
Abstract
Background and Aims:
Mild traumatic brain injury is a common presentation to Emergency Departments. Early identification of patients with cognitive deficits and provision of discharge advice are important. The Abbreviated Westmead Post-traumatic Amnesia Scale provides an early and efficient assessment of post-traumatic amnesia for patients with mild traumatic brain injuries, compared with the previously used assessment, the Modified Oxford Post-traumatic Scale.
Material and Methods:
This retrospective cohort study reviewed 270 patients with mild traumatic brain injury assessed for post-traumatic amnesia over a 2-year period between February 2011 and February 2013. It identified those assessed with Abbreviated Westmead Post-traumatic Amnesia Scale versus Modified Oxford Post-traumatic Scale, the outcomes of these post-traumatic amnesia assessments, the hospital length of stay for patients, and their readmission rates.
Results:
The Abbreviated Westmead Post-traumatic Amnesia Scale was used in 91% of patient cases (and the Modified Oxford Post-traumatic Scale in 7%), and of those assessed with the Abbreviated Westmead Post-traumatic Amnesia Scale, 94% cleared post-traumatic amnesia testing within 4 h. Of those assessed with the Abbreviated Westmead Post-traumatic Amnesia Scale, 56% had a shorter length of stay than had they been assessed with the Modified Oxford Post-traumatic Scale, resulting in 295 bed-days saved. Verbal and written discharge advice was provided to those assessed for post-traumatic amnesia to assist their recovery. In all, 1% of patients were readmitted for monitoring of mild post-concussion symptoms.
Conclusion:
The Abbreviated Westmead Post-traumatic Amnesia Scale provides an effective and timely assessment of post-traumatic amnesia for patients presenting to the Emergency Department with mild traumatic brain injury compared with the previously used assessment tool. It helps identify patients with cognitive impairment and the need for admission and further investigation, resulting in appropriate access to care. It also results in a decreased length of stay and decreased hospital admissions, with subsequent cost savings to the hospital.
Introduction
Mild traumatic brain injury (TBI) is a common presentation in Emergency Departments (EDs). Mild TBI following closed head injury is estimated to comprise 70%–90% of all hospital-treated adult TBIs (1). Even mild TBI can cause significant morbidity (2–4). Cognitive deficits following TBI can include reduced memory for new information, slower information processing, and behavioral changes (5–10). Early identification of post-traumatic amnesia (PTA) and assessment of its duration assist in determining the severity of TBI and consequent management and follow-up (7, 10–13).
At Liverpool Hospital, two standardized PTA scales are currently used. The Modified Oxford Post-traumatic Scale (MOPTAS) was the only scale in use up until 2010. The MOPTAS was designed to measure PTA in patients with any severity of TBI. It consists of orientation questions and a memory test and requires hospital admission for daily testing for a minimum of 4 days. Clearance is reached after scoring 12/12 over three consecutive days following provision of information to recall. Therefore, patients with mild TBI were admitted for a minimum of 4 days for PTA testing or discharged without any formal assessment of PTA.
The Abbreviated Westmead Post-traumatic Amnesia Scale (A-WPTAS), developed in 2007, assesses PTA in patients with mild TBI (14). A-WPTAS consists of a Glasgow Coma Scale (GCS) score plus recalling three pictures. This test is conducted within 24 h of injury and consists of hourly testing from 1 h to a maximum of 4 h, depending on when the patient clears PTA. Clearance is reached by scoring 18/18. If a score of 18/18 is not achieved in the 4 h, then MOPTAS testing is commenced.
In 2008, the Motor Accidents Authority recommended A-WPTAS for assessment in mild TBI (15). At Liverpool Hospital, A-WPTAS was piloted at the end of 2010 on the neurosurgery ward. It was identified that using A-WPTAS in other wards and the ED could assist early clinical assessment of patients with mild TBI, identify the need for appropriate education and follow-up, and potentially minimize hospital admissions and length of stay (16). Consequently, a retrospective study was conducted over a 2-year period to examine the impact of the introduction of A-WPTAS on patient length of stay and readmission rates.
