accidents in adults (3), and traumatic brain injury is the leading cause of downhill skiing injury fatalities in children as well (4, 5).
However, most of the previous studies have been conducted at hospitals located close to alpine terrain and high mountains with big ski resort areas.
In Greater Helsinki (50 km radius from Helsinki), there are only small resorts with slopes less than 80 meters of vertical height, resulting in a completely different kind of skiing compared to major resorts. In urban skiing, Helsinki is known for being the ‘mecca’ of European urban rails. The lack of mountains has led urban skiing and snowboarding to gain popularity in Greater Helsinki during the last decade.
Most studies on the demographics and epidemiology of ski- and snowboard related injuries have been based on emergency department visits or ski-resort clinic data.
Still there are only few studies on the nature and outcome of patients hospitalized with more serious head injuries resulting from skiing and snowboarding accidents. We could not find any previous studies conducted on urban skiing/snowboarding. The aim of this study is to evaluate the types and severity of more serious traumatic brain injuries (TBI) occurring in small, suburban hills and urban environment skiing and snowboarding, and to characterize injury patterns to find out the specific mechanisms of injuries behind these.
Materials and Methods
This study included all patients admitted to the Helsinki University Hospital Trauma Unit from 2006 to 2015 with a head injury (ICD 10 S06-S07) from skiing or snowboarding accidents in Greater Helsinki (50 km radius from Helsinki). Head injuries that did not require a CT-scan or an MRI and injuries older than 24 h were excluded from this study, as well the injuries taking place outside of 50 km radius from Helsinki.
There are 12 small resorts within the 50 km radius from Helsinki that generally are open from December to April. The average elevation difference in these resorts is 62.5 meters (range 30-84 meters) and a total of 33 ski lifts that transport the skiers/visitors up the hill.
For the purposes of this study, the place of injury was divided into three categories; ski resort slopes, terrain parks, and urban. Urban skiing was defined as skiing or snowboarding outside skiing resorts within streets of the cities.
Hospital records were retrospectively reviewed for data collecting: equipment used (skis or snowboard), age, gender, use of helmet, site of injury, mechanism of injury, intubation, transport method, Glasgow Coma Scale/GCS motor component at admission, pupil size and reactivity, other injuries, head CT-scan finding according to AIS (2005 version) classification (if repeated CT scans, the one 24 hours post injury was reviewed), length of stay in hospital and Glasgow Outcome Scale (GOS). Traumatic brain injury was done classification was done from CT-scans usin ICD-10 and severity according to AIS.
Following text is added to the end of the third chapter in methods” The Abbreviated Injury Scale (AIS) is an anatomical-based coding system to describe the severity of injuries. The score describes three aspects of the injury (type, location and severity).
Abbreviated Injury Scale severity score is on a scale of one to six, one being a minor injury and six being maximal (currently untreatable).
Glasgow Outcome Scale (GOS) is perhaps the most widely used measure for assessing global outcome following a brain injury. The scale divides into outcome categories that allow standardized descriptions of the objective degree of recovery. Patients are assigned to one of five possible outcome categories: 1) death, 2) persistent vegetative state, 3) severe disability, 4) moderate disability, and 5) good recovery (6).
Results are presented as means ± SD for continuous non-skewed variables. The frequency distribution of the categorical variables is compared between the groups with the Chi-square test. Statistically significant level is set as p < 0.05. Statistical program SPSS (IBM Corp. released 2009. IBM SPSS Statistics for Windows, version 13.0. Armonk, NY: IBM Corp.) was used for analysis. The study protocol was approved by Helsinki University Hospital’s Review Board.
