
Abstract
Background and Aims:
Patients with acute or chronic wrist pain often undergo wrist arthroscopy for evaluation of chondral and ligamentous abnormalities. The purpose of this study was to compare findings of wrist arthroscopy with cone beam computed tomography arthrography and magnetic resonance arthrography.
Materials and Methods:
Altogether, 21 patients with wrist pain underwent cone beam computed tomography arthrography, magnetic resonance arthrography, and wrist arthroscopy. Chondral surfaces of the scaphoid, lunate, and radius facing the scaphoid and lunate were evaluated. The scapholunate ligament, the lunotriquetral ligament, and the triangular fibrocartilage complex were classified as either intact or torn. Sensitivity, specificity, positive and negative predictive values, and accuracy with 95% confidence intervals were assessed.
Results:
For chondral lesions (n = 10), cone beam computed tomography arthrograms showed slightly higher specificity than magnetic resonance arthrography. The sensitivity of cone beam computed tomography arthrography was also better for these lesions, except for those on the chondral surface of the lunate. For triangular fibrocartilage complex injuries (n = 9), cone beam computed tomography arthrography showed a better specificity and sensitivity than magnetic resonance arthrography. For ligamentous injuries (n = 6), cone beam computed tomography arthrograms were more sensitive, but less specific than magnetic resonance arthrography images. However, the number of lesions was very small and the 95% confidence intervals are overlapping.
Conclusion:
Cone beam computed tomography is an emerging imaging modality that offers several advantages over computed tomography and magnetic resonance imaging. Its usefulness particularly in ligamentous injuries should be further explored in a larger study. Cone beam computed tomography arthrography seems to offer similar sensitivity, specificity, and accuracy compared to magnetic resonance arthrography and therefore serves as a valuable option in evaluating patients with wrist pain.
Keywords
Introduction
Wrist pain is a common complaint among hand surgery patients. Due to the complex anatomy and biomechanics of the wrist, the cause of the pain may, however, be difficult to ascertain through clinical examination alone. Often, noninvasive diagnostic tools, such as radiographs and magnetic resonance imaging (MRI), are used in the evaluation of patients with wrist pain. Radiographs remain the first-line examination in acute trauma, as this imaging modality is the fastest and the radiation dose is the lowest.
MRI is useful in evaluating synovial-related diseases of the wrist and also shows bone marrow edema. Another benefit of MRI is its ability to detect occult ganglion cysts of the wrist. The resolution of MRI does not necessarily exclude chondral injuries, and therefore, magnetic resonance arthrography (MRA) is often performed for suspected abnormalities of chondral surfaces, ligaments, or triangular fibrocartilage complex (TFCC) of the wrist (1). Unfortunately, this examination is time-consuming and sometimes uncomfortable for the patient.
Cone beam computed tomography (CBCT) is a relatively new technology for diagnosing wrist pain. CBCT has proved useful in musculoskeletal (MSK) imaging (2) and assessment of wrist ligaments and radiocarpal cartilage (3). High-resolution images (4), easy installation (5), and low radiation doses (6, 7) are benefits associated with CBCT and reasons for its increasing popularity. A recent study also showed that in acute trauma, CBCT can reveal more fractures than conventional radiographs, and simple fractures seen in radiographs may be identified as complex with CBCT (8). However, radiographs remain the first-line examination in acute trauma. Also, radiographs are still superior to cross-sectional techniques in the detection of hardware complications such as plate fractures and screw breakage (7).
The reference standard in diagnosing wrist ligament tears and chondral lesions is wrist arthroscopy. Arthroscopy offers a precise understanding of the ligaments and chondral surfaces, and in addition to diagnosis, treatment can often be provided during arthroscopy. However, as an invasive procedure, arthroscopy includes the usual risks of surgery and anesthesia.
The purpose of this study was to compare findings of CBCT and MRA with arthroscopic findings of the wrist, with a special focus on chondral surfaces as well as ligamentous and TFCC injuries.
Materials and Methods
The patients included in this study received treatment for acute or chronic wrist pain at the Department of Hand Surgery, Helsinki University Central Hospital, Finland. Altogether, 53 consecutively enrolled patients were offered CBCT arthrography immediately prior to their routinely scheduled MRA. The indication for MRA was suspected ligament tear, TFCC tear, radiocarpal joint cartilage assessment, or distal radioulnar joint evaluation. Each participant provided his or her written informed consent. One patient declined to participate in the study. The hospital’s Ethics Committee approved the study protocol.
The remaining 52 patients underwent imaging with a novel extremity CBCT scanner (Planmed Verity; Planmed Oy, Helsinki, Finland). Subsequent routine 1.5 T MRA was performed using a dedicated wrist coil. The contrast used was a 1:1 solution of 2.5 mmol/L Gd–tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA) and 240 mg I/mL iohexol. A mean of 2.2 mL (range, 1.5–3.0 mL) was injected into the radiocarpal joint under palpation guidance. The imaging took place while the patient was in sitting position, the forearm in slight to moderate pronation, and the elbow extended. Before the final analysis, the studies were anonymized and assigned a random identification number. One month later, two radio-logists with more than 5 years’ experience in MSK trauma imaging reviewed the CBCT and MRA images twice with at least a 2-week interval between evaluations (5). The radiologists were able to choose any imaging plane using the original high-resolution dataset.
