
Abstract
Background and Aims:
Computed tomography angiography has become central to the diagnostic algorithm for penetrating neck injury, but despite its widespread use the literature to support this adoption is limited. We reviewed our experience with computed tomography angiography for the identification of vascular trauma in hemodynamically stable patients with penetrating neck injury at a major trauma center in South Africa.
Materials and Methods:
A prospectively kept trauma registry capturing data in real time was retrospectively reviewed. All patients with penetrating neck injury investigated with computed tomography angiography as the initial vascular investigation during a 47-month period were included.
Results:
A total of 380 patients were included. Indications for computed tomography angiography were as follows: hard signs (13), soft signs (201), no signs but proximity/zone I or III wounds (141), and undefined signs of vascular injury (25). Of the 380 scans, 7 (1.8%) were indeterminate, 299 (78.7%) negative, and 74 (19.5%) positive for a vascular injury (54 arterial and 20 isolated venous injury). Eight were false positive and 4 false negative. The sensitivity, specificity, positive, and negative predictive values for detecting arterial injury were 93.9%, 97.5%, 85.2%, and 99.1%, respectively. Overall, the yield for demonstrating “true arterial injury” was 12.1% (46/380); hard signs: 76.9% (10/13), soft signs: 16.4% (33/201), and no signs: 2.1% (3/141) which all were secondary to gunshot wounds). Only 8.4% (32/380) required intervention for arterial injury and none for isolated venous injury (hard signs: 62.0%, soft signs: 11.4%, and no signs: 0.7%). No serious complications resulted from computed tomography angiography.
Conclusion:
Computed tomography angiography is a safe and effective imaging modality for the investigation of vascular trauma post penetrating neck injury. Asymptomatic patients with stab wounds do not need to be imaged regardless of proximity concerns. Symptomatic stable patients including a subgroup with hard signs should be imaged rather than explored. Computed tomography angiography provides an interventional road map and can identify injuries amenable to endovascular or conservative management.
Keywords
Introduction
The evaluation of hemodynamically stable patients with penetrating neck injury (PNI) has evolved significantly (1–23). Multidetector computed tomography (MDCT) technology has changed the contemporary approach to the evaluation of PNI (11–22), and computed tomography angiography (CTA) has over the last decade become central to the diagnostic algorithms in most trauma centers (11). Despite CTA’s current widespread use for the assessment of PNI, the literature to support this adoption is still rudimentary as depicted in Table 1 (11–22). Although the management of trauma in South Africa has historically been heavily based on a philosophy of selective conservatism guided by clinical assessment, the common availability of CTA today has also resulted in it being increasingly used to evaluate patients with PNI (6–9, 23). The objective of this study was to review the effectiveness and yield of CTA in identifying vascular injuries and its influence in management of patients with PNI in a South African trauma service.