Results
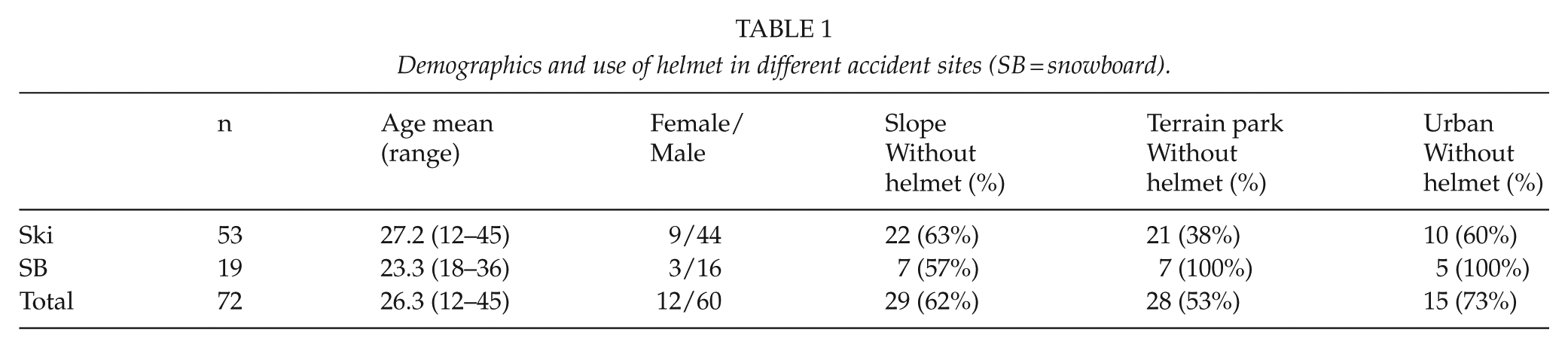
There were a total of 72 patients during the 10-year study period that met the inclusion criteria. The patient demographics and mechanisms of injuries in different accident sites are presented in Tables 1 and 2, respectively. Nine of the skiers were pediatric patients (under 16 years old). There were no significant differences in type of injury, injury mechanism or outcome between pediatric patients and adults.
Demographics and use of helmet in different accident sites (SB = snowboard).
Mechanism of injuries in ski resort slopes, terrain park areas, and in urban areas.
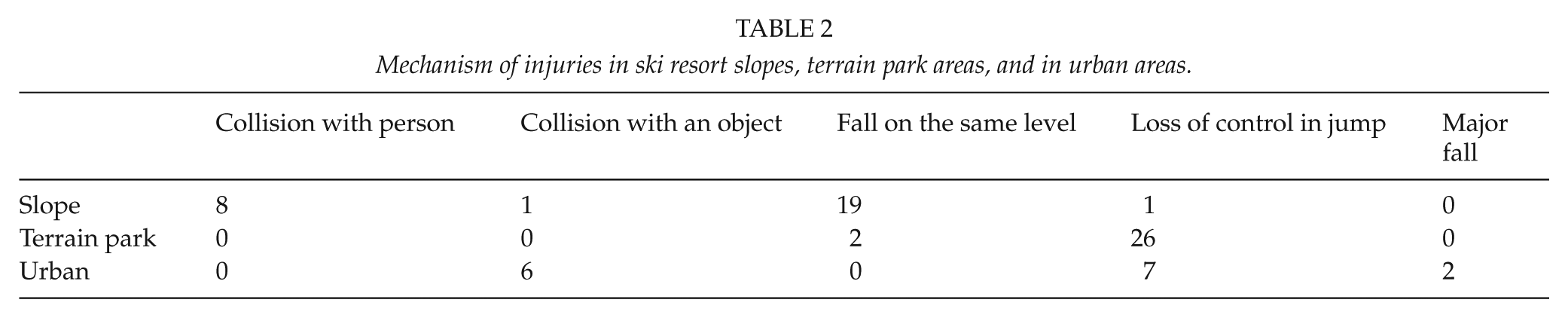
Among skiers head injuries were due to loss of control in jump (n = 22, 41%), falling down on the same level (n = 14, 26%), collision on an on slopes with another person (n = 6, 11%), and collision with an immovable object (n = 4, 7%). Two patients were injured due to a major fall (over 3 meters) while trying to balance on a handrail. Snowboarding injuries were due to loss of control in the jump (n = 10, 52%), falling down on the same level (n = 6, 32%), collision with an immovable object (n = 2, 11%), and collision on an on slope with another person (n = 1, 9%). The detailed information on head injuries in respect of accident sites is presented in Table 3.