Chondral surfaces of the scaphoid, lunate, and radius facing the scaphoid and lunate were evaluated. The chondral lesions were noted only as present or absent, without grading of the surface extent or depth of injury. The scapholunate (SL) ligament, lunotriquetral (LT) ligament, and TFCC were identified as either intact or torn. The inter- and intraobserver agreements of CBCT arthrography were evaluated in a previously published prospective study (5). In this study, the intraobserver reliability in evaluating radiocarpal chondral surfaces was moderate to substantial (kappa-values, 0.42–0.76) and for interobserver variability fair to substantial (0.32–0.62). On the other hand, for ligamentous structures, the intraobserver reliability varied from moderate to almost perfect (0.59–0.91), and interobserver variability varied from fair to almost perfect (0.31–0.90) (5).
Of the 52 patients, 21 (13 men and 8 women; mean age, 34 years (range, 18–58 years)) underwent wrist arthroscopy as a part of the treatment for their symptoms and due to the findings in the MRA. The mean interval between the CBCT arthrography and the wrist arthroscopy was 7 months (range, 2–23 months). The remaining 31 patients, for whom arthroscopy was not indicated due to symptoms or MRA findings, were treated at the Department of Hand Surgery with other treatment methods, as it was considered unethical to perform an invasive procedure on patients for whom it was not necessary.
The surgeons performing the wrist arthroscopy followed a routine adopted in the hospital for examining radiocarpal and midcarpal joints and reporting findings. The findings of the wrist arthroscopy of the 21 patients were retrospectively collected from the patient database. Standard wrist radiographs were not included in this analysis.
The Geissler arthroscopic classification for carpal instability was used to evaluate ligament tears (9). In this study, a patient was considered to have an SL or a LT ligament tear if the injury seen in arthroscopy reached Geissler grade III or IV. In Geissler grade III, a separation between the carpal bones in evident and a small-joint probe can pass through a gap between the carpal bones. Characteristic of Geissler grade IV is gross instability with manipulation of the bones, and a 2.7-mm arthroscope can pass through the gap between the carpal bones.
Tears of the TFCC were classified as peripheral (ulnar or foveal) or central (central or radial) tears according to the description of the tear in the operative report. Any TFCC tear visible in arthroscopy (peripheral or central) was categorized as having a TFCC tear in the final analysis and different types of TFCC tears were not analyzed separately.
We compared the findings of the CBCT arthrography, MRA, and wrist arthroscopy and used the combined first CBCT and MRA readings for analysis. Sensitivity, specificity, positive and negative predictive values, and accuracy with 95% confidence intervals (CIs) were calculated using a commercial software package SAS/STAT v.9.3 (SAS Institute Inc., Cary, NC, USA).
Results
Wrist arthroscopy revealed a total of 10 cartilage lesions in 5 of the 21 patients (Table 1). Four patients had a tear in the SL ligament, two patients had a tear in the LT ligament, and nine patients had a tear in the TFCC. Four of the TFCC tears were central and five were peripheral. Only one of the TFCC tears was a complete tear off from the fovea (requiring TFCC re-insertion) and the rest were superficial tears not requiring treatment other than debridement.
Comparison of chondral lesions in CBCT and MR arthrography and in wrist arthroscopy.
