
Abstract
Background and Aims:
The laparoscopic approach has been increasingly used to treat adhesive small-bowel obstruction. The aim of this study was to compare the outcomes of a laparoscopic versus an open approach for adhesive small-bowel obstruction.
Material and Methods:
Data were retrospectively collected on patients who had surgery for adhesive small-bowel obstruction at a single academic center between January 2010 and December 2012. Patients with a contraindication for the laparoscopic approach were excluded. A propensity score was used to match patients in the laparoscopic and open surgery groups based on their preoperative parameters.
Results:
A total of 25 patients underwent laparoscopic adhesiolysis and 67 patients open adhesiolysis. The open adhesiolysis group had more suspected bowel strangulations and more previous abdominal surgeries than the laparoscopic adhesiolysis group. Severe complication rate (Clavien–Dindo 3 or higher) was 0% in the laparoscopic adhesiolysis group versus 14% in the open adhesiolysis group (p = 0.052). Twenty-five propensity score–matched patients from the open adhesiolysis group were similar to laparoscopic adhesiolysis group patients with regard to their preoperative parameters. Length of hospital stay was shorter in the laparoscopic adhesiolysis group compared to the propensity score–matched open adhesiolysis group (6.0 vs 10.0 days, p = 0.037), but no differences were found in severe complications between the laparoscopic adhesiolysis and propensity score–matched open adhesiolysis groups (0% vs 4%, p = 0.31).
Conclusion:
Patients selected to be operated by the open approach had higher preoperative morbidity than the ones selected for the laparoscopic approach. After matching for this disparity, the laparoscopic approach was associated with a shorter length of hospital stay without differences in complications. The laparoscopic approach may be a preferable approach in selected patients.
Keywords
Introduction
Small-bowel obstruction (SBO) is a major cause of emergency hospital admission, and intra-abdominal adhesions related to prior abdominal surgery is the etiologic cause in up to 75% of cases of SBO in developed countries (1). Laparoscopy has been shown in the short term to lead to shorter length of stay and to cause fewer readmissions due to adhesions in the long term compared to open surgery in various settings (2–4).
However, traditionally, adhesive small-bowel obstruction (ASBO) has been viewed by surgeons as a contraindication to laparoscopic surgery because of the risk of iatrogenic injury to the distented and fragile bowel. Such injuries might go unnoticed during the operation because of decreased visibility due to distention of the bowel and frequent postoperative adhesions (5, 6). Since the first report on laparoscopic section of a single band responsible for SBO by Bastug et al. (7) in 1991, research has shown laparoscopy to be a safe, feasible, and possibly even superior method for managing SBO compared to the open approach (6). However, as no prospective randomized trials comparing the laparoscopic and open management of SBO have been published (6), research published to date is likely to be influenced by selection bias and conclusive data on the subject are lacking. The aim of this study was to compare the preoperative characteristics of patients undergoing laparoscopic versus open approach, match these groups based on preoperative parameters, and compare the outcomes of the matched groups.
Materials and Methods
Data Collection and Analysis
This retrospective comparative study was performed at a university hospital that serves both as a secondary hospital for a population of 0.5 million as well as a tertiary referral hospital for 1.5 million people. Patients were identified from electronic patient records by search for postoperative International Classification of Diseases (10th ed.; ICD-10) diagnosis code K56.5 (intestinal adhesions with obstruction) during 2010–2012. Patient medical history, clinical signs and findings prior to surgery, laboratory parameters as well as other perioperative and postoperative outcomes were obtained from electronic medical records. Complications and mortality within 30 days postoperatively were recorded. Patients who died during their hospital stay were excluded from the analyses for length of stay (total or postoperative). Collected data were statistically analyzed using the SPSS Statistics v. 22 (IBM, Armonk, New York, USA). T-test, Mann–Whitney U test, Fisher’s exact test, and Pearson’s χ2 test were used where appropriate. All tests were carried out two-tailed with α = 0.05. For matched groups, for each patient operated by laparoscopic approach, one patient operated using open approach was chosen based on closest propensity score calculated from the preoperative parameters shown in Table 1. Institutional review board approved the study.
