
Abstract
Background/Aim:
Multivisceral resection for advanced tumors can result in prolonged survival but may also increase the risk of postoperative morbidity and mortality. The primary aim of this study was to investigate whether extensive resections increase the severity of postoperative complications.
Materials and Methods:
A retrospective study was conducted between 2009 and 2014 at the Linköping University Hospital surgical department. All patients with a confirmed or presumed malignant disease who underwent a non-standardized surgical procedure requiring a multivisceral resection were included. The primary endpoint was 90-day complications according to the Clavien-Dindo score.
Results:
Forty-eight patients were included, with an age range of 17–77 years. A median of three organs was resected. The most common diagnoses were neuroendocrine tumor (n = 8), gastric cancer (n = 7), and gastrointestinal stromal tumor (n = 6). One patient died during surgery. Complications ⩾ grade 3b according to Clavien-Dindo score occurred in 10 patients. R0 resection was achieved in 32 patients. No correlation was observed between the number of anastomoses, perioperative blood loss, operative time, and complications. Only postoperative blood transfusion was correlated with severe complications (p = 0.046); however, a tendency toward more complications with an increasing number of resected organs was observed (p = 0.06).
Conclusion:
Multivisceral resection can result in R0, potentially curing patients with advanced tumors. Here, no correlation between extensive resections and complications was observed. Only postoperative blood transfusion was correlated with severe complications.
Introduction
In most abdominal tumors, radical resections are of utmost importance for improving long-term survival (1–4). Abdominal tumors may require resection of multiple organs during the same surgical procedure to achieve radicality. Radical resection (R0) can lead to prolonged survival; however, more extensive surgery may also increase the risk of postoperative complications.
Multivisceral resection is an uncommon procedure, except in cases of synchronous colorectal surgery with resection of hepatic metastases and left-sided pancreatectomy and splenectomy. Because the surgical procedures and diagnoses vary, the literature on the subject is rare. Most publications on multivisceral resections are limited to specific diagnosis, and few focus on different malignant diagnoses (5–7).
Multivisceral resection may be performed either due to direct invasion of the tumor in adjacent organs or metastases. The reported morbidity and mortality of multivisceral resection are higher compared with more standardized resection; however, this observation may reflect that tumors for which multivisceral resection is performed are commonly advanced (5–7). Multivisceral resection is occasionally the only possibility for a curative treatment. Multivisceral resection is not uniform due to the wide range of diagnoses and surgical procedures.
Multivisceral resections appear to be performed for a number of solid abdominal tumors. Patient selection is crucial for improving survival without causing severe complications involving short life expectancy. Therefore, we evaluated all multivisceral resections performed at our institution over a 6-year period.
Materials and Methods
In this article, multivisceral resection refers to a non-standardized surgical procedure performed for preoperative malignant diagnosis. Colorectal resection with synchronous resection of hepatic metastases, as well as gastric resection or left-sided pancreatic resection with synchronous splenectomy, was not included in this cohort.
All patients meeting the inclusion criteria between 2009 and 2014 were included. Patients receiving unsuccessful chemotherapy administered to reach surgery and patients found unfit for surgery were not included. A retrospective medical record study was conducted. Variables included age at the time of surgery, the American Society of Anaesthesiologists (ASA) score, preoperative body mass index (BMI), eventual weight loss, preoperative serum albumin value, number of resected organs, number of anastomoses, operation time, perioperative hemorrhage and eventual blood transfusion, intensive care unit (ICU) stay, postoperative complications, length of hospital stay, oncological treatment, diagnosis, radicality, time to recurrence, and survival.
All patients were discussed in a multidisciplinary conference, including Hepato-Pancreato-Biliary (HPB) surgeons, medical oncologists, and radiologist prior to surgery. In patients with a history of cardiac or pulmonary disease or older than 70 years, a preoperative physiological investigation was conducted. Tumor progression during chemotherapy, advanced age, and/or advanced comorbidity with low performance status were considered contraindications for surgery.