The type of head injuries according to helmet use in 72 patients suffering ski or snowboard related TBIs. Values are given as medians, range in parenthesis.
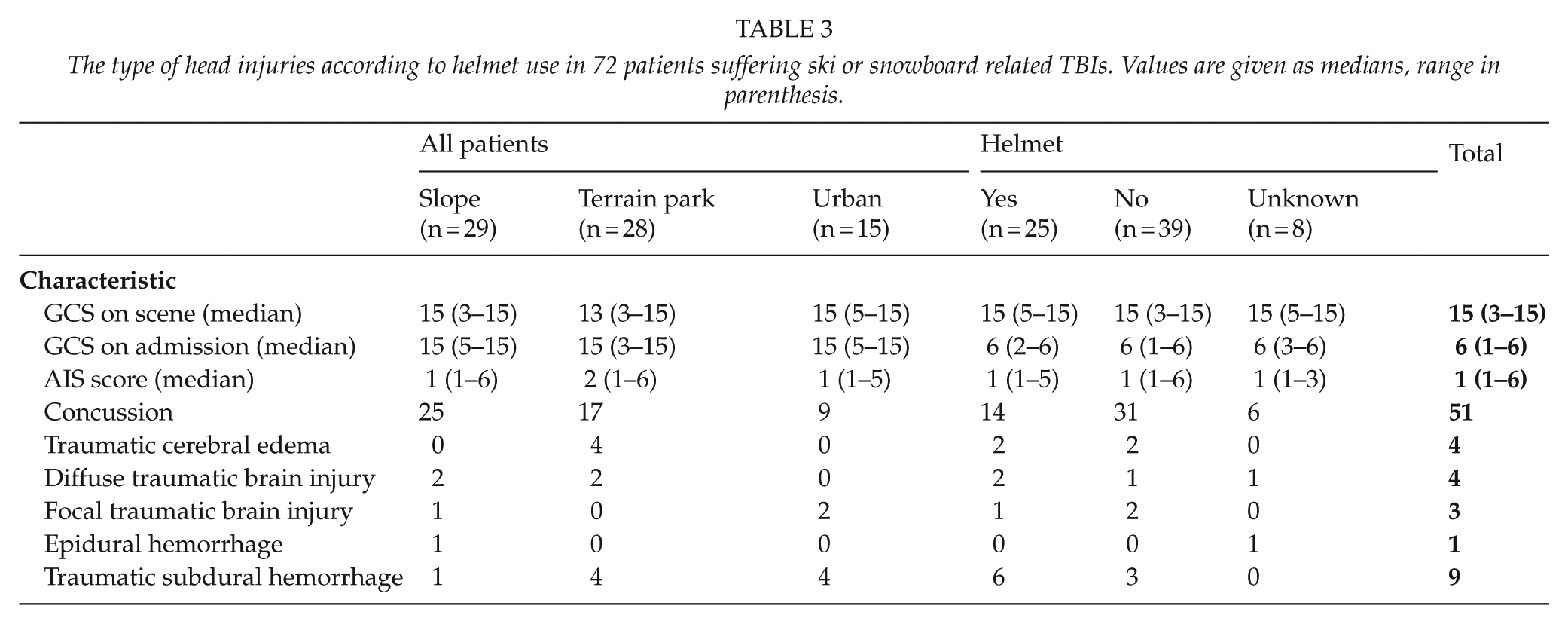
54% (n = 39) of the patients had a primary GCS below 15 on scene and 38% (n = 27) on admission to hospital. Eleven patients (15%) had a GCS score below nine on scene but only eight patients had GCS score below nine on admission. 18% (n = 13) of the patients had a decreased GCS motor component on admission and that was more likely due to terrain parks or urban environment injuries compared to slope injuries (26% vs. 6%; p < 0.05). 70% of the patients had isolated head injuries in the absence of other associated trauma. Most common associated trauma was injuries to extremities with 10 (14%) patients followed by neck injuries among 7 patients (10%). Four patients (6%) had more than three associated injuries (neck, thorax and extremities).