Patient baseline characteristics.
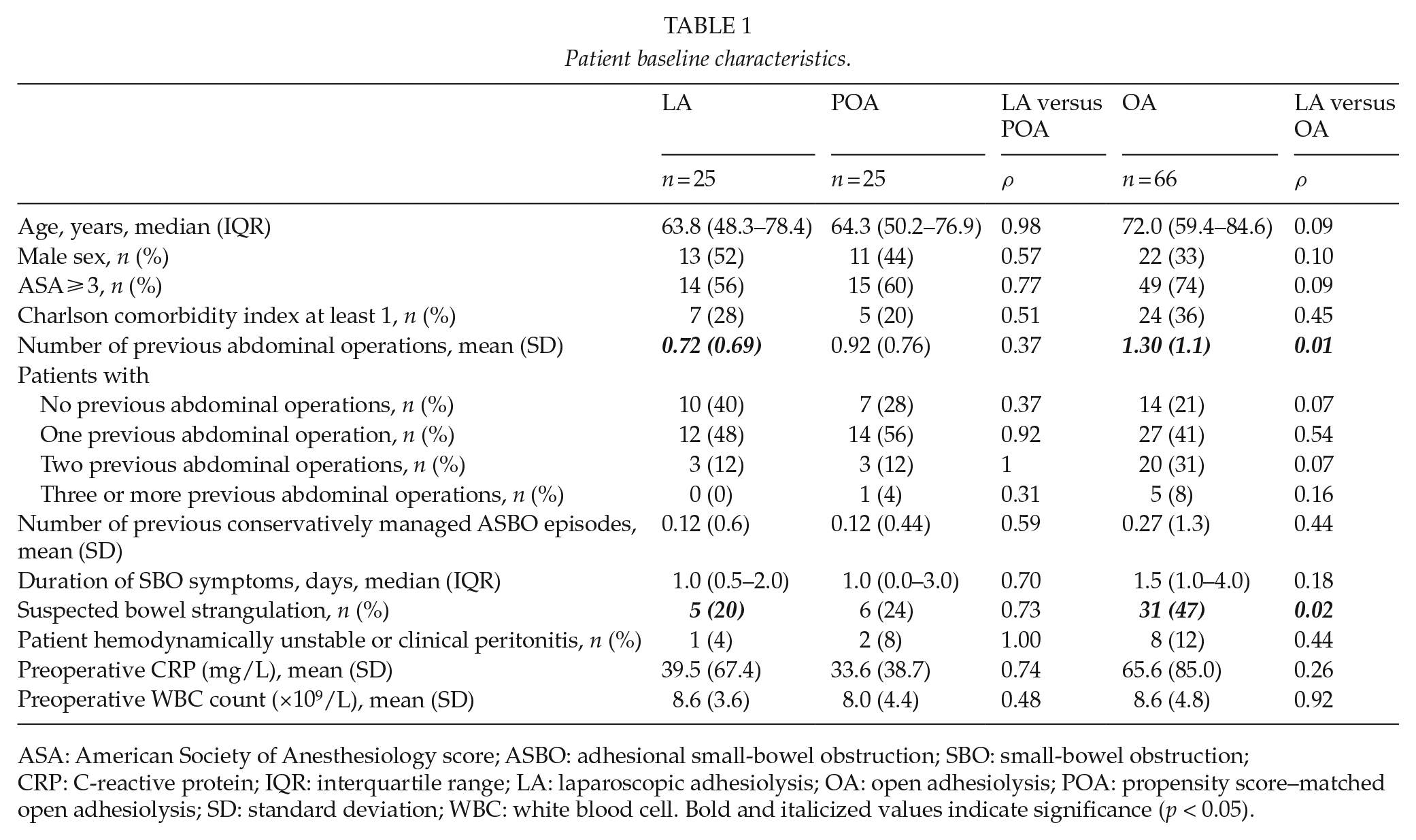
ASA: American Society of Anesthesiology score; ASBO: adhesional small-bowel obstruction; SBO: small-bowel obstruction; CRP: C-reactive protein; IQR: interquartile range; LA: laparoscopic adhesiolysis; OA: open adhesiolysis; POA: propensity score–matched open adhesiolysis; SD: standard deviation; WBC: white blood cell. Bold and italicized values indicate significance (p < 0.05).
