
Abstract
Background and Aims:
The aim of this study was to provide information on incidences and severity of recreational alpine skiing and snowboarding injuries in Northern Finland and to discuss possible preventive measures to reduce the number and severity of injuries in the future.
Materials and Methods:
This retrospective study consists of all injured skiers and snowboarders in the Levi Ski Resort during the 2006–2012 winter seasons. The Levi Ski Resort has a SKIDATA® system which records automatically every ski-lift run taking place. The emergency system of the resort registers the data (conditions during the injury, patient characteristics, and observed and/or suspected injuries) of all injured persons they meet. The severity of injury is defined by the needed level of care: Grade 1 (treated by the emergency system with no need for further referral), Grade 2 (referral to the local primacy care clinic), Grade 3 (transfer to hospital by ambulance), and Grade 4 (transfer to tertiary care by helicopter).
Results:
During the 6-year study period, there were 29,576.132 lift runs and 2911 injuries were met by the emergency system, resulting in the average injury incidence of 0.98 injuries per 10,000 lift runs. Vice versa, the average number of the ski-lift rides needed to generate one injury was 10,160. The knee injuries of the skiers constituted almost one-third of all cases, whereas snowboarders sustained more injuries to the upper limb and axial areas.
Conclusion:
Skiing and snowboarding are related to a relatively high risk of injury. The most common injuries affect the knee in skiers and the upper extremity, especially the wrist, in snowboarders. A continuous and systematic review of injuries is needed to monitor the effects of changes made in terms of the safety.
Introduction
Alpine skiing and snowboarding are popular winter activities in Finland. Alpine skiing has for years had a reputation as a risky sport for skiers due to frequent knee injuries and lower leg fractures. Improvements in bindings, ski boots, and slope grooming technologies have reduced the number of tibial fractures and minor knee strains (1). However, severe ligament tears of the knee as well as severe head injuries are still unresolved problems.
The overall injury rate among recreational skiers is approximately 3 injuries per 1000 skier days (1, 2). Alpine skiing and snowboarding share the hazards of high speed and alpine terrain. The equipment and body mechanics of each sport are different, exposing participants to a distinct assortment of risks and different types of injuries (3). Among skiers, the knee has been reported as the most common site of injury, accounting for 20%–27% of all skiing injuries (4–6). Snowboarders are affected by other types of injuries and they also experience a higher injury rate of 4–16 injuries per 1000 snowboarder days (7). In the literature, it is widely accepted that snowboarders are at an increased risk of head and upper arm injuries, chiefly wrist injuries (4, 8–11). Skiing accidents in different countries may not always follow the same pattern of injury or incidence. Consequently, there is a need for local studies with the aim of finding useful preventive measures to reduce the number and severity of injuries. The purpose of this study was to provide accurate information on the incidence of alpine skiing and snowboarding injuries in Northern Finland, to assess the prevalence and severity of such injuries, and to discuss possible preventive measures to reduce the number and severity of injuries in the future.
Patients and Methods
The present retrospective study covers six seasons (2006–2012), assessing injured recreational alpine skiers and snowboarders at the Levi Ski Resort Ltd., Finland.
According to the annual number of visitors, the Levi Ski Resort is the busiest ski resort in Finland (over 4 million ski-lift runs in the season of 2011). The ski season is 130–140 days on average, starting normally on late October and lasting to May. The Levi Ski Resort has a SKIDATA® system which records automatically every ski-lift run taking place, thus resulting in a reliable number of actual runs down the slopes.
The Levi Ski Resort emergency system meets the injured skiers in two ways: either the person himself or herself contacts emergency system after the injury or, in more cases, the injured person is evacuated from the injury scene by the response team. The emergency system registers the data of all the injured persons they meet. The data consist of injury conditions, patient characteristics, and noted and/or suspected injuries. This retrospective study was based on this registered data. Skiing and snowboarding injuries were defined as any type of injury incurred during downhill sport activity or lift transportation in persons met by the emergency system.
