
Abstract
Background and Purpose:
Proximal humerus fractures are common fragility injuries. The incidence of these fractures has been estimated to be 82–105 per 105 person-years. Treatment of this fracture, especially in the elderly, is controversial. Our study group published a systematic review of the available literature and concluded that non-operative methods are favored over operative methods in three- and four-part fractures. The aim of this multinational study was to compare treatment policies for proximal humerus fractures among the Nordic countries and Estonia.
Materials and Methods:
The study was conducted as a questionnaire-based survey, using the Internet-based program, Webropol® (webropol.com). The questionnaire link was sent to the surgeons responsible for treating proximal humerus fractures in major public hospitals in Estonia, Finland, Norway, and Sweden. Questionnaire included questions regarding the responder’s hospital, patient characteristics, and examinations taken before decision making. Clinical part included eight example patient cases with treatment options.
Results:
Of the 77 recipients of the questionnaire, 59 responded; consequently, the response rate was 77%. Based on the eight presented displaced fracture examples, in both Estonia and Norway and in Finland, 41% and 38%, respectively, preferred surgical treatment with locking plate. In Sweden, the percentage was 28%. The pre- and post-operative protocols showed a similarity in all participant countries.
Conclusion:
Our survey revealed a remarkable uniformity in the current practice of operative treatments and rehabilitation for proximal humerus fractures in the participant countries.
Introduction
Proximal humerus fractures are common fragility injuries. The incidence of these fractures has been estimated to be 82–105 per 105 person-years [1, 2]. Treatment of this fracture, especially in the elderly, is controversial. A variety of options, including conservative treatment and operative treatment either with plates, hemiprosthesis, or total glenohumeral joint prostheses, are available.
In recent years, five randomized controlled trials (RCTs) compared non-operative versus operative treatment of proximal humerus fractures have been published [3–7]. Our study group published a systematic review of the available literature and concluded that non-operative methods are favored over operative methods in three- and four-part fractures [8]. However, a limitation of the existing studies is that the group sizes in these RCTs were small; further trials are thus needed. While the literature weakly supports non-operative treatment in three- and four-part fractures, there is increasing interest in using reverse prosthesis for these fractures [9]; recently, an RCT regarding this subject was launched [10]. To date, it is unclear how individual surgeons decide upon treatment options and how the new trends are affecting decision making in clinical practice.
Nordic countries and Estonia represent an ideal platform for studying possible changes in the clinical practice of treating proximal humerus fractures because of the relatively homogenous population of approximately 22 million people. The area has a common history, with Nordic cooperation via the Nordic Orthopaedic Federation (NOF), which holds regular conferences. Moreover, these countries have a quite similar healthcare system. Thus, evidence-based treatment policies are expected to be adopted quite easily in these countries compared to the fee-for-service and insurance-based healthcare systems such as those in the United States. In Finland, Norway, and Sweden, but not in Estonia, hospital discharge registers exist. A recent Finnish report showed an increasing trend toward operative treatment of proximal humerus fractures [11]. Whether this trend is also occurring in other Nordic countries and in Estonia is not known. Thus, the aim of this multinational study was to compare opinions for proximal humerus fractures treatment among the orthopedic surgeons treating shoulder fractures in Nordic countries and Estonia.
Patients and Methods
The study was conducted as a questionnaire-based survey, using the Internet-based program, Webropol® (webropol.com). The study investigated current opinion with respect to proximal humerus fracture treatment. The questionnaire link was sent to the surgeons responsible for treating proximal humerus fractures in major public hospitals in Estonia, Finland, Norway, and Sweden. If the orthopedic surgeon did not respond, a reminder was sent by electronic mail. Data were collected between 15 November 2014 and 15 January 2015. Altogether, questionnaires were sent to 77 orthopedic surgeons; the distribution among the different countries was proportional to the number of inhabitants in each country (Table 1). As the study covered regions with four different languages, we used only English to avoid understandability problems. Prior to sending out the questionnaire, it was pilot-tested four times with 10 experienced shoulder surgeons to ensure the validity of each question.