Material and Methods
In this retrospective cohort study, all patients with mild TBI were selected from the Occupational Therapy data register. This register contains all patients who had been assessed by occupational therapists in the ED or on the ward at Liverpool Hospital in New South Wales. Included were those patients with mild TBI who required PTA testing between February 2011 and February 2013. Methods used for PTA testing were the MOPTAS and the A-WPTAS. Patients with mild TBI who were assessed for PTA by nursing staff were not included, as nursing staff conducted relatively few PTA scales and held no data register of them.
Mild TBI was defined as an initial GCS of 13–15 on the scene or in the ED with impact to the head resulting in confusion, disorientation, antegrade or retrograde amnesia, or brief loss of consciousness within 24 h post injury. All patients who presented to the ED within the first 24 h post injury were selected for A-WPTAS. Those who presented after this period and those who did not clear A-WPTAS in 4 h progressed to MOPTAS. Patients under the influence of alcohol were not excluded; based on multidisciplinary clinical judgment, they could undertake the A-WPTAS or proceed to the MOPTAS. To clear A-WPTAS, a maximum score of 18 had to be obtained within the first three attempts of testing.
The following data were extracted from the Occupational Therapy data register: age, gender, trauma mechanism, loss of consciousness, GCS, Injury Severity Score, length of stay, and readmissions. The discharge summaries, electronic medical record, and Trauma Registry were used to confirm this information. If there were inconsistencies, a chart review was performed. In addition, the number of attempts and clearance from A-WPTAS and progress to MOPTAS and clearance were registered.