Summary of the literature on the use of CTA for the detection of vascular trauma in PNI.
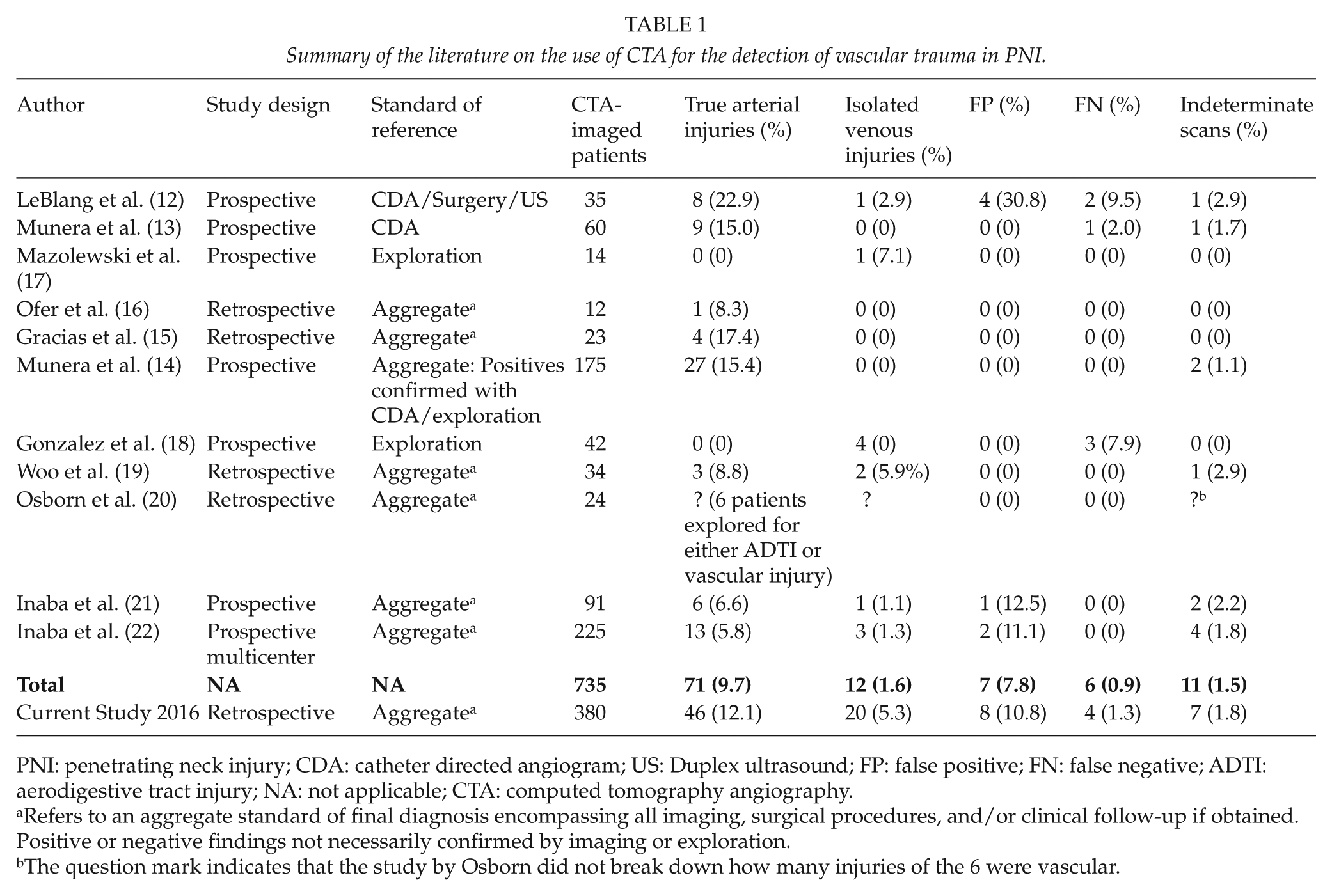
PNI: penetrating neck injury; CDA: catheter directed angiogram; US: Duplex ultrasound; FP: false positive; FN: false negative; ADTI: aerodigestive tract injury; NA: not applicable; CTA: computed tomography angiography.
Refers to an aggregate standard of final diagnosis encompassing all imaging, surgical procedures, and/or clinical follow-up if obtained. Positive or negative findings not necessarily confirmed by imaging or exploration.
The question mark indicates that the study by Osborn did not break down how many injuries of the 6 were vascular.
Materials and Methods
Clinical setting
This study was undertaken at the Pietermaritzburg Metropolitan Trauma Service (PMTS), Pietermaritzburg, South Africa. A retrospective review of a prospectively maintained regional trauma registry was conducted over a 4-year period from January 2011 to December 2014. The trauma registry, which is a hybrid electronic medical registry, captures demographic and clinical data in real time on all admitted trauma patients and is managed by designated trauma consultants in the PMTS (24). The Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal granted ethics approval for this study (Reference number: BE 207/09). The PMTS provides definitive trauma care to the city of Pietermaritzburg and the western part of the KwaZulu-Natal province. It serves as the only trauma referral service for 19 district hospitals, with a total catchment population of over three million people.
Patient Selection
Searching the trauma registry for the keywords “penetrating mechanism of injury,” “neck injuries,” and “investigation with CTA” identified patients for the study. Only hemodynamically stable patients with PNI investigated with CTA, as the initial vascular investigation, were eligible for inclusion. Data pertaining to demographics, zone of injury, mechanism of injury, injury severity score (ISS), clinical signs of vascular injury, the presence of vascular injury, imaging, intervention, and outcome were retrieved and evaluated. CTA scans and/or associated radiological reports were reviewed. All CTA scans performed at our institution are routinely reviewed by both the duty-attending surgeons and duty radiologist and equivocal findings customarily discussed at weekly multidisciplinary conferences. Findings at exploration, formal invasive catheter direct angiogram (CDA), and follow-up when obtained were used as an aggregate standard of reference to establish the effectiveness of CTA (false-positive and false-negative CTA studies, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV)). To determine the indications for the use of CTA in PNI, the yield of CTA in detecting a vascular injury was correlated with clinical signs of vascular injury on presentation, mechanism of injury, neck zones, and the subsequent clinical management.