Operative Technique
For laparoscopy, access to the peritoneal cavity was obtained under direct visual control using the Hasson open technique. Most commonly, the chosen point of entry was just above or below the umbilicus. After insufflating the peritoneal cavity with CO2 gas up to 12 mmHg, additional trocars were placed under direct visual control as necessary. If the site and cause of obstruction were not apparent on general inspection, the ileocecal junction was identified and the small bowel was followed orally, until the point and cause of obstruction could be identified. Most commonly, division of adhesions was performed using cold scissors.
For the open technique, a midline incision was used. Whenever possible, the whole small intestine was freed from adhesions. Bowel was decompressed either through nasogastric tube or, in cases of bowel resection, through enterotomy.
Results
Patients
A total of 190 operated patients were identified by the diagnosis code and patient records manually analyzed. Patients with no ASBO were excluded (n = 25). Furthermore, in order to reduce selection bias, patients who had a contraindication for laparoscopic approach by our hospital standards were excluded. These include patients with a history of intra-abdominal malignancy or surgery for endometriosis and inflammatory bowel disease mainly due to the fact that these patients often have other causes for bowel obstruction that might be overlooked in laparoscopy. Furthermore, patients with a history of diffuse peritonitis, abdominal wall hernia mesh repair, and prior abdominal operation within 30 days are not considered for laparoscopy due to frequent diffuse adhesions. A total of 74 patients were excluded due to these reasons forming the final cohort of 91 patients (Fig. 1). A total of 25 patients initially had laparoscopic