All statistical analyses were performed with SPSS for Windows, version 21.0.0. For this retrospective study, the South Western Sydney Local Health District Human Research Ethics Committee granted ethical approval. This study follows the recommendation of the Strengthening the Reporting of OBservational studies in Epidemiology (STROBE) Statement.
Results
In the period from February 2011 to February 2013 at Liverpool Hospital, 963 patients were admitted with brain injury, of which 80% are anticipated to have had mild TBI (17). In all, 270 patients with mild TBI were reviewed by an occupational therapist and included in the study. Of these patients, 189 were male (70%) and 81 female (30%) with a median age of 30 years (range = 12–89 years). The most common injury mechanisms were motor vehicle crashes (n = 85), falls from height (n = 69), assault (n = 47), and motorcycle crashes (n = 37) (Fig. 1). For 160 patients (59%), there was a reported loss of consciousness at the scene. Median GCS in the ED was 15 (range = 13–15). In 241 of 270 patients (89%), a brain computed tomography (CT) was completed to evaluate the injury (Table 1). No patients underwent a brain CT or magnetic resonance imaging (MRI) because they did not clear A-WPTAS.
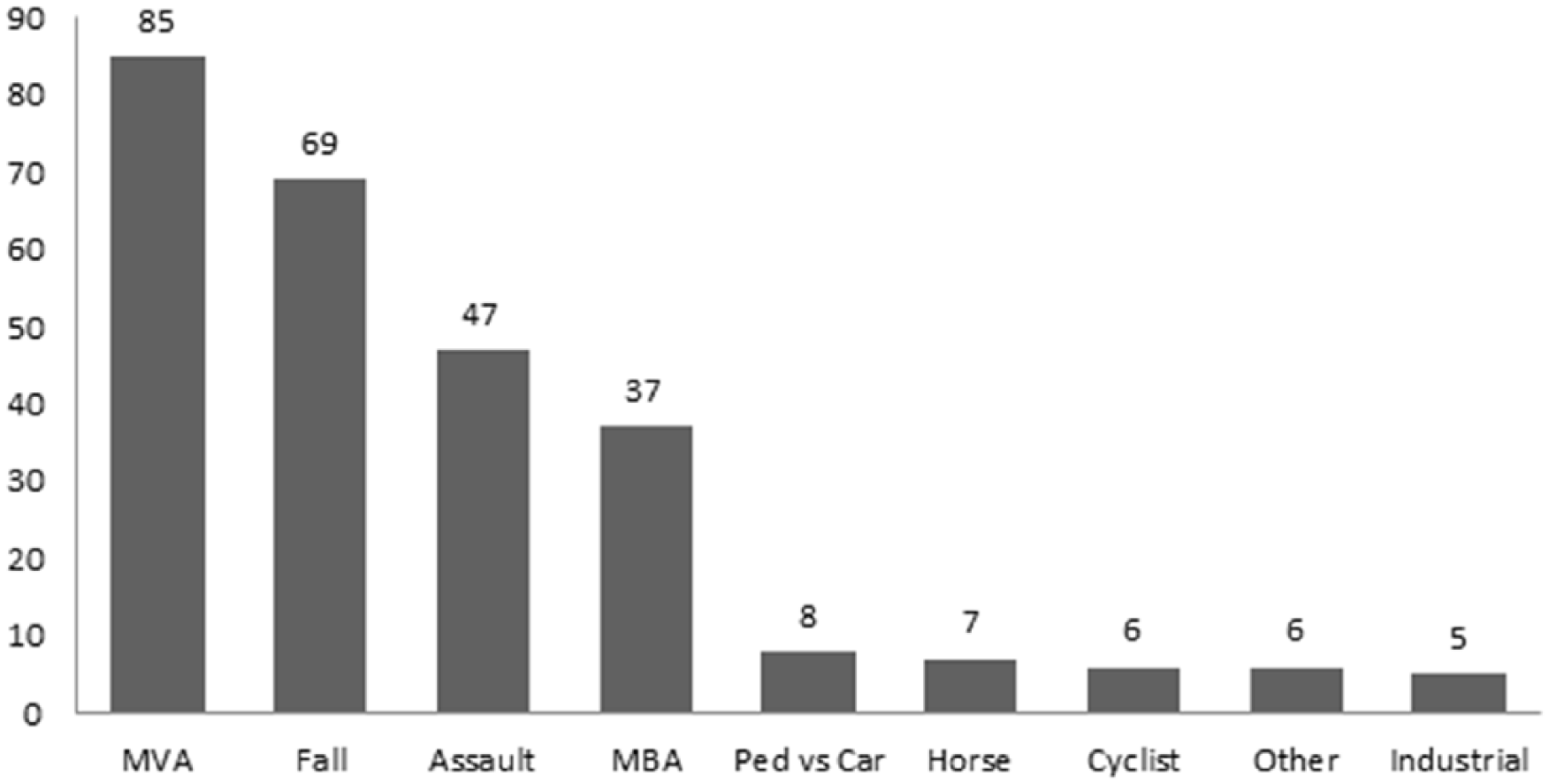
Mechanism of injury.
Baseline characteristics.
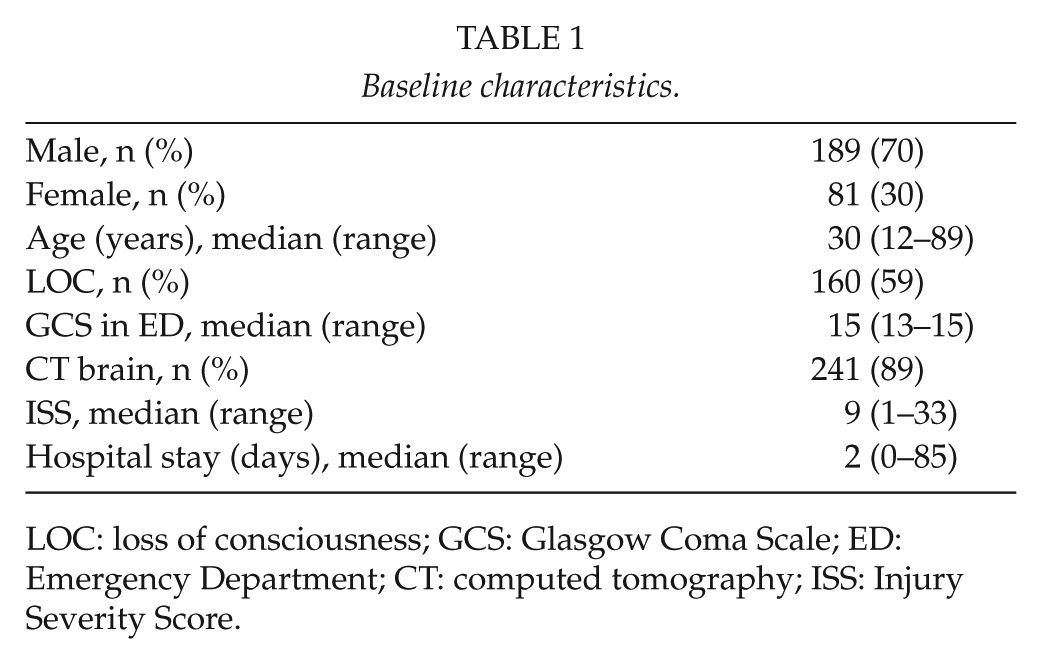
LOC: loss of consciousness; GCS: Glasgow Coma Scale; ED: Emergency Department; CT: computed tomography; ISS: Injury Severity Score.