Number of sent questionnaires, answers, and inhabitants per country. Percentages of the total are presented in parentheses.

The questionnaire consisted of four parts. The first part assessed the clinical experience of the participant and the area in which he/she worked (eight questions). The second part included clinical patient cases with plain x-rays and different alternatives for treatment. Of the eight patient cases sent to the respondents, three were two-part fractures, three were three-part fractures, and two were four-part fractures. (eight questions). The third part concerned pre- and post-operative treatment, including post-operative physiotherapy protocol (nine questions). The fourth part concerned opinions and preferences among the current treatment options in case of elderly patient with low energy trauma. The respondent could choose between the two different methods and justify the willingness in scale 1–5 of one method over another, for example, locking plate or reverse prosthesis. (five questions). Parts 1, 2, and 4 were multiple-choice questions, and part 3 included open-ended answers about post-operative protocol. Statistical analyses were performed using two-way tables with Fisher’s exact test. A p value of <0.05 was considered significant.
Results
Of the 77 recipients of the questionnaire, 59 responded; consequently, the response rate was 77%. Table 1 shows the proportion of respondents in each country. All but one of the respondents were either trauma or shoulder surgeons, and 80% had been working in the field of shoulders for >5 years. A total of 79% of the respondents stated that in their hospital, a special shoulder surgeon team existed, and 43% of the respondents worked in a university hospital. The most common catchment area size for the respondents’ hospitals was 100,000–500,000 inhabitants (72% of the responders).
Of those who responded to the questionnaire, 91% annually treated >50 proximal humerus fractures, and 25% reported that the annual number was >200 proximal humerus fractures. A total of 59% of the respondents reported performing surgery on >25 proximal humerus fracture patients per year.
The second part of the survey, which concerned treatment alternatives, included two- to four-part fractures, described in accordance with Neer [12]. Of the eight patient cases, each patient case was shown with two different x-ray projections of the shoulder, and the following options were given: non-operative treatment, operative treatment with a K-wire or tension band, intramedullary nail, locking plate, hemiprosthesis, or reverse prosthesis. Each responder could choose their one or two most preferred options, and the answers provided were regarded as votes for each case. The total number of votes by the respondents was 547.
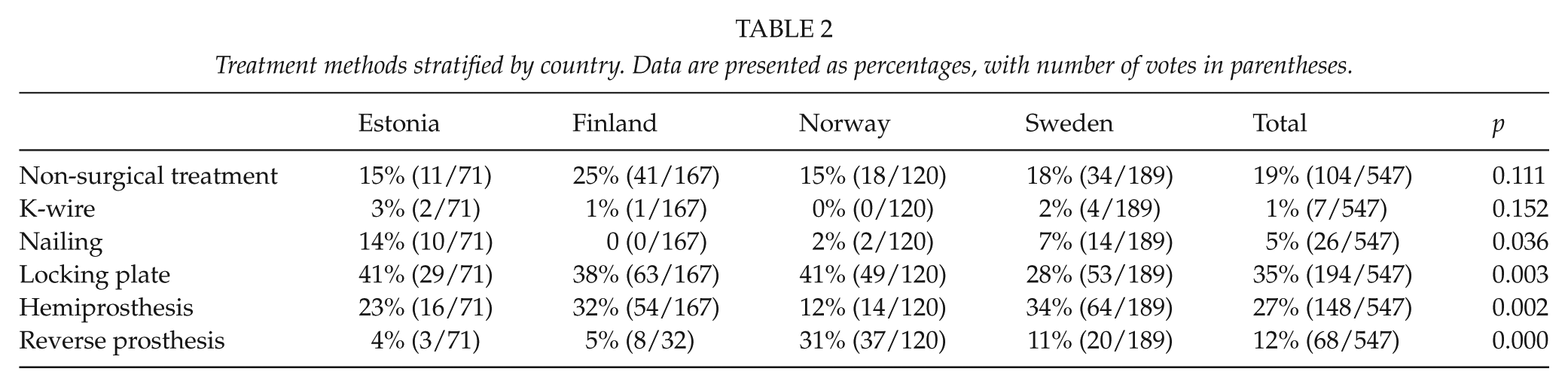