adhesiolysis (LA) and 66 patients open adhesiolysis (OA). Six patients (24%) in the LA group were converted to open surgery, but remained in the LA group for analyses. In two patients, the conversion was due to an inadvertent enterotomy and in four due to the inability to localize the obstruction. Patient baseline characteristics are presented in Table 1. Patients with OA had more often a suspicion of bowel strangulation (46% vs 20%, p = 0.02) and more previous abdominal operations (mean 1.28 vs 0.72, p = 0.01) than LA group (Table 1).
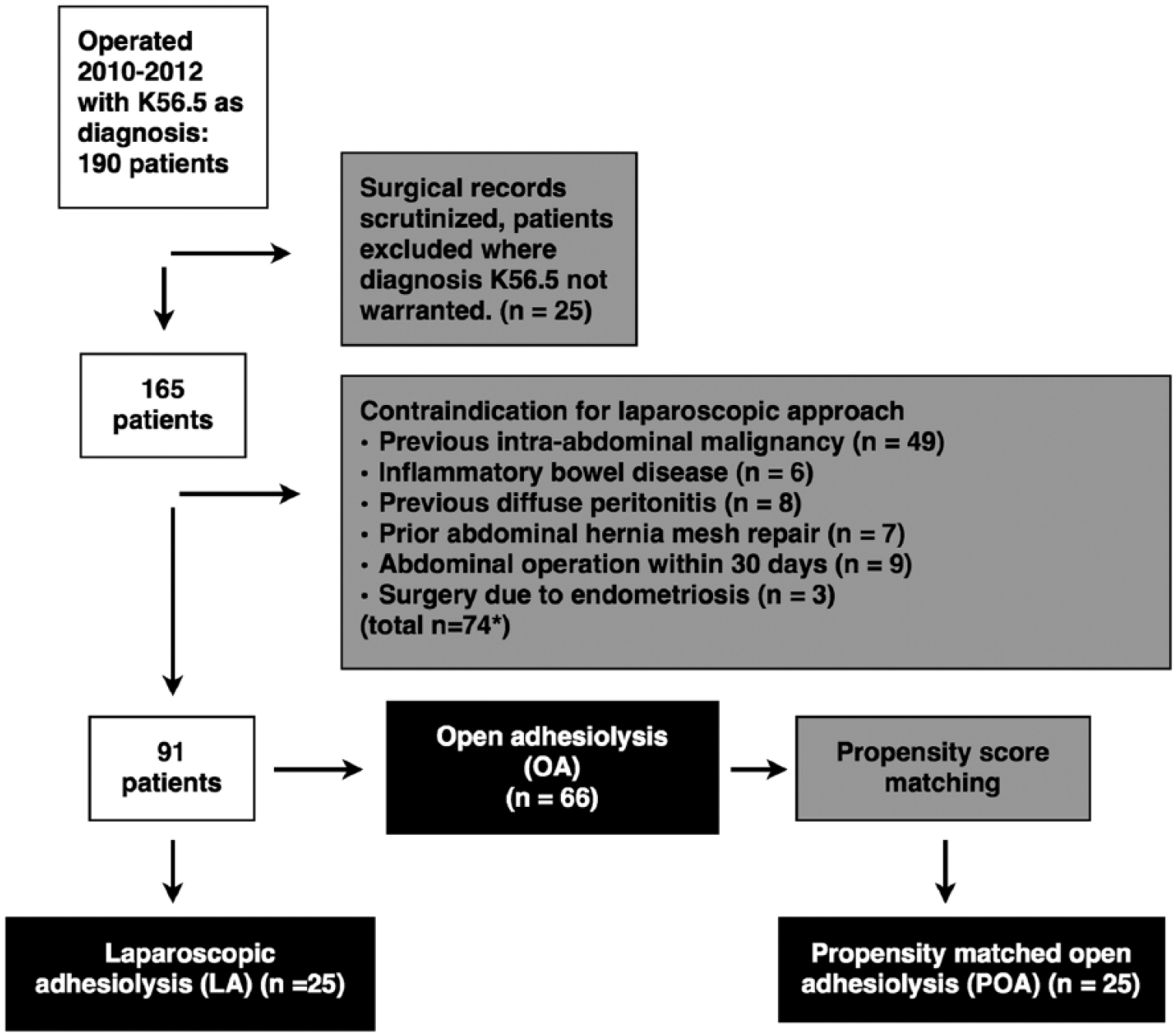
Flowchart presenting patient selection.
LA versus OA
Compared to OA, LA was associated with shorter total (median 6 vs 9 days, p = 0.01) and postoperative (median 3 vs 6 days, p = 0.001) length of stay as well as shorter operating room stay (112 vs 135 min, p = 0.02) (Table 2). There was less irreversible ischemia (0% vs 20.9%, p = 0.01) or need for bowel resection (0% vs 24%, p = 0.01) in the LA group compared to OA group (Table 2). Total time spent in the operating room was slightly higher in the OA group (112 vs 137 min, p = 0.01), but operative time was comparable (41 vs 54 min, p = 0.10). Highest C-reactive protein (CRP) level during hospital stay showed a trend toward higher values in OA group (130 vs 160 mg/L, p = 0.06) (Table 2). Iatrogenic bowel lesions occurred similarly in both groups (overall LA 6 (24%) vs OA 17 (26%) patients, p = 0.86; serosal injury LA 2 (8%) vs OA 13 (19%), p = 0.10; bowel perforation LA 4 (16%) vs OA 4 (6%), p = 0.21) and were all detected during the primary operation. Overall complication rate did no differ between the groups (16% vs 24%, p = 0.40), but OA group showed a trend toward higher severe (Clavien–Dindo 3 or higher) complications (0% vs 14%, p = 0.052) (Table 3).
Perioperative characteristics.