A-WPTAS was commenced for 246 patients (91%), of which 231 cleared A-WPTAS (94%) within the first 4 h and 15 patients (6%) did not clear the A-WPTAS. Nine of these patients (4%) progressed to MOPTAS for the 4-day assessment of PTA, and six patients (2%) were discharged before assessment was completed. In all, 20 patients (7%) commenced MOPTAS immediately as they did not meet A-WPTAS criteria, as it was greater than 24 h from injury. Four patients (1%) received no formal PTA assessment as they were discharged prior to its commencement (Fig. 2). In 46 of the 231 patients (20%) who cleared the A-WPTAS, it was identified that assessment by an occupational therapist started later than 24 h post injury.
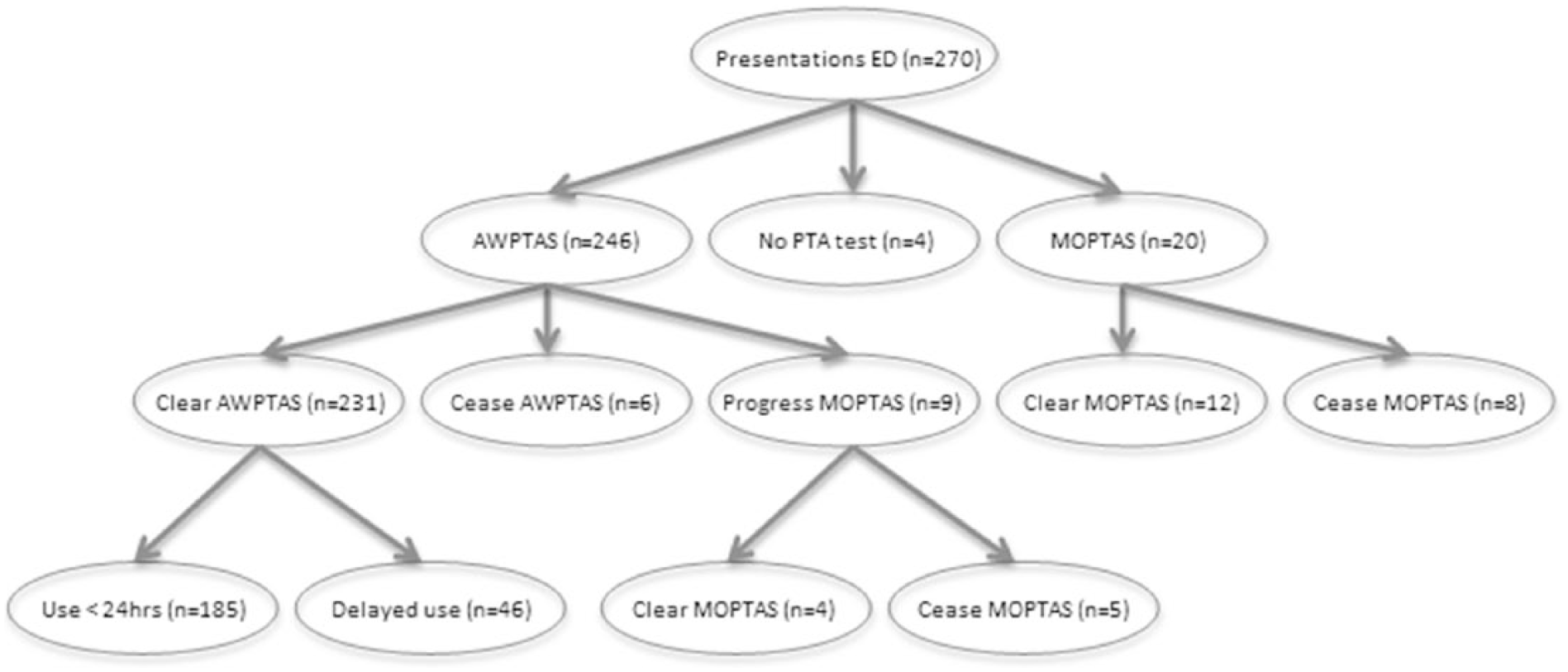
Post-traumatic amnesia testing after mild traumatic brain injury.
More than half of the patients (151 patients) had a shorter admission, as a result of using the A-WPTAS, than was previously required with the 4-day MOPTAS assessment. Of these patients, 40 (15%) had a 1-day hospital length of stay, 64 patients (24%) had a 2-day length of stay, and 47 patients (17%) had a 3-day length of stay.
Twelve patients represented to EDs within the local health district hospitals, six with symptoms related to TBI. All had been assessed and cleared A-WPTAS on their first presentation and had been provided follow-up information. Three were reviewed in ED for mild post-concussion symptoms and discharged. Three (1%) were readmitted with mild post-concussion symptoms, monitored for 2 days, and discharged.
Discussion
This retrospective study demonstrates that few patients presenting with isolated mild TBI assessed with the A-WPTAS required admission for ongoing PTA assessment using the MOPTAS. The previous “gold standard” of assessment (MOPTAS) for TBI required admission and 4 days of PTA testing. In this study, all patients clearing A-WPTAS and being otherwise medically cleared for discharge had a reduced length of stay compared with the previous 4-day hospital testing and received verbal and written discharge advice. The use of the A-WPTAS contributed to the overall assessment of patients with mild and isolated TBI and resulted in a reduced length of stay. This allows better access for those with more significant TBI and timely discharge, following assessment and investigations, for those with mild injuries.