CTA Protocol at PMTS
Hemodynamically unstable patients with self-evident hard signs of vascular injury (exsanguinating hemorrhage or rapidly expanding/pulsatile neck hematoma) are subjected to mandatory exploration. Hemodynamically stable patients, including patients in whom a threatened airway has been secured, are managed selectively. Mechanism of injury and physical examination are used to determine the need for further radiological investigation. Patients with PNI secondary to gunshot wounds (GSW) undergo mandatory CTA, whereas patients with injury due to stab wounds (SW) are investigated selectively depending on the presence or absence of clinical signs of vascular injury. All stable patients with hard signs (bruit or thrill, central neurologic deficit corresponding to the side of the injury, and absent pulse on the injured side) and stable patients with soft signs (history of severe bleeding or hypotension, small–moderate non-expanding/pulsatile hematoma, deficit of anatomically related nerve, on-going venous ooze, hemothorax (>500 mL), pulse discrepancy, systolic blood pressure discrepancy (>20 mmHg), widened mediastinum on chest X-ray (>8 cm at T4 on supine film) should undergo CTA. At the time of the study, imaging was also often done for asymptomatic patients, at the attending surgeon’s discretion, due to proximity concerns alone or involvement of zone I or III. CTA images are obtained by the use of two 64 slice MDCT units (Toshiba and Siemens), acquiring transverse sections of 0.6 mm thickness, from the base of the skull to the aortic arch, reconstructed to section thicknesses of 2–3 mm. The indications for CDA in our trauma service are now limited to CTA studies with equivocal findings, obscuring scatter from metallic foreign bodies (FBs) when compromising CTA interpretation, and finally for its still current advantage over CTA studies—cases amenable to endovascular therapy.
Results
Indications for CTA
A total of 383 out of 510 patients with PNI were identified as having undergone CTA, but 3 of these were later excluded from the study, as CTA had not been the initial vascular investigation. In total, 380 patients were eligible for inclusion in the study. The majority of patients were male (342) with a mean age of 29.6 years (range: 8–78 years) and a median ISS of 9 (interquartile range (IQR): 14–4). All patients were hemodynamically stable, but 14 required an emergency airway. The mechanism of injury was primarily SW (SW: 328, GSW: 52). Using Roon’s classification (2) of the neck zones, the injuries were distributed as follows: zone I (160), zone II (93), zone III (30), multiple zones (59), posterior triangle (36), and undefined injuries (2). The clinical indications for imaging were as follows: stable patients with hard signs (13, including 3 GSW), soft signs (201, including 29 GSW), and no signs (141, including 17 GSW but also 124 patients with SW imaged due to proximity/at surgeon’s discretion) and 25 with undefined signs of vascular injury.
CTA Findings and Management of Vascular Injury