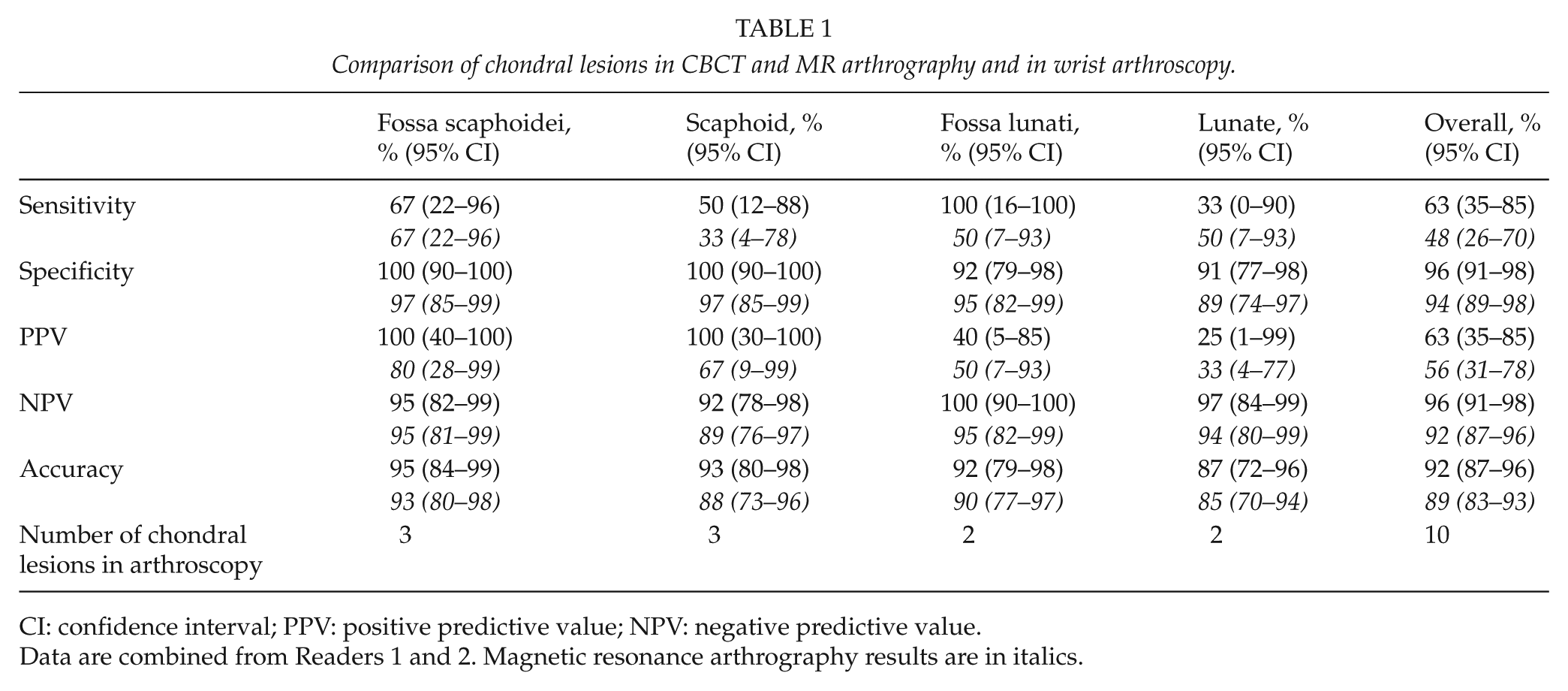
CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value.
Data are combined from Readers 1 and 2. Magnetic resonance arthrography results are in italics.
The patients had also suffered isolated ligament injuries as well as tears associated with TFCC tears or chondral lesions. These findings were treated arthroscopically or in open surgery depending on the patient’s symptoms and overall patient evaluation.
Tables 1 and 2 present the comparative results for CBCT and MRA and wrist arthroscopy for the chondral lesions and ligamentous and TFCC tears. The absolute counts for the two readers are presented in Tables 3 and 4.