According to the AIS classification, 30% (n = 22) had moderate (AIS 2), 14% (n = 10) serious (AIS 3), 14% (n = 10) severe (AIS 4), and 10% (n = 7) had critical (AIS 5) head injuries. There were no statistically significant differences in mean head AIS between the accident sites.
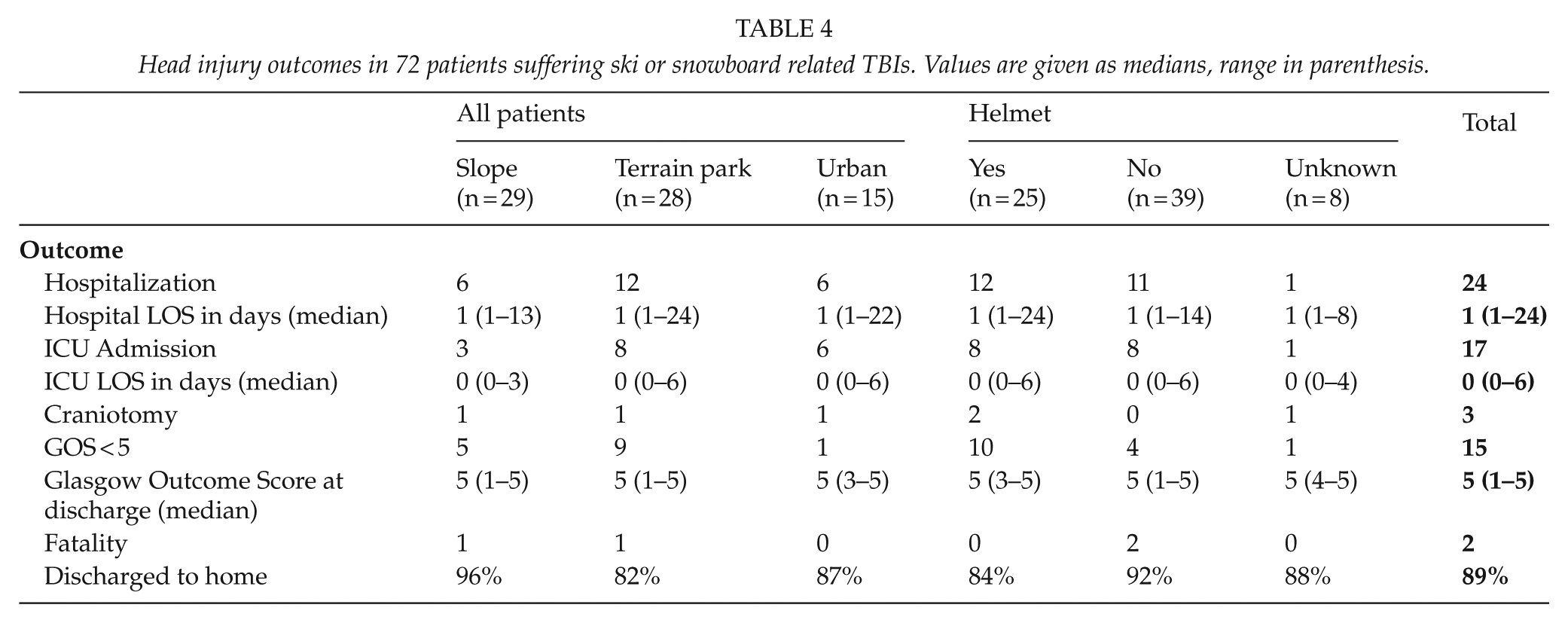
The mean length of stay in hospital was 2.95 (SD 2.96) days for the whole study population. A total of 17 patients were admitted to ICU. Patients who got injured in terrain parks or on streets where more likely to be admitted to ICU than patients injured on slopes (29%, 40% vs. 10%, p < 0.05). Compared to those not wearing a helmet with those who were wearing a helmet, there were no statistically significant differences in hospitalization (48% vs. 28%; p > 0.05) or in ICU admission (32% vs. 20%; p > 0.05).