Out of 380 scanned patients, 299 (78.7%) CTA studies were negative and 7 (1.8%) indeterminate. Only 74 (19.5%) scans were positive for a vascular injury with 54 (14.2%) revealing arterial injury and another 20 (5.3%) demonstrating an isolated venous injury (IVI). In all, 90 vascular injuries (33 venous and 57 arterial) were identified on the 74 positive CTA studies. For venous injuries, the most common finding on CTA was an occlusion of the vessel suggestive of a thrombus (51.5%), whereas for arterial injuries the most common finding was a pseudoaneurysm (38.6%). Sub-analysis of our data for arterial injury specifically for GSWs revealed pseudoaneurysms as being the least common finding (15.4%) and vessel occlusions (53.8%) and wall irregularity (30.8%) suggestive of intimal injuries to be the dominant presentation. The distribution of injured vessels and their radiological appearance and management is depicted in Table 2.
The distribution, radiological description, and management of 90 CTA identified vascular injuries. a
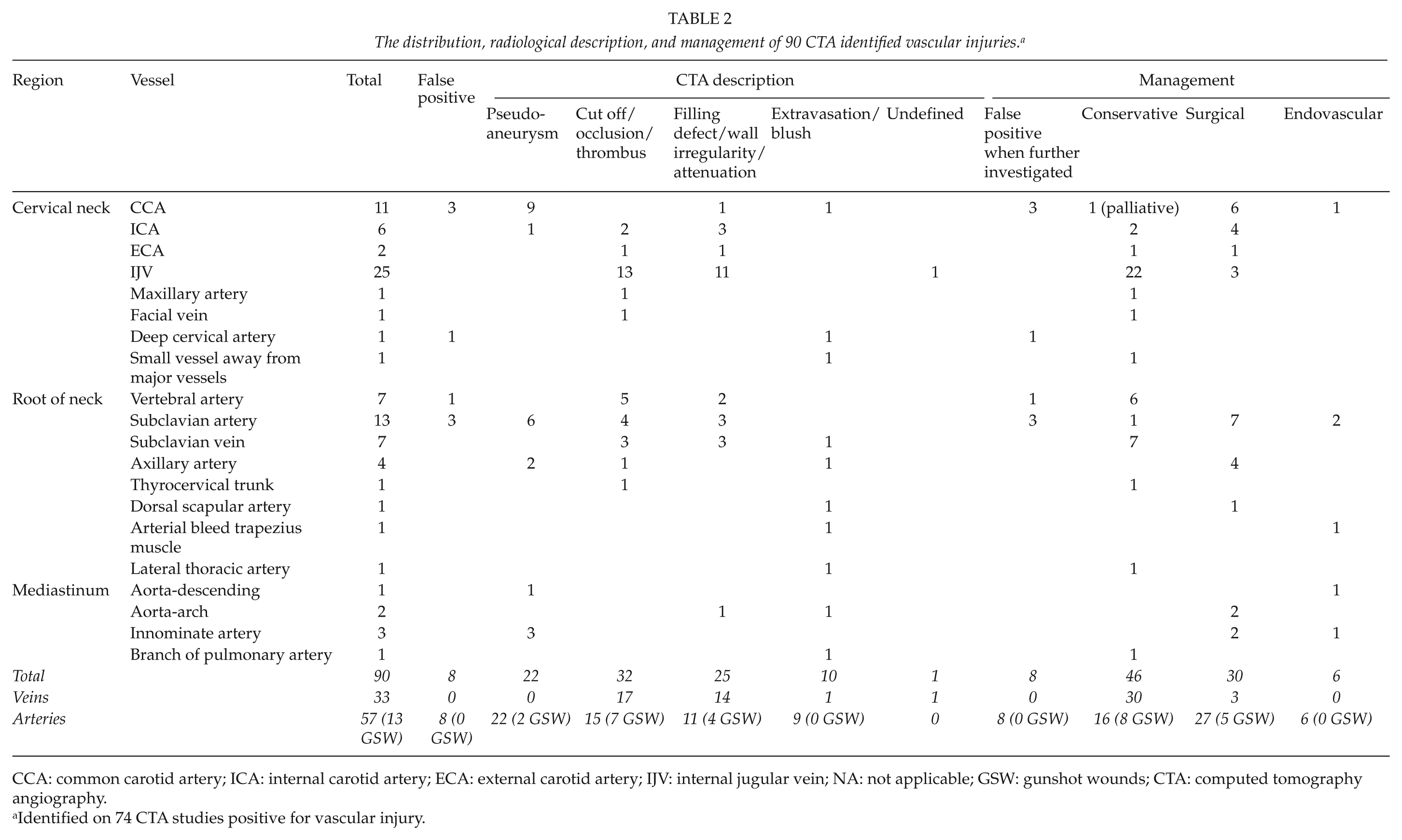
CCA: common carotid artery; ICA: internal carotid artery; ECA: external carotid artery; IJV: internal jugular vein; NA: not applicable; GSW: gunshot wounds; CTA: computed tomography angiography.
Identified on 74 CTA studies positive for vascular injury.
Indeterminate CTAs
Out of 380 CTA studies, 7 (1.8%) were indeterminate and this was primarily due to scatter from metallic FBs. Only a total of 33 patients had retained FBs visible on CTA, but in 6 (18.2%) of these patients, the retained FB made it difficult to exclude a vascular injury. This necessitated further imaging in four patients. For one of these, an injury to the internal carotid artery (ICA) was demonstrated with CDA and managed operatively. For another, CDA was suggestive of an injury to the subclavian artery (SCA). This patient subsequently underwent a negative exploration and was found to have external compression of the artery by a fragment of the first rib. CDA clearly excluded injury in a third patient. The remaining patient with an indeterminate scan was found to have an ectatic thyro-cervical trunk on CDA.
Effectiveness and Yield of CTA
A total of eight CTAs were falsely positive for a vascular injury. This constituted 8 out of a total of 74 (10.8%) positive CTA studies for vascular injury in general but 8 out of 54 (14.8%) CTA studies positive for arterial injury specifically. These false-positive CTA scans were related to subtle changes in major arteries and were confirmed to be false positive by CDA in seven patients and by a repeat CTA study in one patient.
CTA was found to be false negative for vascular injury in four patients. This constituted 4 out of a total of 299 (1.3%) negative CTA studies for vascular injury in general and 3 out of 319 (0.9%) for arterial injury specifically. These four missed injuries represented three delayed presentations of pseudoaneurysms of minor arterial branches and one a non-bleeding injury to the internal jugular vein (IJV) injury, which was incidentally discovered during exploring for a concomitant esophageal injury. Fig. 1 gives a study overview of the above results. Excluding the seven indeterminate CTAs, the sensitivity, specificity, PPV, and NPV of CTA in detecting a vascular injury in general was 94.2% (66/(66 + 4)), 97.4% (295/(295 + 8)), 89.2% (66/(66 + 8)), and 98.7% (295/(295 + 4)). Excluding also IVI, the sensitivity, specificity, PPV, and NPV of CTA in detecting an arterial injury was 93.9% (46/(46 + 3)), 97.5% (316/(316 + 8)), 85.2% (46/(46 + 8)), and 99.1% (316/(316 + 3)).