Comparison of ligament injuries and TFCC tears in CBCT and MR arthrography and in wrist arthroscopy.
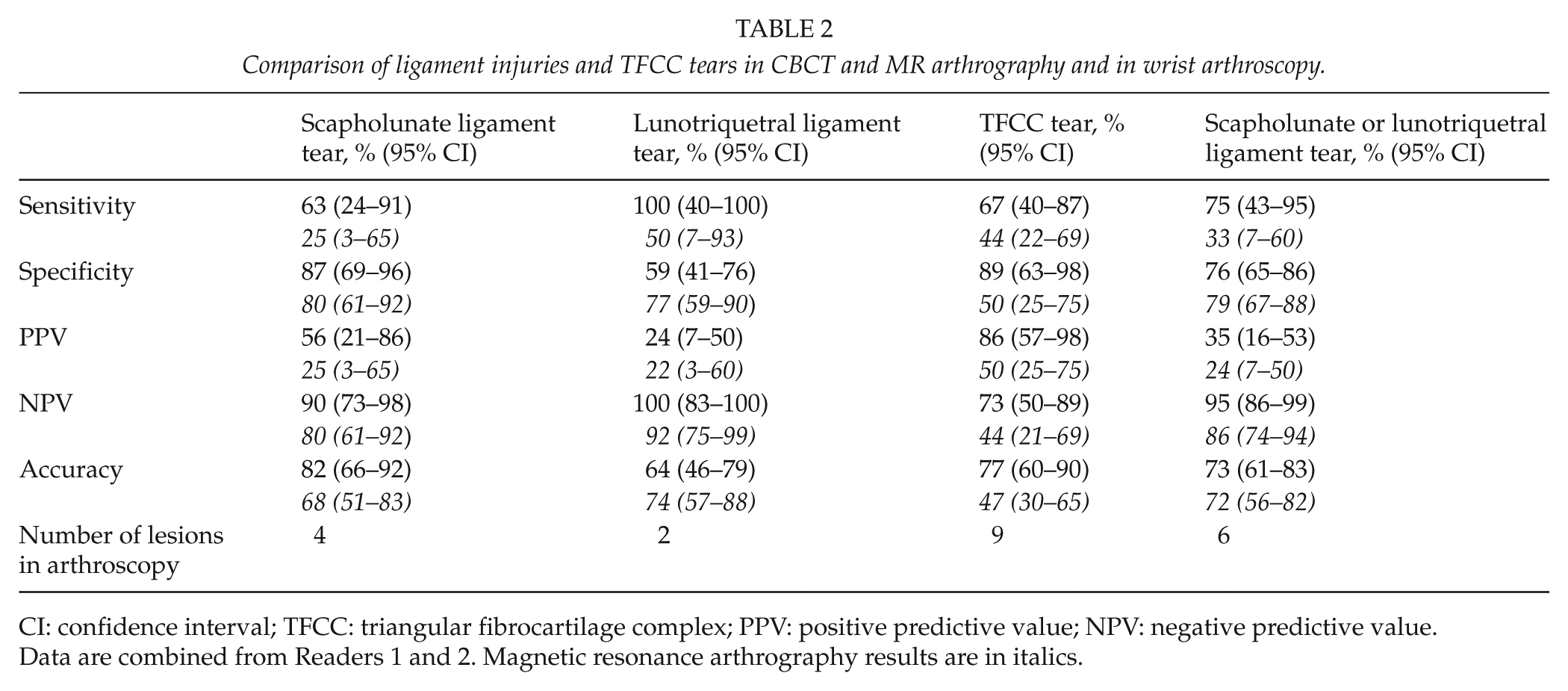
CI: confidence interval; TFCC: triangular fibrocartilage complex; PPV: positive predictive value; NPV: negative predictive value.
Data are combined from Readers 1 and 2. Magnetic resonance arthrography results are in italics.
Absolute counts for Readers 1 and 2 (R1/R2) for chondral lesions.
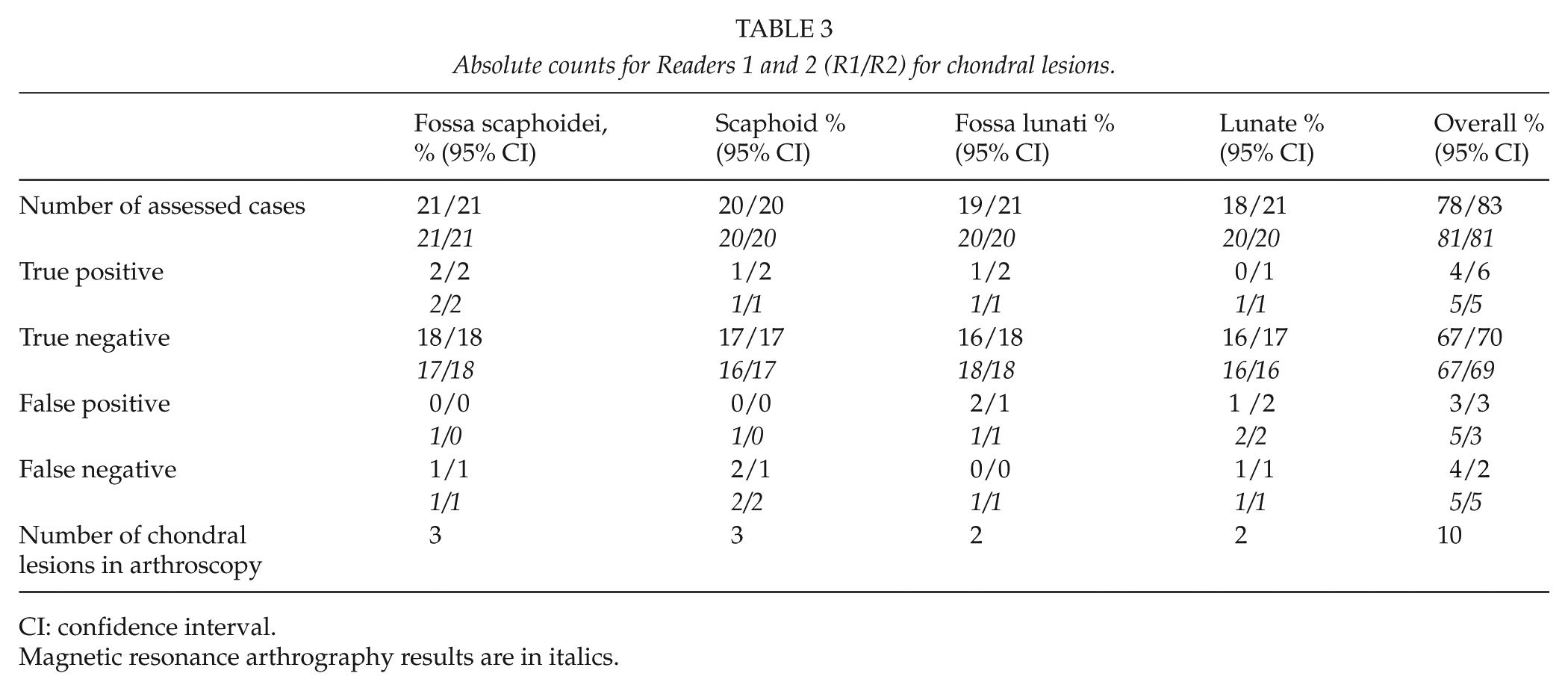
CI: confidence interval.