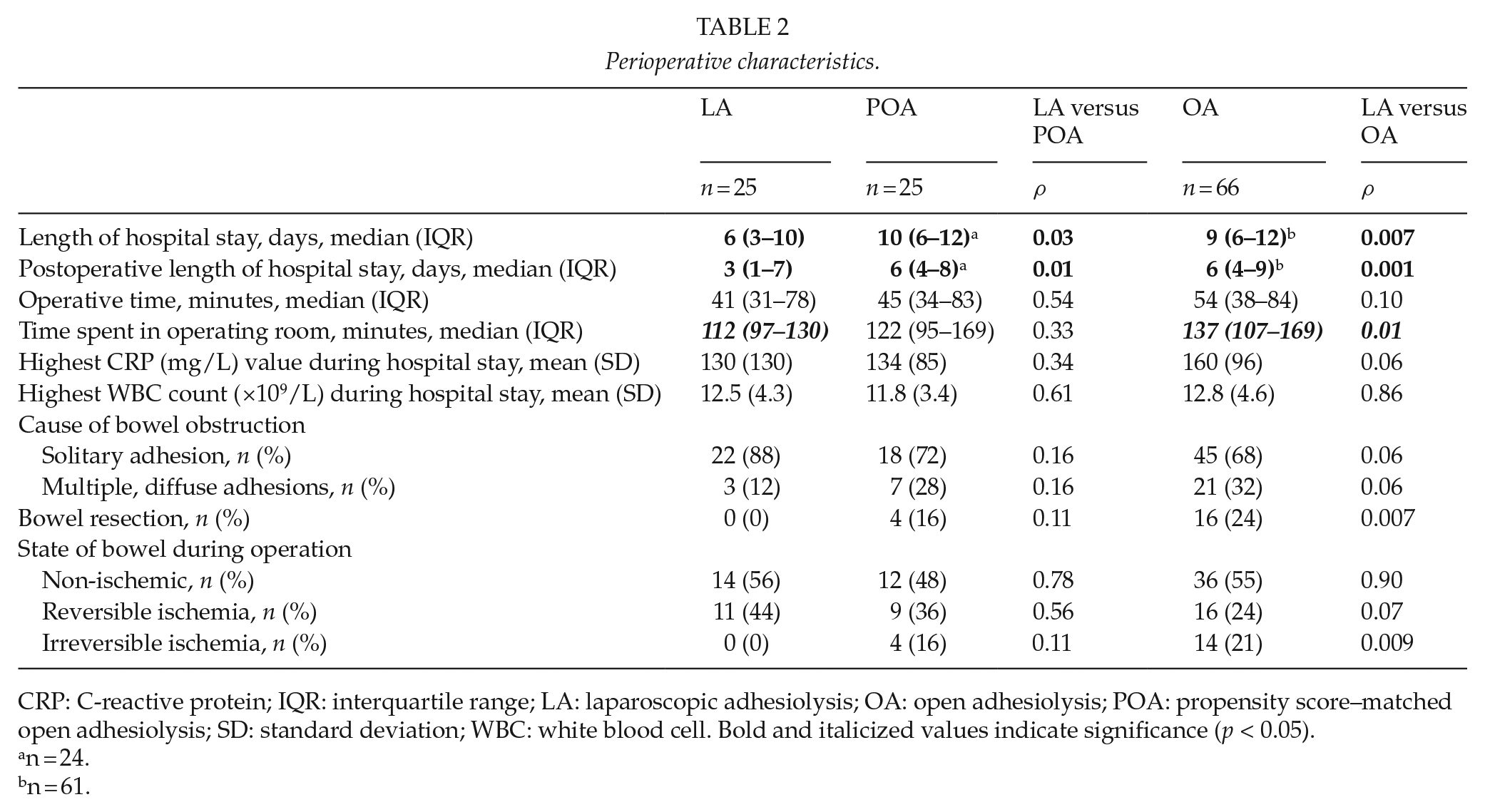
CRP: C-reactive protein; IQR: interquartile range; LA: laparoscopic adhesiolysis; OA: open adhesiolysis; POA: propensity score–matched open adhesiolysis; SD: standard deviation; WBC: white blood cell. Bold and italicized values indicate significance (p < 0.05).
n = 24.
n = 61.
Complications.