All patients had at least a computed tomography (CT) scan of the thorax and abdomen to rule out lung metastases and to ensure that the whole tumor burden was identified prior to surgery. In selected cases, magnetic resonance imaging (MRI) and positron emission tomography (PET) CT were also included in the preoperative workup.
Resections were defined as radical (R0) when all resection margins were free of tumor, regardless of margin width. This definition was used for all diagnoses.
The primary purpose of this study was to evaluate whether extensive resections were associated with increased frequency of severe postoperative complications. A secondary aim was to evaluate radicality, recurrence, and survival. This study was approved by the local ethics committee of the southeast region of Sweden (Dnr 2015/42-31)
Statistics
Data are presented as the median (range), unless otherwise stated. Statistical analysis was performed with Statistica 8.0 (StatSoft Inc., Tulsa, OK, USA). Group proportions were compared with a χ 2 test. p < 0.05 was considered statistically significant.
Results
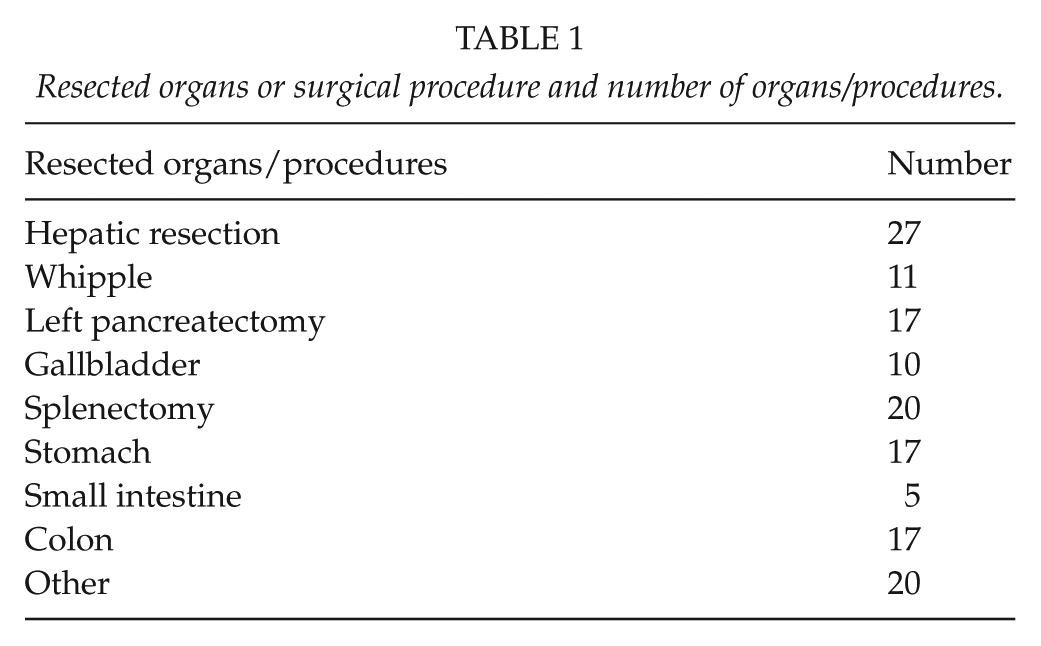
Forty-eight patients were included (21 females and 27 males). The median age at time of surgery was 61 years (17–77 years). Sixteen patients (33%) had ASA score 1, 26 patients (54%) had ASA score 2, and 6 patients (13%) had ASA score 3. Sixteen patients received neoadjuvant oncological treatment, 24 received adjuvant oncological treatment, and 17 patients received no oncological treatment. Fifteen patients underwent liver resection, and 15 patients underwent pancreatic resection, in addition to other resected organs. Seven patients underwent liver resection combined with pancreaticoduodenectomy, and four patients underwent liver resection combined with a left-sided pancreatic resection. One patient underwent hepatic resection, pancreaticoduodenectomy, and left pancreatic resection, with a part of the pancreatic body left intact. Six patients had neither hepatic nor pancreatic resection. The median number of resected organs was three (2–7). The number of resected organs in patients was as follows: two organs (6 patients), three organs (21 patients), four organs (5 patients), five organs (9 patients), six organs (6 patients), and seven organs (1 patient). For details regarding the resected organ and number of patients, see Table 1.