Magnetic resonance arthrography results are in italics.
Absolute counts for Readers 1 and 2 (R1/R2) for ligament and TFCC tears.
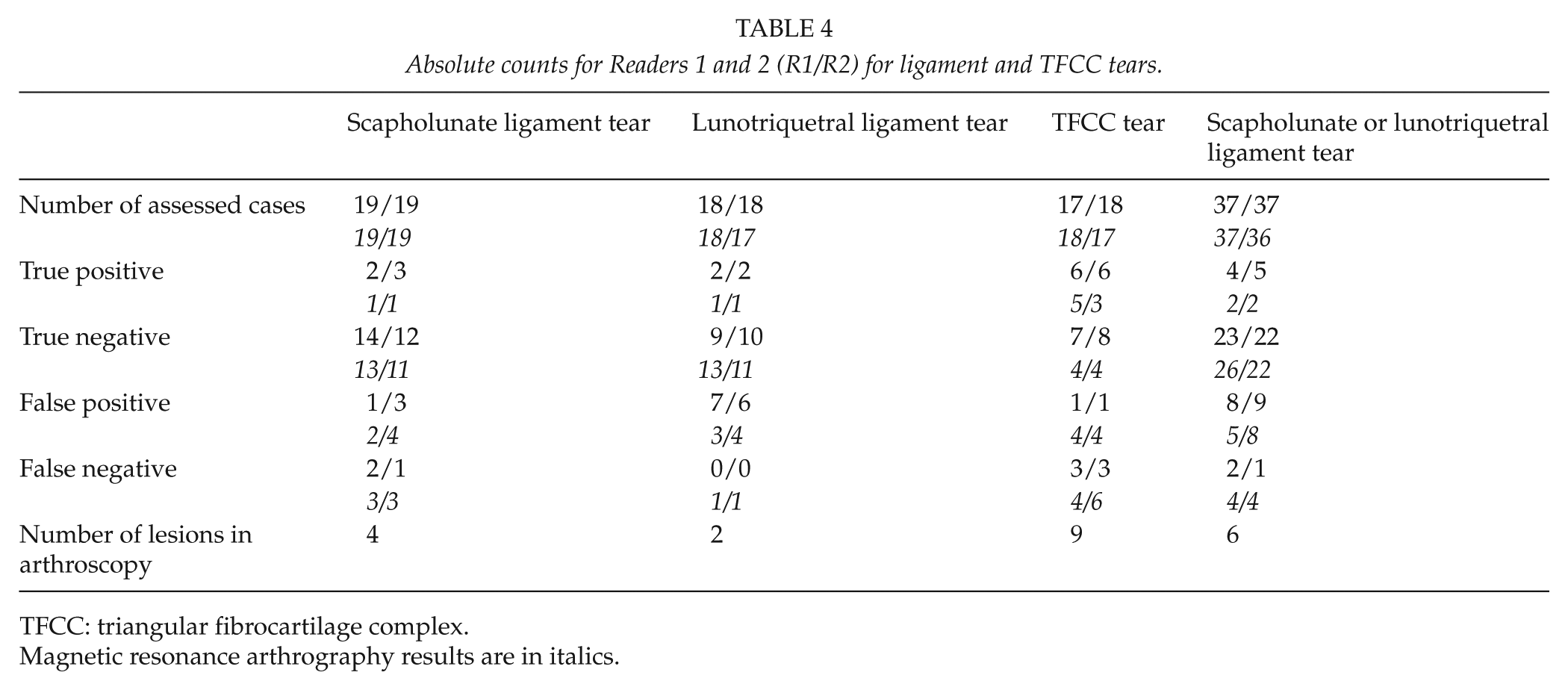
TFCC: triangular fibrocartilage complex.
Magnetic resonance arthrography results are in italics.
For technical reasons, we were unable to assess all structures in all patients in CBCT and MRA. One patient had a previous SL ligament reconstruction and one had a distal intra-articular fracture of the radius. In these patients, the contrast injection was technically challenging, and therefore, contrast concentration remained suboptimal. The number of assessed chondral lesions for CBCT arthrography was 78 of 83 (Reader 1/2) and for MRA 81/81. The number of assessed cases for TFCC tear for CBCT arthrography was 17 of 18 and for MRA 18 of 17. For ligament tears, the respective figures were 37 of 37 and 37 of 36.
For chondral lesions (n = 10), CBCT arthrograms showed slightly higher specificity than MRA. The sensitivity of CBCT arthrography was also better for these lesions, except for those on the chondral surface of the lunate. However, the number of lesions was very small and the 95% CIs are overlapping.