Over a 2-year period at Liverpool Hospital, by using A-WPTAS instead of MOPTAS, 40 patients were discharged 3 days earlier (120 days), 64 patients were discharged 2 days earlier (124 days), and 47 patients were discharged 1 day earlier (47 days). This equates to 295 bed-days saved at a current cost of AUD$829 per bed-day (as per Liverpool Hospital, Finance Department), resulting in a total savings of AUD$244,555.
The retrospective nature of this study is a limitation, with only patients reviewed by an occupational therapist included. This increases the chance of selection bias. Following review of data from the Clinical Information Department regarding relevant diagnostic-related groups over the same period, it is estimated that one-third of presentations to the ED with mild TBI were referred to occupational therapy for PTA assessment. This may be related to availability of occupational therapists (cover 8 h of a 24-h period), some PTA scales being conducted by nursing staff, informal assessment being used and patients discharged, or other medical issues taking priority. Representations for patients in this study were captured through the district electronic medical records; therefore, presentations to general practitioners, medical specialists, or hospitals outside the district are unknown.
Conclusion
The A-WPTAS provides an effective and timely assessment of PTA in patients presenting to the ED with isolated and mild TBI. It helps determine the need for ongoing investigation of cognition, identifies the need for education and follow-up, and results in a reduced length of stay for patients with mild TBI resulting in greater bed availability and significant cost savings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.