Based on the GOS score at discharge, 78% (n = 57) were classified as having a good recovery from the injury (GOS 5), 13% (n = 9) had a moderate disability (GOS 4), 5% (n = 4) had a severe disability (GOS 3), and 3% (n = 2) died (GOS 1). No patients were in a persistent vegetative state. Majority of the patients (89%) were discharged to home. Majority of the patients (89%) were discharged to home. Two patients (3%) were stepped down to other hospitals for further care. Both patients had suffered traumatic subdural haemorrhage and spinal injury to lumbar spine. Four patients (6%) were transferred to rehabilitation facilities. Three of these four patients had suffered traumatic subdural haemorrhage and one patient had epidural haemorrhage and multiple facial fractures. We could not find statistically significant differences in decreased GOS (less than 5) regarding the use of helmet or no helmet (26% vs. 3%; p > 0.05). There were no statistically significant differences in decreased GOS between the accident sites terrain park 33%, urban 20% and slopes 10%; p = 0,18). The detailed information on the outcome in respect of accident sites are presented in Table 4.
Head injury outcomes in 72 patients suffering ski or snowboard related TBIs. Values are given as medians, range in parenthesis.
There were two fatal injuries due to head trauma. One patient was struck by a snow groomer and had an initial GCS of 3. He underwent endotracheal intubation at the scene, was transported by helicopter to the hospital, and admitted to the ICU, where he subsequently died secondary to a severe subdural haemorrhage. The other patient had a collision with an immovable object in a terrain park, arrived at the accident and emergency department with an absent pulse, a GCS of 3, and fixed and dilated pupils. Neither of these patients was wearing a helmet.
Discussion
In this study we found that even on very small slopes and in urban environments, head injuries from skiing and snowboarding accidents can be serious and even fatal. Most prior studies of ski and snowboard related trauma have been based on hospital emergency room visits or mountain ski-resort clinic data (1, 7–9). Even though head injuries comprise only 3–15% of all injuries in skiers and snowboarders, it appears that the incidence of TBI is increasing (1, 10–12). The reason for that is still unknown. The data from this study population, which was limited to persons who were referred to a tertiary level clinic, represents only a fraction of the total number of ski-related head injuries in southern Finland, and therefore it was impossible to estimate incidences. The reason behind increased incidence can be increased risk-taking behaviours that snow sports and the energy drink industry have embraced and advocated. During the last decade many resorts have built bigger terrain parks, which contain man-made features used for jumping or performing aerial manoeuvres and these appear to have increased the risk and/or severity of injuries. The same trend has been seen in urban riding where skiers and snowboarders try acrobatic manoeuvres while jumping down stairs or off buildings or trying to balance on handrails.
The patient demographics in this study, which included a mean age of 26,3 years and male majority (12/60) is consistent with earlier studies conducted on ski and snowboard related head trauma (7, 13, 14).
Levy et al. (3) found that the majority of head injuries were concussions but 14% of patients suffered severe brain injuries with an overall mortality rate of 4%. In this study the majority (70%) of the head injuries were concussions and 30% of the injuries were severe. This study was conducted at a tertiary level hospital where the most seriously injured patients are referred. This study examined only those individuals who had sustained the more severe trauma and were triaged to have head CT done which can explain the higher number of severe head injuries.
It is estimated that head injuries are the cause of 59-88% fatalities in skiing and snowboarding related injuries (5, 15, 16). The mortality rate, including prehospital mortality, was 3% in this study population, which is consistent with earlier studies (3, 7, 16). Urban environments and local ski hills close proximity to hospital with neurosurgical capability, which has been shown to decrease mortality and improve outcome (17–19), probably may have resulted lower mortality rate and better Glasgow outcome scores.