For TFCC injuries (n = 9), CBCT arthrography showed a better specificity and sensitivity than MRA. For ligamentous injuries (n = 6), CBCT arthrograms were more sensitive, but less specific than MRA images.
MRA, CBCT arthrography, and wrist arthroscopy revealed no chondral lesions or ligament injuries in five patients. For these patients, arthroscopy was performed because of severe or persistent symptoms to rule out other wrist abnormalities. One of these patients presented with an occult ganglion that was extirpated arthroscopically. The remaining four patients presented with mild synovitis of the radiocarpal joint or around the TFCC area and underwent arthroscopic debridement.
Fig. 1 shows a true-positive SL tear identified in CBCT arthrography, MRA, and arthroscopy. CBCT arthrography revealed a small tear in the LT ligament, although it was not visible in either MRA or wrist arthroscopy, thus representing a small tear without instability of the ligament. Fig. 2 shows the radial scaphoid fossa and lunate chondral defects as well as an LT tear identified in CBCT arthrography, MRA, and wrist arthroscopy.
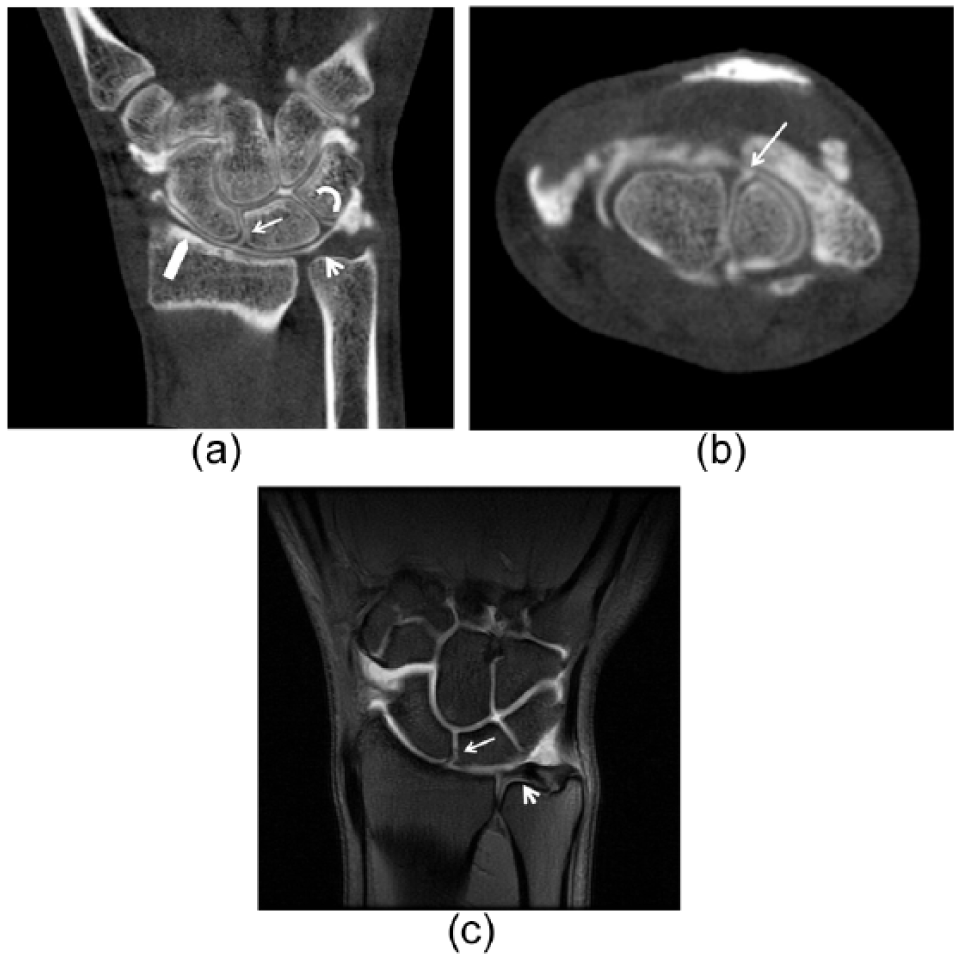
(a) Coronal and (b) axial CBCT images and (c) coronal T1 fs MR arthrography image of the same patient. A true-positive SL tear (arrow, a–c) in a 22-year-old male that was identified in CBCT arthrography, MR arthrography, and arthroscopy. Contrast leakage is seen in the midcarpal joint through the SL tear. A small tear was also identified in the LT ligament in CBCT arthrography (curved arrow, a), but it was not visible in arthroscopy or in MR arthrography, thus representing a small tear without instability of the ligament. No perforation in TFC (arrowhead, a and c) is seen. Note also the excellent visualization of cartilage in CBCT arthrography image (block arrow, a).