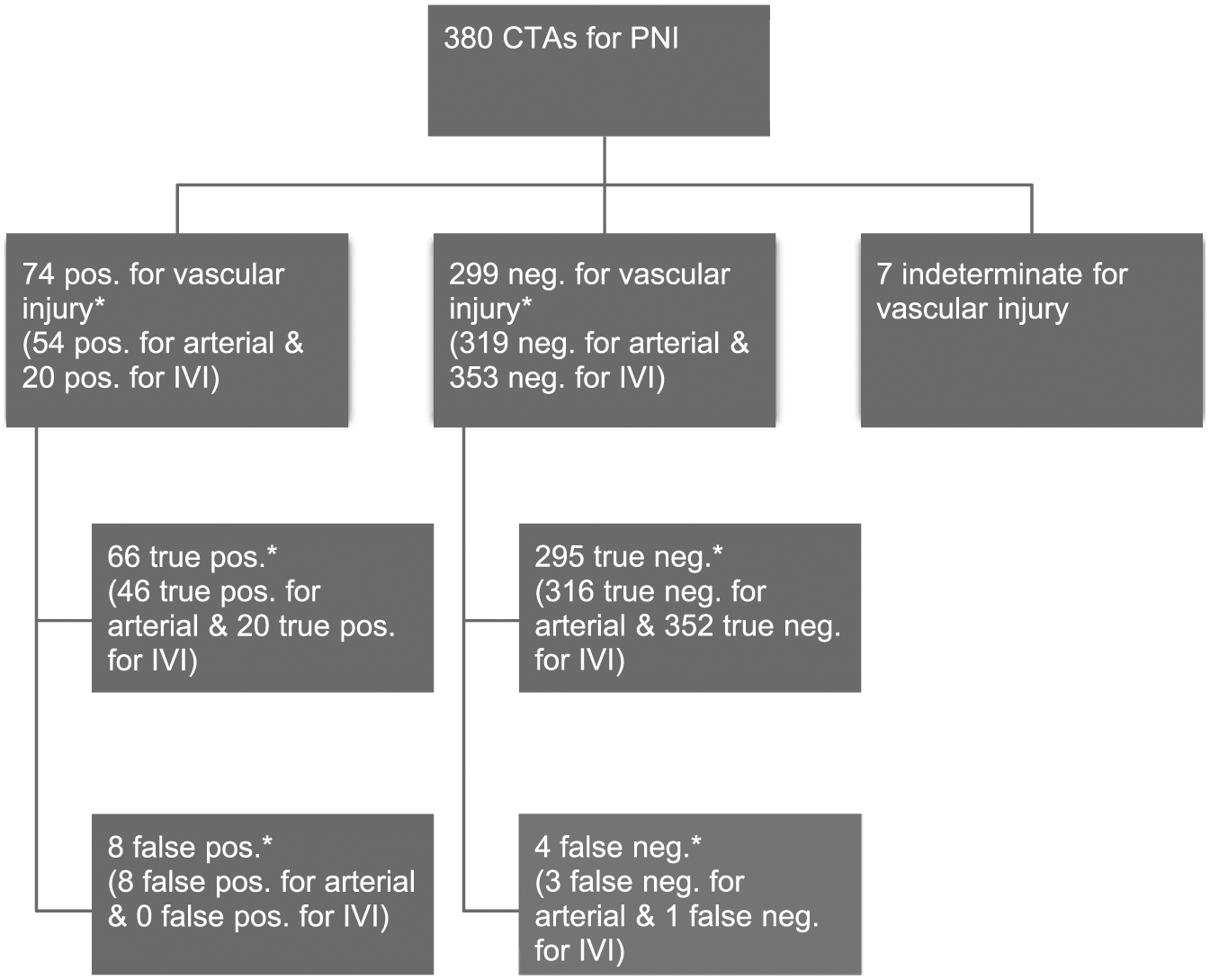
Study overview.
In total, 20% (74/380) of CTAs were positive for vascular injury. However, when adjusted for false-positive findings (8) and CTAs positive for IVI (20), none of which mandated surgery, the yield of CTA for demonstrating a “true arterial injury” was only 12% ((74 − 8 − 20)/(380)).
Sub-analysis of this yield according to zones of the neck was as follows: zone I: 13% ((34 − 3 − 10)/(160)), zone II: 10% ((14 − 2 − 3)/(93)), zone III: 13% ((6 − 1 − 1/30)), the posterior triangle: 14% ((9 − 2 − 2)/(36)), and patients with injuries to multiple zones: 12% ((11 − 0 − 4)/(59)). When analyzed according to the mechanism of injury, this yield was for patients with GSW 19% ((12 − 0 − 2)/52)) which was almost twice as high as that for patients with SW of 11% ((62–8–18)/328). Analyzed according to clinical signs, this yield was for patients with hard signs and soft signs and the asymptomatic patient: 77% (10/13), 16% (33/201), and 2% (3/141), respectively. No patients required exploration for IVI alone. However, the need for intervention due to arterial injury was for patients with hard signs and soft signs and the asymptomatic patient: 62% (8/13), 11% (23/201), and less than 1% (1/141). Table 3 demonstrates the yield of CTA according to the clinical signs at presentation and the management of true arterial injuries.
Yield of CTA for vascular injury according to signs of vascular injury and management of arterial injuries.