Resected organs or surgical procedure and number of organs/procedures.
The median number of anastomoses was one (0–4). Eleven patients had four anastomoses, and five had three anastomoses. The median operating time was 316 min (115–850 min), and the median perioperative bleeding was 800 mL (25–3800 mL). Twenty-five patients had a blood transfusion, with a median of 4 (1–29) units, including 17 patients who had a perioperative blood transfusion of 2 (1–4) units. Four patients were hemodynamically unstable prior to blood transfusion. The median hemoglobin (Hb) prior to transfusion was 86 g/L (73–96 g/L). The median preoperative Hb for the patients requiring transfusion was 123.5 g/L (95–166 g/L), whereas for the patients managed without transfusion, Hb was 133 g/L (101–156 g/L). Hb decreased by 37.5 g/L (8–70 g/L) from preoperative levels prior to transfusion.
The median preoperative BMI was 24.8 kg/m2 (18.7–37.2 kg/m2). Sixteen patients had a preoperative weight loss of 7 kg (4–22 kg), 25 patients had no weight loss, and these data were unavailable in 7 patients. The median preoperative albumin was 36.5 g/L (22–48 g/L), and 12 patients had albumin levels less than the lower reference value. Eight patients had both preoperative weight loss and albumin less than the lower reference value. One patient had BMI < 20 kg/m2, and this patient did not exhibit preoperative weight loss or low albumin levels.
Nine patients had a postoperative ICU stay, with a median of 3 days (2–9 days). In two cases, the ICU stay was for enhanced observation for patients without organ failure.
Postoperative complications were graded according to Clavien-Dindo score (8). Forty-two patients experienced a postoperative complication, and 25 of those complications were grades 1 and 2. Ten patients had a grade 3b or higher complication, and of those, seven were grade 4. One patient with a large pheochromocytoma of the left adrenal gland with involvement of the right atrium died during surgery. No other postoperative (90 days) deaths were observed. Six patients underwent re-operation: two because of bleeding, one for bowel obstruction, one for septicemia due to intra-abdominal abscess, one for septicemia because of colon perforation, and one due to suspicion of insufficient biliary anastomosis. The median hospital stay was 9.5 days (4–116 days). For details regarding postoperative complications, number of patients with each complication, and grade according to Clavien-Dindo, see Table 2.
Number of complications and grade according to Clavien-Dindo in 48 patients after multivisceral resection.