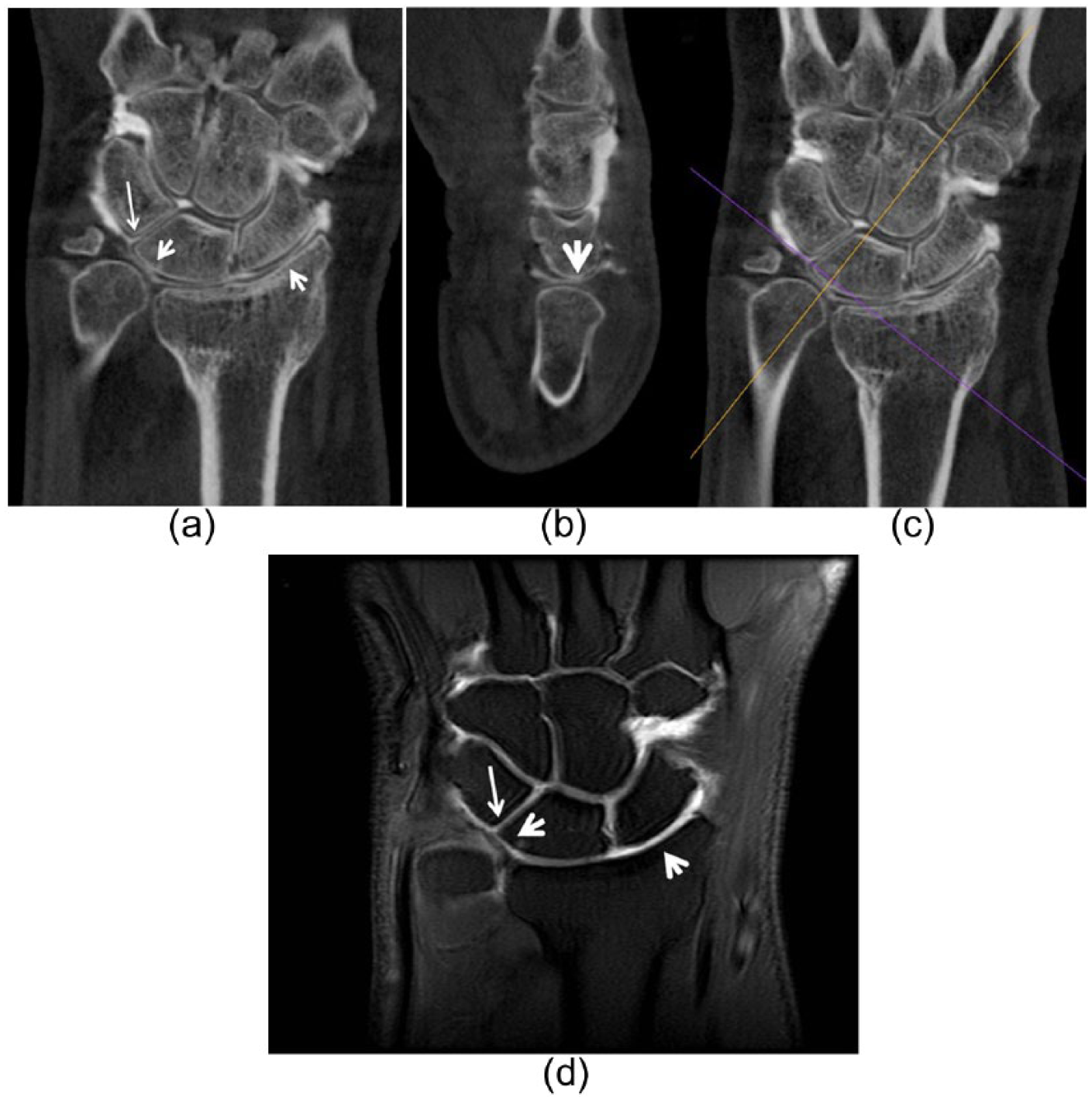
(a) Coronal, (b) oblique sagittal, (c) and coronal CBCT images and (d) coronal T1 fs MR arthrography image of the wrist in a 55-year-old male. Radial scaphoid fossa and lunate chondral defects (arrowheads, a and d) and an LT tear (arrow, a and d) were identified in CBCT arthrography, MR arthrography, and arthroscopy. The orange line in the coronal image (c) shows the plane to create the oblique sagittal plane in b.
Discussion
Wrist arthroscopy is often performed on patients with acute or chronic wrist pain in an effort to diagnose chondral lesions or ligament tears and to evaluate the TFCC. Arthroscopy is, however, an invasive procedure that involves the usual risks of surgery and anesthesia. Therefore, ideally, diagnosis of the underlying cause of wrist pain would be confirmed with wrist imaging instead.
Several options exist for wrist imaging: plain radiographs, MRI, MRA, conventional CT, CT arthrography, and the novel CBCT. Each imaging technique offers certain advantages and drawbacks, and thus, the choice of imaging modality often depends on personal preferences and access to these modalities. Ideally, the wrist imaging modality should be precise and sensitive in excluding chondral lesions and ligamentous tears.