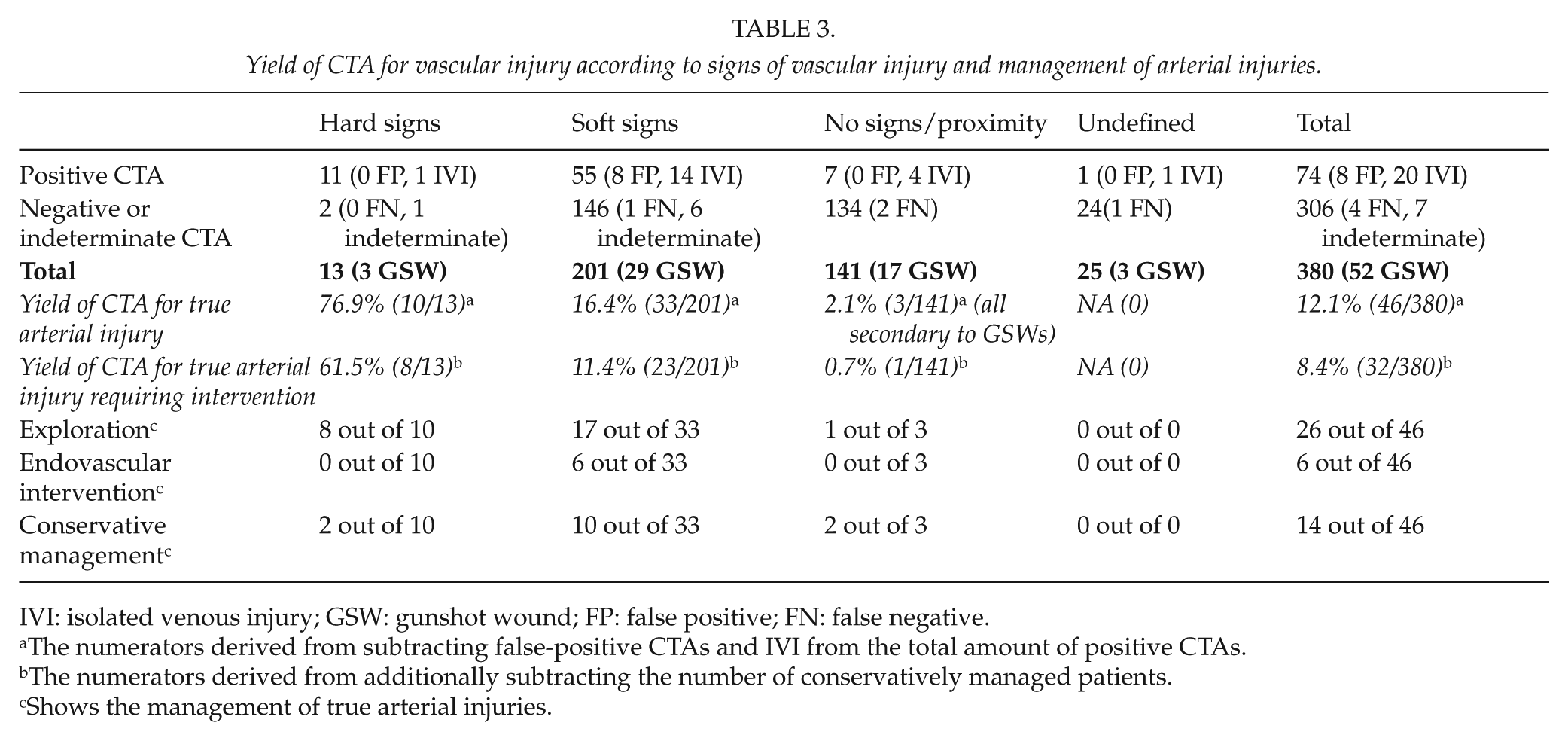
IVI: isolated venous injury; GSW: gunshot wound; FP: false positive; FN: false negative.
The numerators derived from subtracting false-positive CTAs and IVI from the total amount of positive CTAs.
The numerators derived from additionally subtracting the number of conservatively managed patients.
Shows the management of true arterial injuries.
Outcomes
Out of 13 CTAs performed for patients with stable hard signs of injury, 11 (84.6%) studies were positive for arterial (10) or venous (1) injury. Most of these patients had central neurological deficits or an absent pulse on the injured side and one a bruit. The majority had zone I injuries or injuries to multiple zones and only one a zone II injury. Only 8 of the 13 (61.5%) patients with stable hard signs required exploration for vascular injury. No patients with hard signs and vascular injury died or complicated as a result of pre-operative imaging.
Imaging of asymptomatic patients, done due to proximity at the “surgeons discretion,” revealed arterial (3) or venous (4) injury in only 5% (7/141). The four IVI were all managed conservatively. The arterial injuries were all secondary to GSWs, and in two cases, the trajectory was trans-cervical. As only 17 of the 141 asymptomatic patients sustained injury secondary to GSW, the yield of CTA for asymptomatic patients with GSW to the neck was 18% (3/17) in this subgroup. Two VA and one ICA injuries were demonstrated. None had pseudoaneurysms or extravasation of contrast. Only the patient with the ICA injury, who also had a concomitant abdominal GSW, proceeded to the operating room for exploration, giving a negligible clinical yield of less than 1% (1/141) for imaging asymptomatic patients in our study. No CTA-imaged patients underwent a negative or non-therapeutic exploration. Furthermore, no serious complication resulted from imaging with CTA.