The injuries were classified according to the injured body site and the type of injury. Clavicle injuries were classified as shoulder injury. The emergency system does primary triage only by clinical assessment and is not able to make more accurate diagnoses needing, for example, radiological examinations. In this study, the injury types were classified according to eight primary triage findings: (1) contusion, (2) distortion/strain, (3) suspected fracture, (4) open fracture, (5) laceration/wound, (6) commotion, (7) unconsciousness over 10 min, and (8) dislocation. The severity of injury was classified into four categories by the needed level of care: Grade 1 injury (patient was treated by the emergency system with no need for further referral), Grade 2 injury (patient was transferred to the local primacy care clinic), Grade 3 injury (patient was transferred to hospital by ambulance), and Grade 4 injury (patient was transferred to tertiary care by helicopter). We defined Grade 1 injuries as minor, Grade 2 injuries as moderate, Grade 3 injuries as severe, and Grade 4 injuries as critical.
The injury incidence was calculated by using the annual number of ski-lift runs provided by the SKIDATA® system. The incidence is presented as the number of injuries per the number of 10,000 ski-lift runs. In addition to the observed incidence, we estimated the injury rate for 1000 skier days by using the method described by Bergstrom and Ekeland (12, 13), where 20 ski-lift ascends count as one skier day. The study protocol was approved by the hospital administrative board.
Results
During the 6-year study period, there were 29,576,132 lift runs, and altogether 2911 injuries were recorded. The average injury incidence was 0.98 injuries per 10,000 lift runs (annual variation from 0.82 to 1.08, Fig. 1). Vice versa, the average number of ski-lift rides needed to generate one injury was 10,160. The estimated mean injury rate was approximately 1.97 per 1000 skier days, which makes the mean days between the injury (MDBI) 508 days. Skiing was associated with 1991 (68%) cases, snowboarding with 893 (31%) cases, and other (monoski, snow bikes, snowblades, etc.) in 27 (1%) cases. The mean age for the entire population was 24 years (range 3–82 years). However, the mean age for snowboarders was 21 years (range 7–66 years), whereas the mean age for skiers was 24 years (range 3–82 years). Injuries occurred slightly predominately in male both in snowboarding (55%) and in skiing (57%).
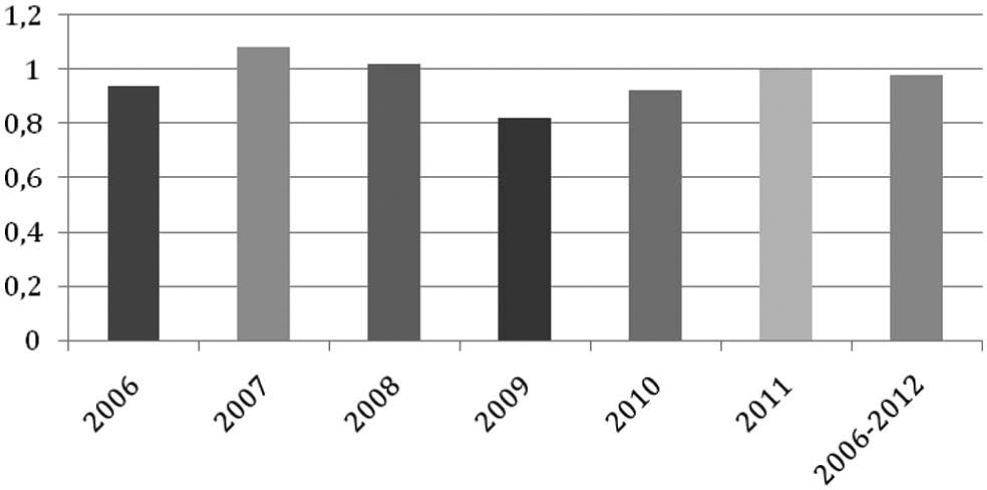
Recorded injuries per 10,000 lift runs during the study period of 6 years.
In skiers, the majority of accidents (1430, 72%) took place in slope on-piste areas, while 388 injuries (19%) took place in terrain parks, 112 (6%) during ski-lift taxi, and 61 (3%) in off-piste areas. The injuries were due to falling down on the same level (1246, 63%), loss of control in jump (388, 19%), collision on an on-piste area with another person (156, 8%), and collision with an immovable object (142, 7%). However, only 3% of the injuries due to loss of control while jumping occurred in females. In snowboarders, 70% (632) of the accidents took place in slope on-piste areas, followed by accidents in terrain parks (221, 25%), during ski-lift taxi (25, 3%), and in off-piste areas (27, 3%). Snowboarding injuries were due to falling down on the same level (616, 69%), loss of control in jump (212, 24%), collision with an immovable object (26, 3%), and collision on an on-piste area with another person (24, 3%). The ski-patrol evacuated 720 (36%) injured skiers and 280 (31%) injured snowboarders from the slopes. The most common reason for referring the patient to further care was the need for X-ray in Grade 2 patients and major fracture or suspicion of it in Grade 3 patients. The location of injuries (Fig. 2) and the distribution of the severity of injuries in presented locations are shown in Table 1.