For the eight presented patient cases, the locking plate was preferred in 35% of the responses, followed by hemiprosthesis (27%). Non-operative treatment was preferred in 19% of the responses. The proportion of willingness to provide non-operative treatment did not differ among the countries (p = 0.110). Surgery with K-wire and tension band was preferred in 1% of the responses. In Estonia, 14% of the surgeons preferred nailing as an operative method; this was significantly greater than in the other countries, where only 0–7% preferred nailing (p = 0.036). In both Estonia and Norway and in Finland, 41% and 38%, respectively, preferred surgical treatment with locking plate. In Sweden, the percentage was 28% (p = 0.003). Preferences for the prosthesis options were different in Norway, where use of the hemiprosthesis was significantly lower (12%, p = 0.002), while use of the reverse prosthesis was significantly higher (31%, p = 0.000) compared to all of the other countries. For the hemiprosthesis option, the preference percentages were 23%, 32%, and 34%, respectively, for Estonia, Finland, and Sweden, and for reverse prosthesis they were 4%, 5%, and 11%, respectively. The results are summarized in Table 2.
Treatment methods stratified by country. Data are presented as percentages, with number of votes in parentheses.
Before making a decision regarding treatment, 40/59 (68%) preferred to perform computed tomography (CT) imaging of the shoulder. In preoperative planning, 50/59 (85%) used CT. A majority of the respondents (n = 46, 78%) had a post-operative care protocol in their clinic. All 59 respondents had an in-ward physiotherapist who guided post-operative care. Almost all of the respondents (n = 56, 95%) referred patients to outpatient post-operative physiotherapists. Half of the respondents (n = 27, 46%) preferred two post-operative outpatient visits, while six respondents (10%) preferred more than three post-operative outpatient visits. There were no differences among the countries with respect to CT imaging or preoperative planning.
Physiotherapy protocols for non-operatively treated patients and cases that were addressed with a locking plate were quite similar among the respondents. Most frequently, a sling was used for 2–3 weeks and pendulum movements began immediately after the operation. From two weeks to 4–6 weeks, passive movements were allowed; thereafter, free active mobilization was encouraged. After operations with prostheses, variations in post-operative treatment were wide. In general, after an anatomic prosthesis, sling and pendulum movements were recommended 4–6 weeks after the operation. With reverse prosthesis, after care was started (e.g. with passive mobilization) as early as one week after the operation and continued with active flexion exercises from four weeks onward.
In the last part of the questionnaire, we allowed the respondents to choose between two different treatment methods in an imaginary elderly patient with low energy trauma. The differences in recommended treatments were only minor and statistically insignificant among the four countries. The results are summarized in Figure 1.
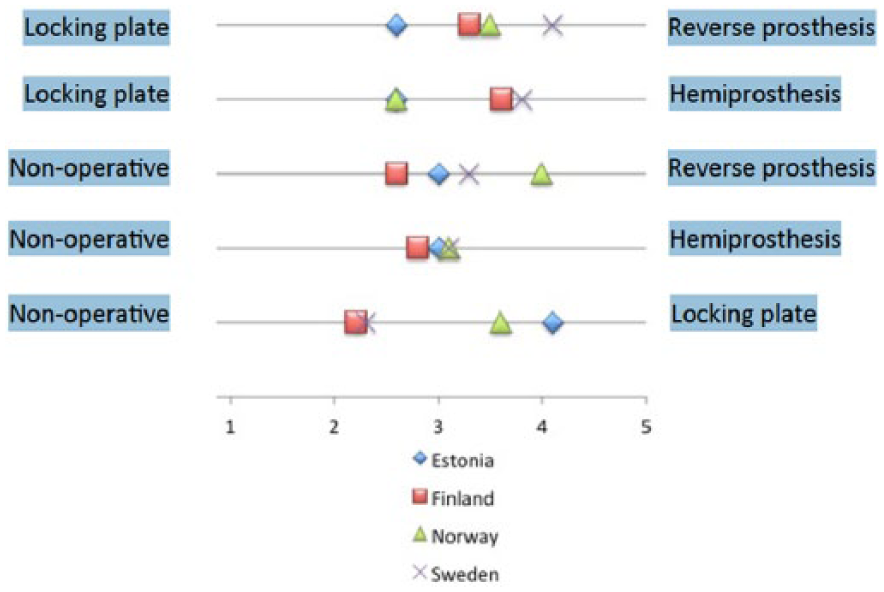
Respondents’ answers plotted on a continuum between imaginary claims.