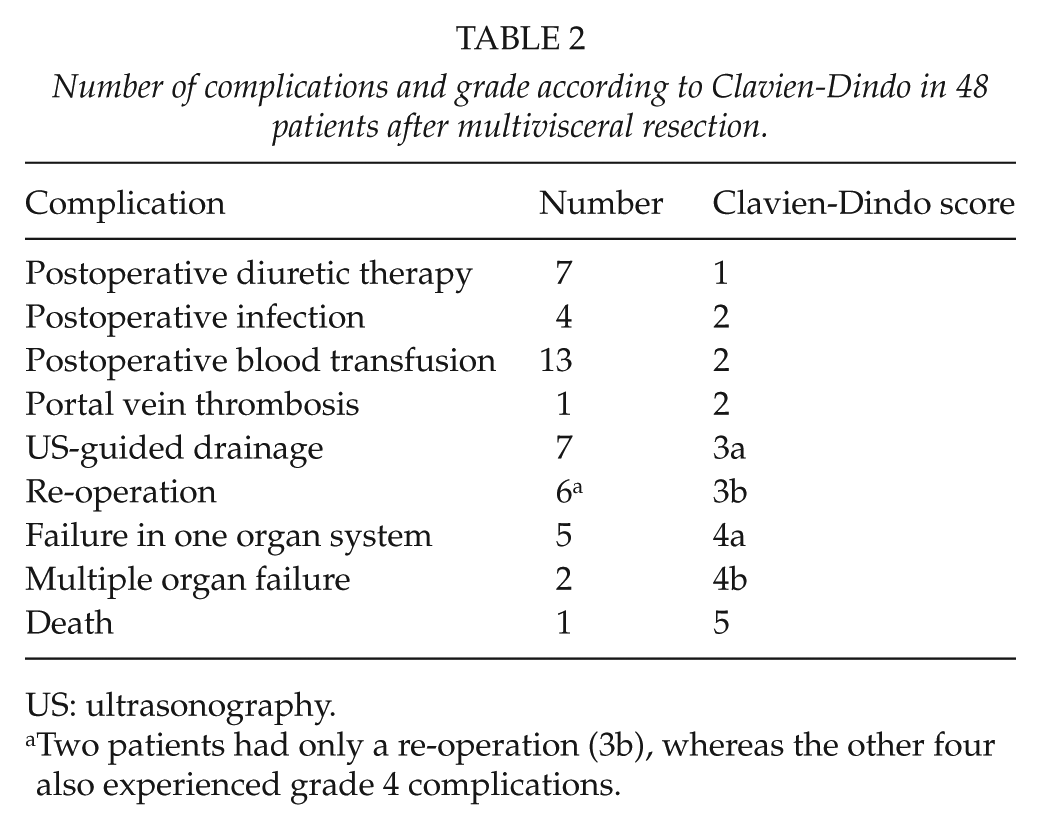
US: ultrasonography.
Two patients had only a re-operation (3b), whereas the other four also experienced grade 4 complications.
Postoperative complications are listed in Table 3.
Factors potentially affecting the postoperative complication rate.
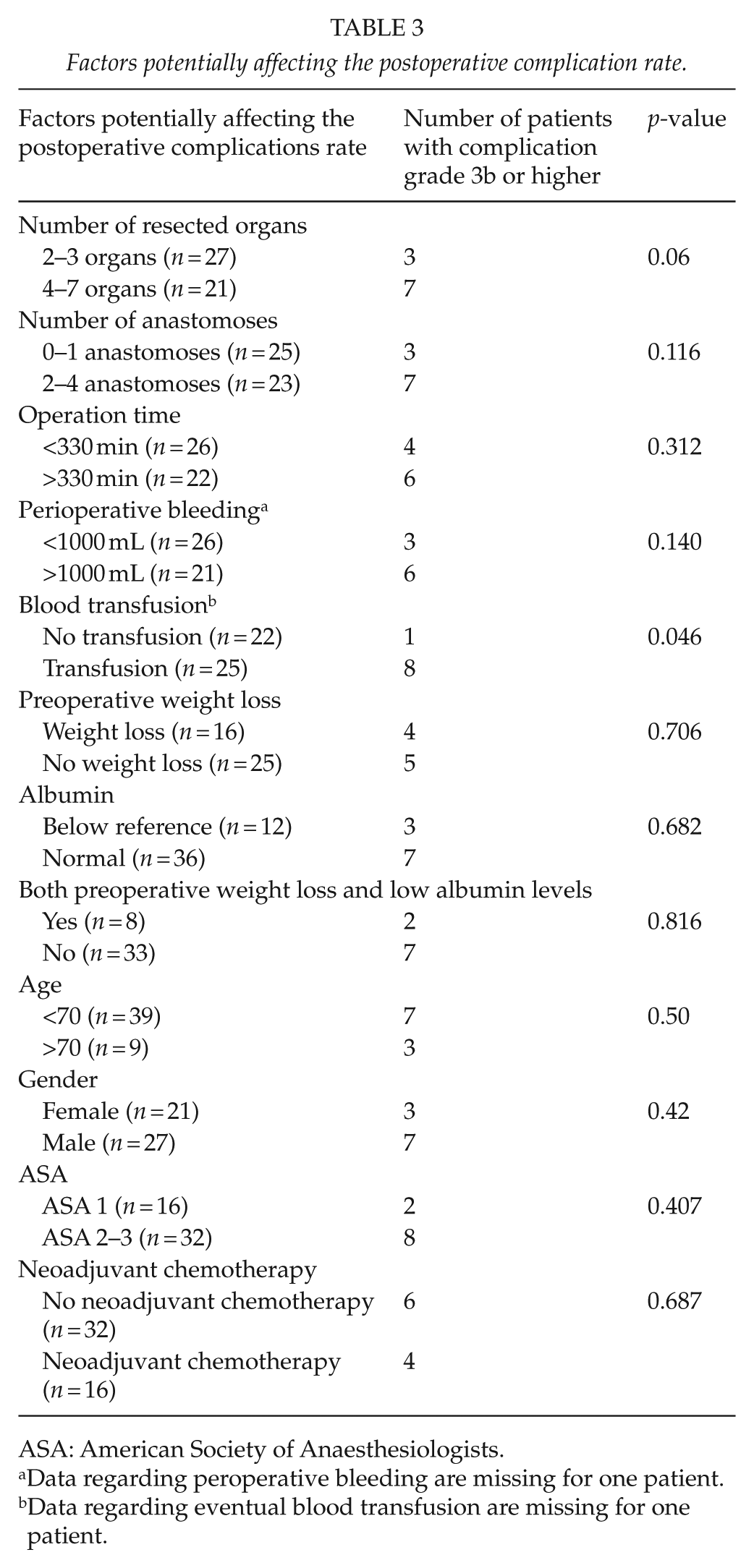
ASA: American Society of Anaesthesiologists.
Data regarding peroperative bleeding are missing for one patient.
Data regarding eventual blood transfusion are missing for one patient.
The difference in complication rate was not significant when comparing patients of different age, gender, or ASA classification. Low nutritional status was not correlated with severe complications. The number of resected organs and number of anastomoses were not significantly correlated with the rate of postoperative complications, although a tendency toward a higher complication rate with more resected organs was observed (p = 0.06). Surgery duration and perioperative bleeding were not significantly correlated with postoperative complications. Neoadjuvant chemotherapy was not correlated with postoperative complications. Intraoperative and postoperative blood transfusions were the only factors significantly correlated with severe complications (⩾3b).
Forty-three patients had final malignant diagnoses. R0 resection was achieved in 32 patients, and 6 patients had R1 resection. In five cases, radicality was difficult to assess or not stated in the pathology report. Five patients were confirmed as benign diagnosis, although the preoperative investigation strongly suggested malignancy. Two patients were diagnosed with chronic cholecystitis. Additionally, ganglioneuroma was diagnosed in one patient, chronic pancreatitis in one patient, and seromucinous cystadenoma originating from the pancreas in one patient.
The most common malignant diagnoses were neuroendocrine tumor (NET) (n = 8), gastric cancer (n = 7), gastrointestinal stromal tumor (GIST) (n = 6), and gallbladder cancer (n = 4). Other diagnoses were locally advanced colorectal cancer and colorectal liver metastases (n = 5), pancreatic cancer (n = 3), sarcoma (n = 3), cholangiocarcinoma (n = 1), duodenal cancer (n = 1), renal cancer (n = 1), pheochromocytoma (n = 1), malignant melanoma (n = 1), lymphoma (n = 1), and one poorly differentiated retroperitoneal carcinoma of unknown origin (n = 1).