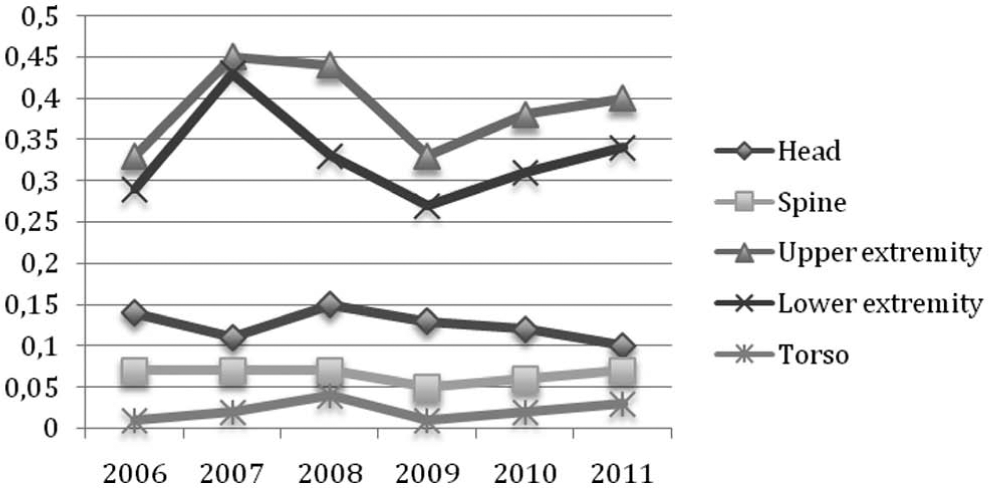
Anatomical injury location per 10,000 lift runs during the study period of 6 years.
Location of injuries (bold) and distribution of the severity of injuries in presented locations (italic).
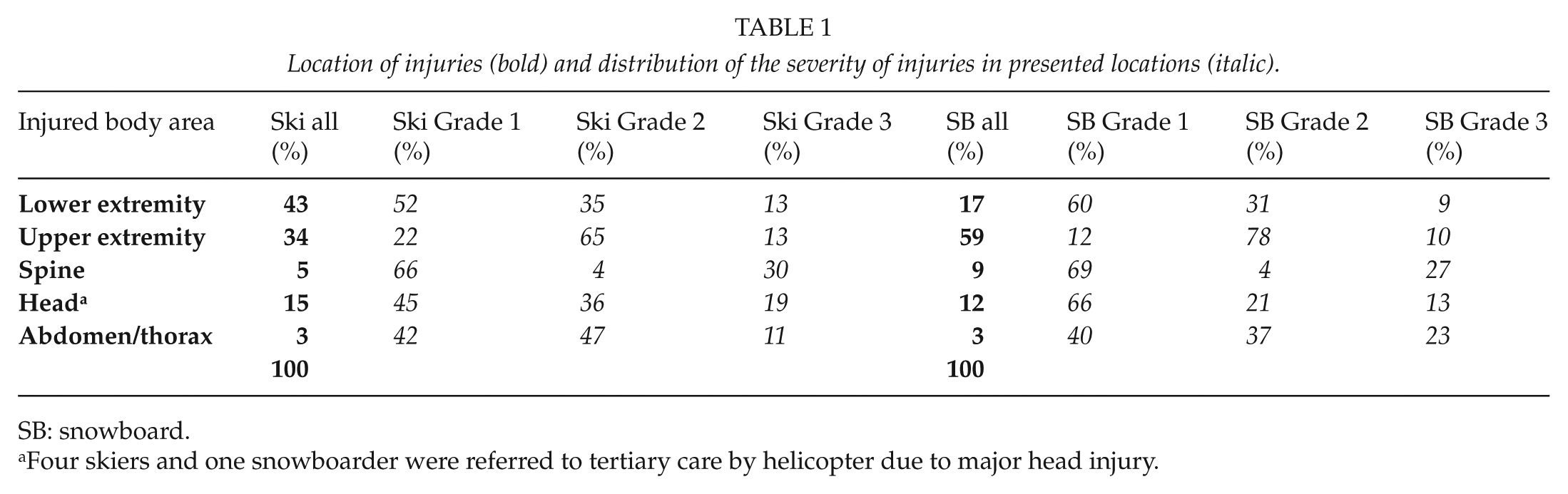
SB: snowboard.