Discussion
The main finding of our study was that operative treatment is still the most preferred treatment method for displaced proximal humerus fractures in elderly patients. We found differences in hardware selection among the countries. The most preferred treatment was locking plate (35%), followed by hemiprosthesis (27%). Although recent reports suggest that reverse prosthesis has gained in popularity [13, 14], in our study, it was preferred in only 12% of the responses and mostly in Norway, where it was more commonly used than hemiprosthesis. In Estonia, nailing of the proximal humerus fracture was preferred more than in the other countries included in this study. Indications for surgery varied among the countries. This probably reflects the lack of evidence in the literature; clinicians had to make decisions based on their own experience and on traditional practices.
The other main result of our study was that the current practices of post-operative care and rehabilitation did not differ among the Nordic countries and Estonia.
Questionnaire-based surveys are widely used in epidemiological studies [15]. More recently, they have been introduced to investigate the implementation of guidelines or treatment policies; for example, for Achilles rupture, pelvic fracture, and carpal tunnel treatments [16–18]. The biasing effect of surveys could potentially cause uncertainty in the results and needs to be taken into account when conducting or using the results of questionnaire-based research [19]. This bias could emerge from the selection of responders or the proportion of nonresponders.[20] The non-responder bias is considered minimal when the response rate exceeds 70% [21]. In our study, the response rate was 77%.
The present survey was designed to investigate diagnosis, treatment, and post-operative care in three Nordic countries and in Estonia. Questionnaire recipients were either trauma or shoulder surgeons with >5 years of experience who worked in a mid-sized or large hospital. The recipients were selected because they were known to be either shoulder or trauma surgeons in their respective countries. This led to a proportionally smaller number of answers, but it ensured that the coverage of shoulder surgeons was good in each country. However, a limitation of participant selection is that it excludes small-volume hospitals, in which general orthopedic surgeons are responsible for treatment.
The strengths of our study include a good response rate of 77% and the unique set of questions that we used to inquire about treatment preferences for proximal humerus fractures. As the survey was designed to investigate treatment options, it could not be used to analyze quantitative issues regarding the number of patients who underwent specific treatments.
In conclusion, our survey revealed a remarkable uniformity in the current opinion of rehabilitation and non-operative treatment for proximal humerus fractures in the participant countries. The best choice among the different surgical treatments remains unclear, and the results of this survey echoes the lack of consensus over the issue. Our questionnaire revealed that there was heterogeneity in almost all aspects of surgical treatment in the countries that we assessed. Hopefully, tools will be identified that will allow for more secure, evidence-based decision making based on the results of RCTs that are currently enrolling patients [10, 22–24].
Footnotes
Acknowledgements
The authors wish to thank the following doctors who took part in the pilot study and who supplied us with the names of colleagues who are shoulder surgeons: Tore Fjalestad, Jens-Ivar Brox, Hans Berg, Karl-Åke Jansson, Lars Adolfsson, Cecilia Mellstrand-Navarro, Aare Märtson, Kristo Kask, and Tapio Flinkkilä. No funding was received for the preparation of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.