Thirty-one patients received oncological treatment. Of those, 7 received neoadjuvant treatment, 15 received adjuvant treatment, and 9 received both neoadjuvant and adjuvant treatment.
Sixteen patients with a malignant diagnosis did not receive adjuvant oncological treatment. Eleven did not receive treatment because of a lack of available effective treatment or indication for treatment, three patients because of postoperative complications with long postoperative recovery, and two patients were determined to not be capable of withstanding oncological therapy, despite uneventful recovery without major complications, because of low performance status. It is unknown whether additional three patients received oncological treatment. The diagnosis of patients for whom effective treatment or indication was missing were as follows: gastric cancer (n = 4), NET (n = 3), gallbladder cancer (n = 2), sarcoma (n = 1), and colorectal cancer (n = 1).
The median follow-up was 33 months (0–71 months), and 19 patients were diagnosed with recurrence during follow-up. The median time of recurrence was 8 months (2–43 months) after surgery and 10 months (3–46 months) after diagnosis. Twelve of the patients with recurrence were deceased at 10 months (1–25 months) after surgery and 13 months (6–39 months) after diagnosis. The estimated 5-year survival was 55%.
In patients with recurrence, 12 had R0 resection and 3 had R1 resection; in 4 cases, radicality was difficult to assess. For the 12 patients with R0 resection, the median time of recurrence was 9 months (2–43 months) after surgery. For the patients with R1 or unknown R status, the median time of recurrence was 8 months (5–42 months) after surgery (p = 0.13) (Figs 1 and 2).
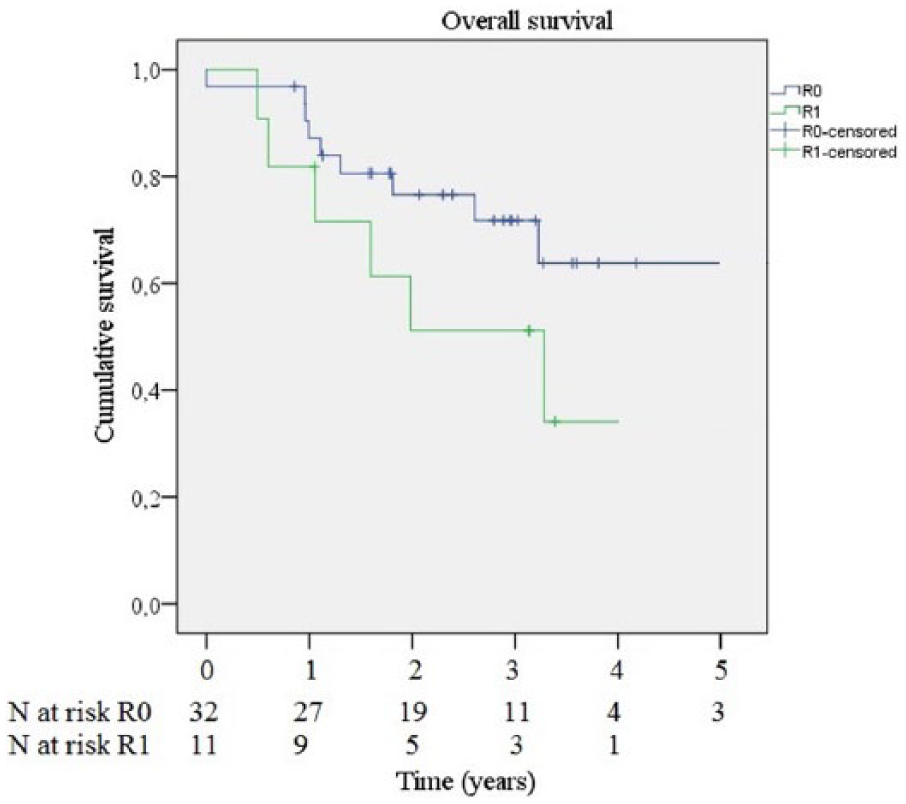
Survival for patients with R0 respective R1 resection.