Four skiers and one snowboarder were referred to tertiary care by helicopter due to major head injury.
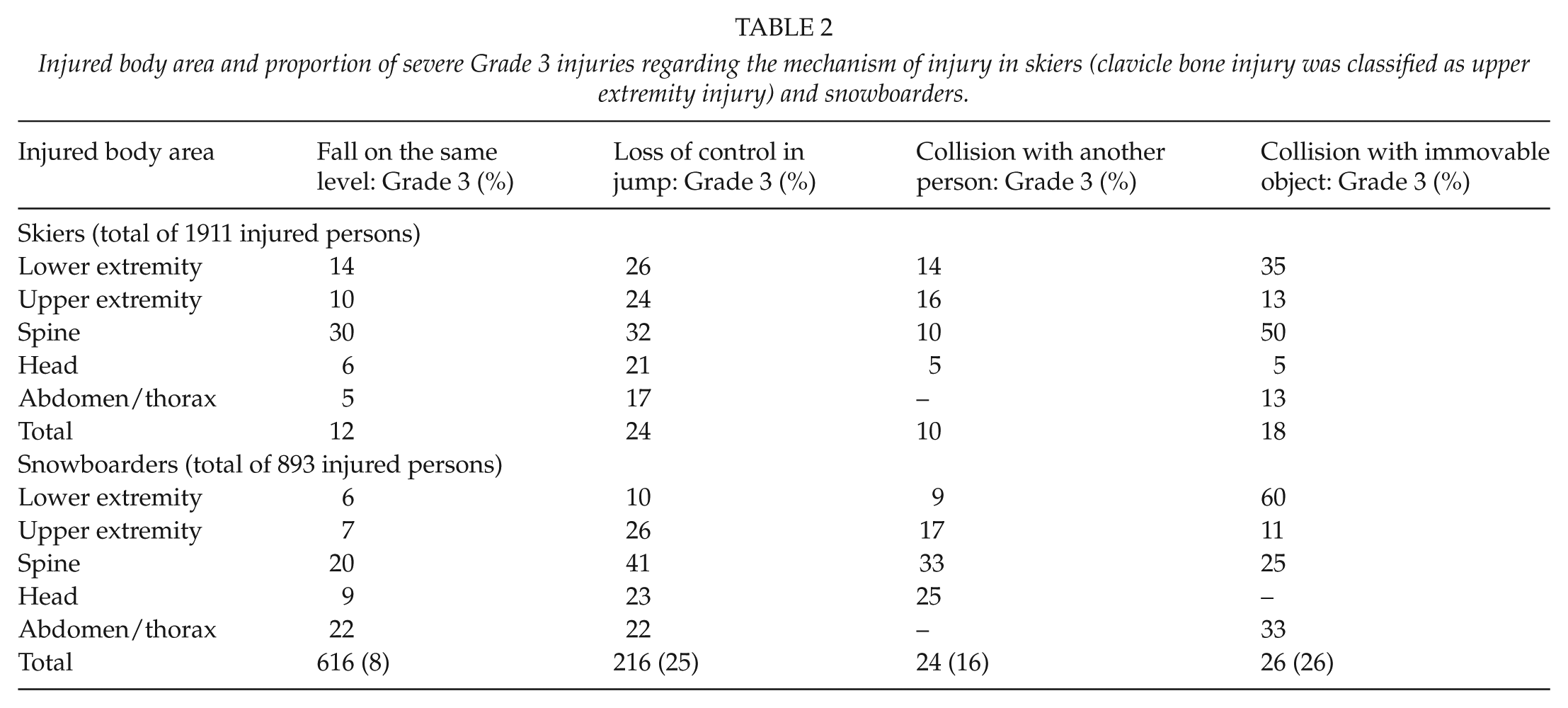
During the study period of 6 years, four skiers and one snowboarder were transferred to hospital by helicopter due to major head injury. The emergency system met nine fatalities during the study period, but they were all due to a medical condition and none of them occurred in ski slopes during downhill activities. Out of the skiing injuries, 15% (298) were classified as severe, 44% (879) as moderate, and 41% (810) as minor. In snowboarding, the figures were 13% (112), 53% (471), and 34% (310), respectively. The injured body area and the proportion of severe Grade 3 injuries regarding the mechanism of injury in skiers and snowboarders are presented in Table 2.