Discussion
CTA for PNI is a safe imaging modality and it accurately identifies arterial injury. We found the rate of false-negative investigations to be very low (0.9%) although CTA was false positive for arterial injury in 8 out of 54 (14.8%) patients. This was due to subtle changes in major arteries and required further imaging. Another limitation of CTA for PNI was the presence of metallic FBs, which primarily were bullet fragments. Even though only 6 (1.6%) of all scans were indeterminate due to FBs, this constituted 18% (6/33) of all patients with FBs. Regardless of these shortcomings, we found CTA to be a very effective imaging modality for PNI, reflected by a 0% negative/non-therapeutic exploration rate. These results support previous reports suggesting that CTA for PNI reduces the rate of negative explorations (19, 20).
For a long time, mandatory exploration of all PNI breaching the platysma was considered the norm due to a prevailing concern over the reliability of physical exam. This, however, resulted in a high rate of negative exploration (1) and was abandoned (2–11). Most authors now follow a strategy of selective conservatism. Mandatory exploration is reserved for patients with overt signs of a vascular injury and all other patients are selectively investigated based on a combination of so-called soft signs and the site of the external wound (2–9, 11). Until a decade ago, the imaging modality of choice to assess the vascular system following PNI was a formal CDA (9, 10). This technique was reliable and accurate, but was associated with a small but significant incidence of potentially serious complications (25).
CTA has now replaced CDA as the first choice for imaging in patients with PNI (11, 22). It offers a non-invasive alternative to CDA. However, the literature to support this approach is scarce as demonstrated in Table 1 (12–22). Only a few studies have examined the effectiveness of CTA and analyzed the indications for its use for PNI. The majority of these studies have been small and in total have assessed less than a 100 CTA images positive for vascular injury. Our data reinforce previous results from the literature and confirm that CTA is an excellent investigation for PNI with a sensitivity, specificity, PPV, and NPV approaching 94%, 98%, 85%, and 99%, respectively, for the detection of arterial injury.
Whether CTA for PNI, despite its definite false-positive rate, might be a beneficial screening modality for patients with PNI in low-volume trauma centers and general surgical units dealing with the occasional PNI remains unanswered from this study. Our study confirms that in high-volume trauma centers like ours, nothing is gained by imaging asymptomatic patients unless injured by a GSW. In such settings, the indication for CTA can be guided by clinical assessment.
Regardless of clinical signs, the yield of CTA for PNI secondary to GSWs in our study was almost twice as high as that for SW (19% vs 11%). In addition, it is clinically difficult to assess a GSW of the neck (10). In light of this, we advocate mandatory imaging of all GSWs to the neck. The issue of which stable patients require imaging following a stab wound (SW) of the neck is controversial. Most authors now agree that imaging of asymptomatic patients without signs of vascular injury has a low yield (3–5, 8, 9, 11, 22). Our data concur with these reports and show that patients who require vascular imaging can be identified by physical examination, irrespective of zone or proximity.
Although the presence of a hard sign is very suggestive of an injury, the presence of a soft sign only predicts an arterial injury in about 16% of patients. Furthermore, the presence of clinical signs does not reliably predict who will require treatment. Mandatory exploration of all stable patients with a hard sign of vascular injury will result in a significant rate of non-therapeutic exploration and may deny a subset of patients the option of conservative or endovascular management. Although 77% of patients with hard signs in our series had arterial injury, only 62% of patients with hard signs required exploration for arterial injury. Of the patients with a soft sign, 16% had an arterial injury, but only 11% required intervention of which 26% (6/23) were managed with endovascular techniques. Imaging with CTA of stable patients with clinical signs of vascular injury effectively identifies patients with vascular injuries and helps identify injuries amenable to endovascular or conservative management.
Venous injuries may present with hard signs but ultimately may not require any intervention. This was elegantly shown by the Cape Town group (26). They described the conservative management of venous injuries in unstable patients with PNI. After initial control of life-threatening bleeding was achieved by use of Foley Catheter Balloon Tamponade (FCBT), the authors went on to image these patients with CDA. They reserved exploration for patients with confirmed arterial injuries on CDA or for those in which FCBT was unsuccessful. Our own data suggest that venous injuries identified in stable patients with PNI can for the most part be treated conservatively.
Our suggested approach to PNI in the CTA era is depicted in Fig. 2. For stable patients with a GSW to the neck imaging is essential regardless of clinical findings. For stable patients who sustain a stab wound, all those with a soft sign should be imaged but asymptomatic patients can be observed with serial neck examination. Although unstable patients with self-evident hard signs of vascular injury must be taken directly to the operating room, stable patients with hard signs should be imaged regardless of the site of the external wound. One-third of these patients may not require vascular exploration. In addition, the zone of the external wound often does not correlate with the zone of the visceral injury (27) and accurate delineation of the injury with CTA facilitates surgical planning.