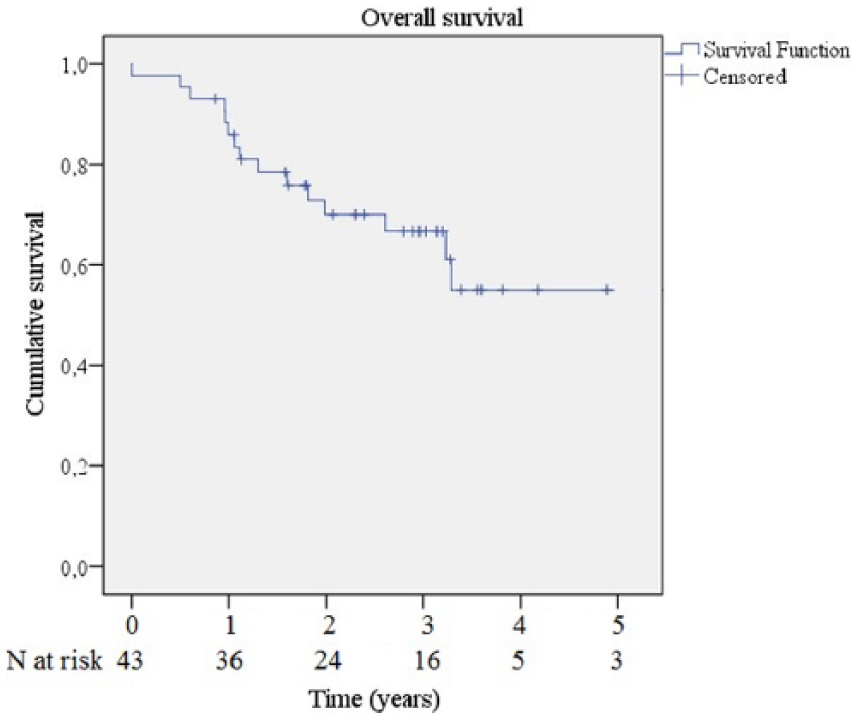
Survival for the all patients with final malignant diagnoses.
Discussion
In this study, 42 patients had a hepatic and/or pancreatic resection. Radicality was achieved in 32 patients. One patient died during surgery, and 42 patients had at least one postoperative complication. Ten patients experienced grade 3b-5 complications according to the Clavien-Dindo score. No significant correlations between postoperative morbidity and the number of resected organs, number of anastomoses, operative time, or perioperative bleeding were observed. However, a tendency toward more severe postoperative complications with ⩾4 resected organs compared with <4 resected organs was observed. Only perioperative and postoperative blood transfusions were significantly correlated with postoperative morbidity. This lack of significance may be related to the limited number of patients included in this study. Nineteen patients had recurrence at 7 months after surgery, and 13 patients were deceased at 16 months after surgery.