Injured body area and proportion of severe Grade 3 injuries regarding the mechanism of injury in skiers (clavicle bone injury was classified as upper extremity injury) and snowboarders.
In skiers, the injured body part was lower extremity in 42% (846) of the cases, upper extremity in 34% (680), head in 15% (298), and spinal column in 6% (120) of the cases. In snowboarders, the respective figures were lower extremity in 17% (148), upper extremity in 59% (525), head in 12% (106), and spinal column in 9% (83) of the cases. Out of all lower extremity injuries, 68% and 47% were knee and 26% and 33% lower leg and ankle injuries in skiers and snowboarders, respectively. In the upper extremity injuries, 38% and 26% were affecting shoulder and 27% and 61% the wrist, hand, or thumb in skiers and snowboarders, respectively.
Discussion
We found the average injury incidence among skiers and snowboarders to be 1.0 (0.98) injuries per 10,000 lift runs. In other terms, there has to be an average of 10,160 ski-lift rides to generate one injury. By recording every ski-lift ride, the SKIDATA® system gives an exact injury incidence related to the number of lift rides. However, we could not find previous studies on the incidences of recreational skiing injuries conducted by the comparable method. Thus, we cannot compare our exact incidence rate to previous studies published on recreational skiing.
The International Ski Federation (FIS) is running an injury surveillance system among race skiers and presents an injury incidence per 9.8 per 1000 ski runs (14). However, there are some differences in the overall injury patterns and incidence between alpine ski racers and recreational skiers (14, 15). In addition to the observed exact incidence of injuries per 10,000 lift runs, we also estimated the injury rate for 1000 skier days by using the method described by Bergstrom and Ekeland (12, 13), where 20 ski-lift ascends count as one skier day. By that method, our estimated injury rate for 1000 skier days was lower than that in previous studies done in the United States and continental Europe (1–3, 16, 17) but similar to that in Nordic studies (18–20). It has been speculated that Nordic people are more experienced skiers than American and European skiers, which could be one of the reasons for lower injury rates in the Nordic countries compared to other countries around the world. Furthermore, Nordic ski resorts, especially the ones in Finland, are smaller with fewer steep slopes compared to North American and continental European resorts. In addition, most of the Nordic ski resorts are well groomed and use artificial snow makers to even out the differences in conditions between the warmer and colder months, which make the slopes safer for the skiers. In Table 3, the characteristics of ski resorts with previously published injury incidences among recreational skiers and snowboarders are shown.
Characteristics of ski resorts with previously published injury incidences among recreational skiers and snowboarders.