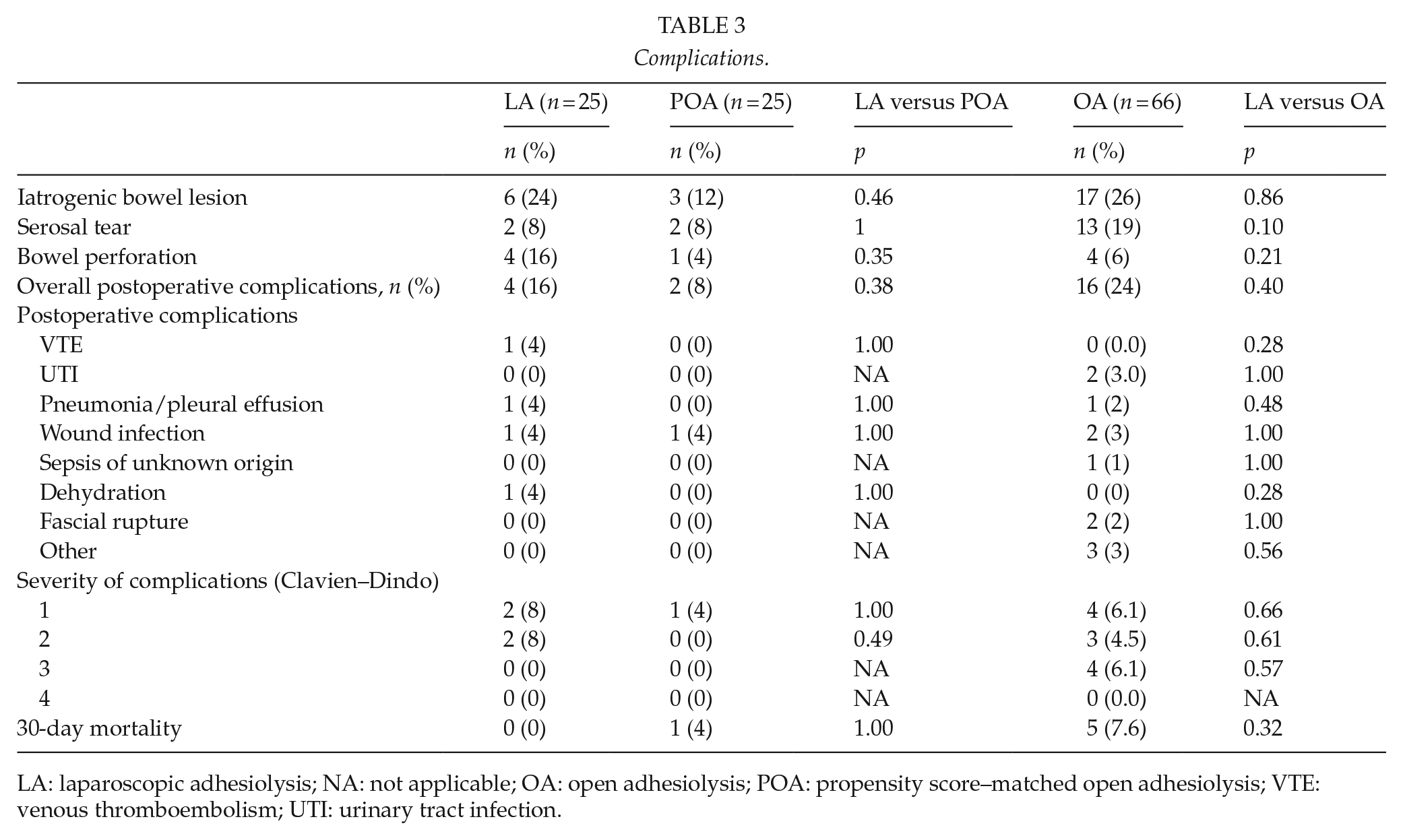
LA: laparoscopic adhesiolysis; NA: not applicable; OA: open adhesiolysis; POA: propensity score–matched open adhesiolysis; VTE: venous thromboembolism; UTI: urinary tract infection.
Laparoscopic Approach versus Propensity-Matched Open Adhesiolysis
There were no differences between LA and propensity score–matched open adhesiolysis (POA) groups in preoperative parameters indicating proper matching (Table 1). Compared to POA, LA was associated with shorter total (median 6 vs 10 days, p = 0.04) and postoperative (median 3 vs 6 days, p = 0.001) length of hospital stay without differences in complications (Tables 2 and 3). Operative time, inflammatory parameters (CRP and white blood cell count), proportion of diffuse adhesions, and bowel vitality during operation were comparable in LA and POA groups (Table 2).