It has been documented in earlier studies that injuries taking place in jumps are more likely to be severe in nature and more likely require an ambulance transfer (9, 10, 20, 21). In our dataset, skiers and snowboarders that were injured in terrain parks or on streets had more severe head injuries and had a worse injury outcome than those on slopes. Regardless of the place of injury, patients who collided with an object had the most severe injuries followed by patients who lost control while jumping. But these results were not statistically significant due to the small study population.
Even though in this study 30% of the injuries were severe head injuries, the majority of head injuries (79%) achieved a good outcome as measured by GOS. However, 13% of the patients had a moderate disability at discharge. Studies of ski-related injuries in Switzerland (14) and USA (7) reported 68% and 79% of patients respectively achieving a GOS 5 at discharge.
Because of the small study population and the lack of a control group we could not estimate the protectiveness of helmets. We found no statistically significant differences between patients with helmets and without helmets in hospitalization or injury outcome therefore no conclusions on helmet use and injury outcome shouldn’t been drawn based on this study. A recent study by Sulheim et al. (22) found that the use of helmets has increased but they observed an unexpected reduction in the protective effect of a helmet. There exists controversy about the precise degree of efficacy of helmets in protecting against injury but earlier studies support the use of helmets for both skiing and snowboarding (23, 24). Noteworthy in our study population was that all snowboarders who suffered a head injury either in terrain parks or in urban environments were not wearing helmets. Reason behind this is unknown - it is possible that it is a statistical bias due to the small study population. It is also possible that helmet wearing among snowboarders is not considered trendy or it is not felt necessary when snowboarding on small hills or in the streets.
The major limitation of this study is the retrospectivity of the study and the small study population. Also, it is likely that all injuries were not included in the data, since some of the less injured patients have sought for medical assistance at other hospitals introducing selection bias. Helsinki University Hospital is a tertiary level hospital where the most seriously injured patients are referred. This study examined only those individuals who had sustained the more severe trauma and were triaged to have a head CT-scan done. Therefore it was impossible to count for incidence of head injuries or the protectiveness of helmets therefor no conclusions on helmet use and injury outcome shouldn’t been drawn based on this study. Statistical analysis was difficult due to small number of patients, which makes beta error possible.
Although a wide variety of demographic and environmental characteristics were collected, important confounders were not available from hospital records, such as the manoeuvre being attempted on the feature (inverted jumps) or the size of the feature or the speed at the time of impact. Repeated head CT were not done routinely for every patient, but only in cases when the patient’s condition deteriorates during hospital admission or when the initial CT was showing injury that may need surgery if intracranial injury should extend. Thus, decision of repeated head CT is done individually in every case. This may cause some minor bias in grading the initial injury according to CT scans, since there is a possibility that initial extend of the injury can slightly increase during 24 hours even the clinical condition of the patient remains unchanged. Which, naturally, will not be detected if no routine control of 24 h CT is done.
To avoid head injuries, we strongly recommend the use of helmets especially in terrainparks and in urban riding on stairs and concrete instead of snow. We have to emphasize the importance of proper terrain park design with safety nets, signs, and adequate grooming of the jumps and landings to reduce the risk of injuries. Urban environments are not designed for skiing or snowboarding even though many of riders think so and education and risk awareness should be emphasized.
Conclusion
Head injuries on small hills and in urban environments can be serious and potentially fatal. The skiers and snowboarders injured in terrain parks or on streets had more severe head injuries than those on slopes. The injury profile and severity in small ski resort injuries is comparable to those on alpine terrain and high mountains. TBIs can greatly affect the quality of life and pose a high financial burden to society and to individuals. As participation in these sports increases, understanding the mechanisms and injury pattern of TBIs will greatly assist in implementing effective medical prevention programs and proper safety equipment practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.