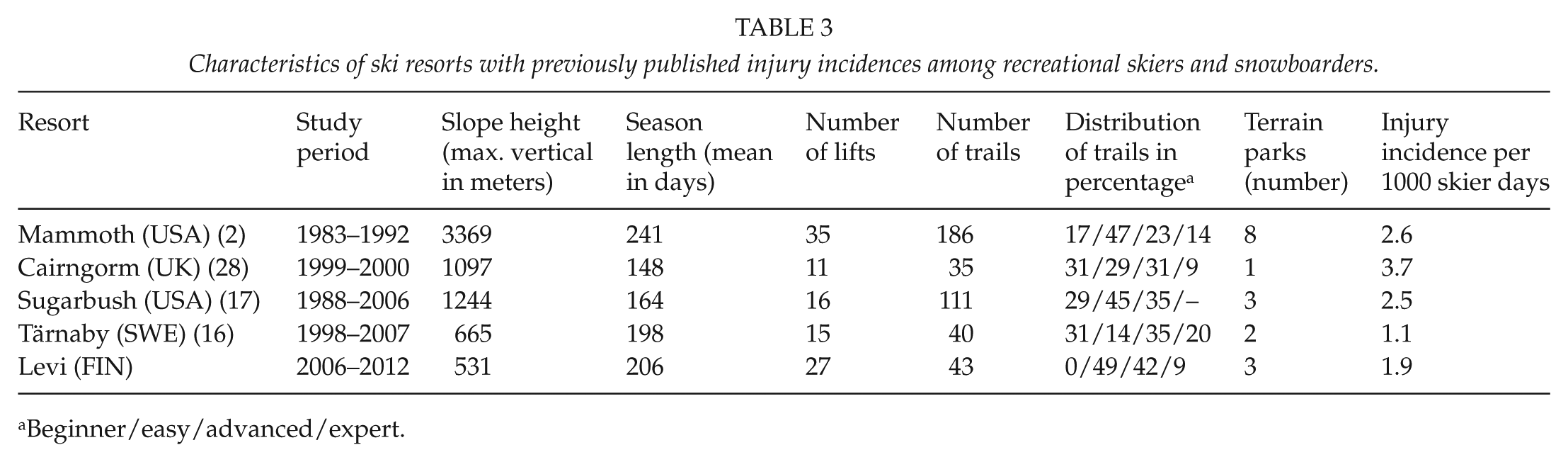
Beginner/easy/advanced/expert.
There have been several studies indicating an increased propensity for upper extremity injuries in snowboarding (17–21). In this study, it was also found that snowboarders were more likely to sustain upper extremity injuries when compared to skiers. The high number of injuries in the upper limb, in particular fractures of the wrist, is alarming, suggesting that further prevention is needed. There is evidence that prevention using wrist guards is beneficial, thus more information is needed on preventive measures among the snowboarders.
There is a difference in the distributions of lower extremity injuries between snowboarders and skiers, ankle and knee injuries being more common among snowboarders, whereas knee and tibial injuries predominate among skiers. In our study, the knee injuries were the most common type of injury among skiers, and snowboarders sustained fewer lower limb injuries than skiers. Similar results have been found in earlier studies (17–21). Even though the use of helmets has become more common during the last 15 years, the amount of head injuries among skiers and snowboarders is relatively high. Unfortunately, we were not able to determine the percentage of helmet use from our data due to missing information. However, there is convincing evidence that ski helmets reduce the risk of head injury (22). Helmets are not mandatory at Finnish ski resorts at present, but it would now be an opportune time to bring the compulsory use of helmets into a wider discussion.
Injuries taking place in terrain parks are more likely to be severe in nature and more likely require an ambulance transfer. Similar results have been found in earlier studies (23–25). Designing safer terrain parks and jumps is, however, challenging. We conclude in general that proper terrain park design with safety nets, signs, and adequate grooming of the jumps and landings reduces the risk of injuries. To avoid injuries, especially colliding injuries, safety should be properly underpinned in slope design. Highly visible signs asking skiers to slow down should be posted at places where two or more slopes merge into one. It is also important to avoid narrow passages in a slope and provide easier bypasses for beginners at the steeper parts of the slopes. It is reported that wider slopes reduce injuries (13, 26, 27), which should be taken into consideration when planning and designing ski trails. Adequate safety nets and protective gear should be placed on slopes to avoid collision with immovable objects.
The major shortage of this study is the inability to differentiate between skiers and snowboarders and males and females. The dedicated incidences of skiers and snowboarders could not be analyzed separately by using the present method. We could only present the overall total injury incidence for both groups. Also, it is likely that all injuries were not included in the data, since some of the less injured patients may have not contacted the ski resort emergency system but have sought for medical help after returning home. This was not obviously the case with the severe injuries which needed acute attention at the ski resort. We neither contacted the injured patients nor had an access to their medical post-injury data. Thus, we were not able to gain the final diagnosis of the injuries but had to use the primary triage diagnosis made by the ski resort emergency personnel.
We conclude that alpine skiing and snowboarding are related to a relatively high risk of injury. Fortunately, severe life-threatening injuries in these sports are infrequent. A continuous and systematic review of injuries is needed to monitor the effects of changes made in terms of the safety measures.
Footnotes
Acknowledgements
We thank Levi Ski Resort Emergency Management Services for the co-operation and all the help provided to conduct this study. The access to provided data is highly appreciated.
Declaration of Conflicting Interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.