Discussion
We report here that a laparoscopic approach for ASBO reduces length of hospital stay compared to OA without affecting complication rates or mortality in propensity-matched analyses. Furthermore, our data show that less challenging cases and less critically ill patients are more likely to be selected for laparoscopic surgery. This selection bias has not been addressed in most of the previous retrospective cohort studies comparing the laparoscopic approach to open surgery for ASBO (8–10) or only partially addressed (11–14).
Previously, authors who have systematically analyzed and compared baseline characteristics have found significant differences between groups (10, 13–15). Patients having open surgery are older, more likely to be female, have more previous comorbidities as well as a higher number of previous abdominal surgeries and are more often in need of emergent surgery. These data are in line with the results of the first part of our analysis.
In recent years, many studies in which LA and OA have been compared against each other have yielded results favoring the laparoscopic method at least for some patients (8, 10–15). As patient baseline differences have not been accounted for or have only partially been accounted for in these studies, it is likely that at least some of these studies show laparoscopy in a too positive light. Using data from the American College of Surgeons’ National Surgical Quality Improvement Program database, Lombardo et al. (16) compared 222 patient pairs propensity-matched for baseline characteristics and found laparoscopy to be associated with a reduction in length of hospital stay (4 vs 10 days) as well as a lower risk of complications (odds ratio, 0.41). We found a 4-day reduction in length of hospital stay comparing laparoscopically managed patients against the propensity-matched openly managed group.
The more widespread use of computed tomography seems not only to be useful for diagnosis but also a valuable tool in preoperative planning. LA has been shown to be more likely to be successful if the site of obstruction is caused by a simple band with a clearly identifiable transition zone above the pelvic brim (9, 17).
Previously, laparoscopic surgery for SBO has been associated with a considerable number of iatrogenic bowel perforations, a small but considerable number of which remain unnoticed during the operation. Dindo et al. (18) published the results of 537 patients entered in a Swiss multicenter database who had laparoscopy for SBO between 1995 and 2006. The overall conversion rate was 32.4%. When a conversion was pre-emptive, for example, due to matted adhesions or poor visibility, postoperative morbidity was 19.4% and 20.5% for laparoscopically assisted procedures with a small target incision. However, when the conversion was due to an intraoperative complication, postoperative morbidity rose to 45.9%. A higher body mass index (BMI) was found to be independently associated with a higher reactive conversion rate.
Taken together, previous as well as our research suggests that unless selection bias is systematically accounted for, comparing laparoscopy against laparotomy for adhesiolysis will overestimate the benefits of laparoscopy because surgeons are likely to manage more difficult cases by laparotomy.
In light of our and previously published research, patients who are relatively healthy, have few previous abdominal surgeries, and have a bowel obstruction caused by a simple adhesion are most likely to benefit from laparoscopy when compared to the open surgery (15, 16). The situation is less clear for patients who have more baseline morbidity and an obstruction caused by more complex adhesions (9, 17, 18). It is likely that there is a group of patients in whom laparoscopy should not be attempted as it is likely to be harmful.
The key limitations to our study were the retrospective study setting as well as the relatively small sample size with similar limitations applying to previously published studies on laparoscopic management of ASBO and SBO in general (6, 19). We tried to mitigate the effects of selection bias on our study by first excluding patients with contraindications to laparoscopy, and, second, by matching the open and laparoscopic group using propensity scores based on preoperative parameters. To date, high-quality data on the subject based on prospective randomized trials are lacking. Recent studies have tried to mitigate selection bias (14–16), but nevertheless the benefits of laparoscopy might be overestimated. This series comprises patients operated on between 2010 and 2012, and in 2013 we have started a prospective, multicenter, randomized, controlled trial comparing LA to open surgery (20), which will hopefully provide us with more information regarding the benefits and harms of the laparoscopic approach for ASBO.
In conclusion, the laparoscopic approach seems to be beneficial in selected patients with ASBO by shortening the length of hospital stay, but prospective randomized trials are needed to confirm the benefit of laparoscopy in ASBO.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by Vatsatautien tutkimussäätiö Foundation, Mary and Georg Ehrnrooth’s Foundation, and governmental competitive funds (EVO).