MRA is an established technique for detecting ligament injuries, even though the technique is rather expensive and may have contraindications (10, 11). It is, however, also known that not all articular traumatic or pathological abnormalities of the wrist can be defined or excluded with MRI. Often, the appearance, depth, and extent of the chondral lesion seen in wrist arthroscopy guide the surgeon in choosing the appropriate surgical procedure (e.g. ligament reconstruction or partial radiocarpal arthrodesis in SL ligament injury). This decision may be challenging based on MRI images alone. On the other hand, severe chondral abnormalities and osteoarthritis can be diagnosed in standard radiographs and no cross-sectional imaging is needed.
Relative to the gross pathologic inspection of cartilage surfaces in cadaveric wrists, MRI has shown a sensitivity of 43%–52% for cartilage lesions (12). This is also in accordance with our study, as we observed an overall sensitivity for chondral lesions of 48% with MRA. In the study of cadaveric wrists, the sensitivity was higher for the proximal carpal row (67%–71%) than for the distal carpal row (14%–24%).
In a comparative study on MRI and arthroscopy in evaluating wrist ligament and TFCC tears (13), 35 of 49 patients underwent MRA in addition to conventional MRI. MRA proved 100% sensitive and 100% specific in detecting ligament and TFCC tears. We also found a high specificity for ligamentous tears (79%), but a much lower sensitivity (33%) when comparing MRA with arthroscopic findings.
CT arthrography is an alternative technique of wrist imaging that can reveal bony and chondral lesions, ligament injuries, and tears of the TFCC. Compared with conventional MRI, both CT arthrography and MRA have higher accuracy in diagnosing tears of the SL and LT ligaments as well as of the TFCC of the wrist (14). CT arthrography has also been shown to be better in identifying which component of interosseous carpal ligaments is injured (14).
A comparative evaluation of wrist ligament and cartilage injuries has previously been performed for CBCT and cadaveric specimens by Ramdhian-Wihlm et al. (3). They found 100% accuracy for cartilage tears, 77% for TFCC tears, and 74% for SL/LT ligament tears, in concordance with our findings of 92%, 77%, and 73%. In a comparative study on conventional CT arthrography and arthroscopy of the wrist by Bille et al. (15), CT arthrograms were demonstrated to be highly accurate in detecting SL, LT, and TFCC tears, with high sensitivity and specificity (SL 94%/86%, LT 85%/79%, TFCC 30%/94%). Their study also revealed that CT is not a precise tool in detecting peripheral TFCC tears.
Due to the small number of patients with ligament tears, we conducted no separate analysis of the specific anatomic location of the tear. For the same reason, no separate analyses of central and peripheral tears of the TFCC were performed. The small number of positive findings is a limitation of this study.
CT arthrography appears to provide a better accuracy than MRA in evaluating partial ligament tears (16). For CT, Bille et al. (15) found that the sensitivity and specificity for SL tears were 94% and 86%, respectively. We observed a lower sensitivity for both CBCT and MRA, but a comparable specificity for CBCT. For LT tears, Bille et al. (15) reported a sensitivity of 85% and a specificity of 79%, whereas the corresponding values in our study for CBCT arthrography were 100% and 59%. For cartilage lesions in their study, CT had a sensitivity of 45% and a specificity of 97%; our corresponding values for CBCT were 63% and 96%.
There was reasonably high number of false-positive ligament tears in our study. This may be explained by small partial tears and perforations of the ligaments that are not always visible in wrist arthroscopy. These small ligament tears are also clinically irrelevant.
The hand surgeons performing the wrist arthroscopy had access to the MRA images, but they were not aware that the patients were participating in the study, and therefore, the CBCT arthrography findings could not have influenced the surgeons’ reports on the results of the arthroscopy. CBCT with high spatial resolution is an emerging imaging modality in musculoskeletal radiology and it offers several advantages over CT and MRI. The radiation dose is lower than in CT (7), and the examination is faster than in MR imaging and offers a more pleasant option for patients suffering from claustrophobia. CBCT units are less expensive and require less space than CT equipment. These units can even be placed in operating rooms. One clear advantage of the current CBCT system is its high anatomic spatial resolution, which exceeds the 0.23 mm3 standard of the current clinical scanners, including most CT or MRI scanners, permitting even more accurate cartilage and ligament evaluation. Also, CBCT can be especially useful in cases with orthopedic implants near the wrist or if MRA is contraindicated.
Due to small number of positive findings in this study, the role of the CBCT arthrogram remains unclear, particularly in ligamentous injuries, but this study shows that this imaging modality has potential to identify healthy chondral surfaces and it can probably also replace MR when needed. Regarding the ligamentous injuries, its usefulness should be further explored in a larger study. CBCT arthrography seems to have similar sensitivity, specificity, and accuracy compared to MR. If readily available, CBCT serves as a valuable option in evaluating patients with acute or chronic wrist pain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Ethics Committee of Helsinki University Central Hospital (reference no. 266/12/03/02/2010).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.