Postoperative complications were graded according the Clavien-Dindo score, which has been well established (8). A new classification that may be more accurate is the Comprehensive Complication Index (CCI) in which all complications, not only the most severe, are summarized to calculate a score (9). For this report, we used the more widespread Clavien-Dindo score. Multivisceral resection including hepatic and pancreatic resection are rare procedures, and the diagnoses are diverse, which makes drawing firm conclusions difficult. Similarly, comparisons with other publications are difficult. Because of the diversity of diagnoses, concluding whether specific diagnoses have a higher risk of complications is not possible. Multivisceral resection with either hepatic or pancreatic surgery combined with resection of at least one other organ in the setting of different malignant diagnoses has a reported postoperative mortality up to 7% and a reported complication rate of 59%, of which 33% are described as severe (5). Complications were more common for patients older than 70 years and after pancreatic resections (5). Combined hepatic and pancreatic resection has a reported total postoperative morbidity of up to 46%–47% and postoperative mortality of 4%–18% (6, 7). The highest mortality was observed in the patient group who underwent major hepatectomy combined with pancreatoduodenectomy (PD) (6). The lowest mortality was observed when the hepatic resection was either minor or major and the pancreatic resection was either PD or left pancreatectomy (7). Other studies have shown an increased risk of postoperative complications after pancreaticoduodenectomy compared with left pancreatic resection and after resection of more than two organs, as well as long operation time (10–12). The resections were performed in settings of different malignant diagnoses, and gastroenteropancreatic neuroendocrine tumor (GEP-NET) and biliary tumors were the most common (6, 7). The only significant risk factor for postoperative complications was preoperative chemotherapy. These results differ from our results, in which the only factor significantly associated with increased risk of postoperative complications was postoperative blood transfusion. Previously, data have indicated that postoperative blood transfusion is associated with an increased risk of postoperative complications (13, 14). Additionally, previous data have indicated that a liberal transfusion strategy may reduce postoperative complications after abdominal surgery for solid malignant tumors (15). Another consideration is that a 50% or more reduction in Hb has been associated with an increased frequency of postoperative complications (16). The optimal strategy regarding postoperative blood transfusion has not yet been established.
These differences in findings may be related to the heterogeneity of the study cohorts. However, we found a trending correlation between the number of resected organs and complications, despite our small number of patients. Notably, this cohort was limited in size, and therefore, the ability to reject differences in results between is limited.
Multivisceral resection in gastric cancer has a reported mortality of up to 4% (17), and in combined gastrectomy and pancreaticoduodenectomy, the complication rate has been reported to increase up to 71% (18). Operations for neuroendocrine tumors originating in the pancreas or duodenum have a described total complication rate of 41.7%, with a major complication rate of up to 25%–30% (12, 19). Multivisceral resections in locally advanced and metastatic GIST have reported rates of severe complications (grade 3 or higher) of 10% and 21%, respectively. Postoperative mortality was not reported in this previous paper (20).
The total morbidity rate after HPB surgery has been reported to be 28%, and 19% of reported complications were serious (21). Major postoperative complications have been reported to occur in 15% of patients after hepatectomy and 24% of patients after pancreatic surgery (22). A mortality rate of 3% after HPB surgery has been reported (21), and a 30-day mortality of nearly 1% after hepatic surgery as well as after pancreatic surgery has been observed (22). These results are comparable to those obtained here. After combined hepatic and pancreatic resection, the median disease-free survival (DFS) was 10 months, and after multivisceral resection with hepatic or pancreatic involvement, 3-year overall survival (OS) and DFS were 79% and 68%, respectively (5, 6).
Here, R0 was achieved in 32 patients. The reported R0 frequency varies between 64% and 98%. However, the diagnoses and resections greatly vary, making meaningful comparisons difficult (12, 17, 20, 23–25). In this study, the estimated 5-year OS for the whole cohort with malignant diagnoses was 55%. Although not significant, a tendency toward earlier recurrences in patients with R1 resections was observed. Our study supports the use of multivisceral resection in selected patients with locally advanced tumors to achieve R0 resections. An important limitation of this conclusion is the lack of information about patients receiving chemotherapy who did not reach surgery, making an intention to treat analysis impossible.
Conclusion
Multivisceral resection can be performed with a high R0 rate at the cost of increased total morbidity. However, serious complications and mortality are only marginally increased and are comparable to other branches of HPB surgery. Importantly, for this special category of patients, surgery is the only treatment with curative potential. Therefore, these results indicate that multivisceral resections should be considered for patients fit for surgery with advanced tumors. Achieving R0 resection is of utmost importance for patients with advanced tumors.
Footnotes
Acknowledgements
The results in this article have been previously presented as a poster at a Swedish surgery conference in August 2014 and at an E-AHPBA conference in February 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.