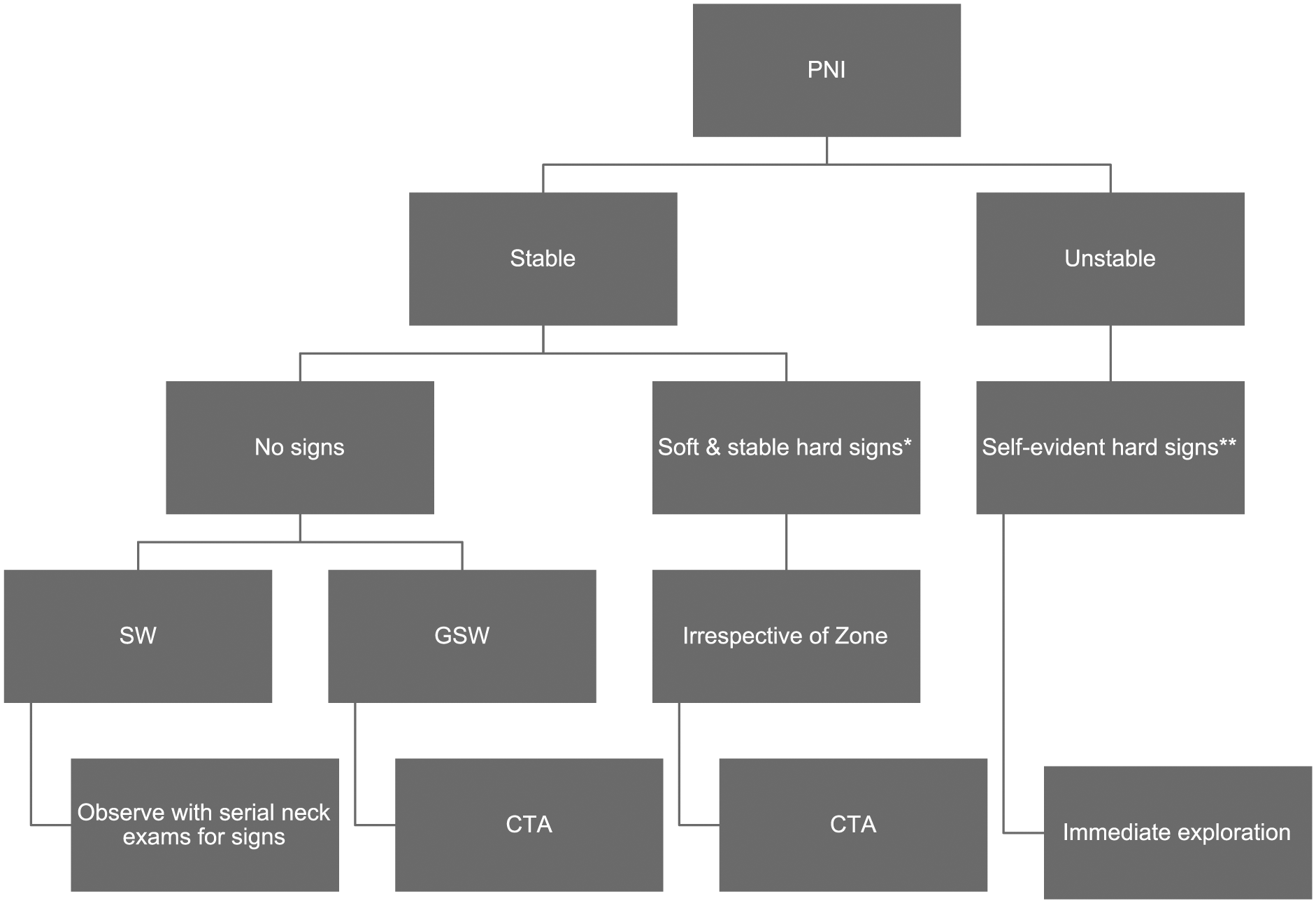
Approach to PNI in the CTA era.
Conclusion
CTA for PNI is safe and accurately identifies arterial injury following PNI. The rate of false-negative investigation is very low although there is a definite incidence of false-positive studies. Patients with GSW to the neck need imaging but SW should be imaged selectively. Asymptomatic patients can be observed and do not need imaging for proximity concerns. CTA is useful for all symptomatic but hemodynamically stable patients, including a subgroup with stable hard signs. In this subgroup, only two-thirds will ultimately require vascular intervention.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest. The manuscript is not under review elsewhere and has not previously been published. The abstract has, however, been presented at the American College of Surgeons, Committee on Trauma Annual Meeting on 2 March 2017 at National Harbor, MD, USA.
Ethical Approval
The authors have ethics approval to maintain their database from the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal (Reference number: BE 207/09).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.