
Abstract
Background and Aims:
The aim of the present study was to determine whether usage of mesh with larger pores, compared with mesh with smaller pores, would result in a decreased rate of chronic pain at 3-year follow-up. According to earlier published short-term results, differences in mesh pore size do not influence the rate of chronic pain.
Material and Methods:
The patients were randomized into two study groups for which meshes with similar weight but different pore size were used: the UM group received Ultrapro mesh (pore size 3–4 mm) and the OM group received Optilene LP mesh (pore size 1 mm). Pain scores were measured on a visual analog scale. The feeling of a foreign body was a yes-or-no question.
Results:
A total of 65 patients in the UM group and 63 patients in the OM group were included in analysis. Of the patients, 33.9% in the UM group and 15.9% in the OM group reported having experienced pain during different activities at 3-year follow-up (P = 0.025). Comparison with the results of 6-month follow-up (46.3% in the UM group, 34.3% in the OM group) showed that the rate of chronic pain had decreased significantly in the OM group (P = 0.009) but not in the UM group (P = 0.113). The feeling of a foreign body in the inguinal region was experienced by 23.1% of the patients in the UM group and by 15.9% in the OM group (P = 0.375). There was one hernia recurrence in the OM group. Severe preoperative pain and younger age were identified as risk factors for development of chronic pain.
Conclusions:
Mesh with larger pores, compared with mesh with smaller pores, has no advantages in reducing the rate of chronic pain. We speculate that the reason for the higher rate of chronic pain in the study group where the mesh with larger pores was used might have been the different composition of the meshes at implantation. Also, it is possible as development of chronic pain after inguinal hernia repair is multifactorial, we failed to find a plausible explanation for this difference. Low recurrence rates were achieved with both meshes used in our study.
Keywords
Introduction
Considering that the lifetime risk for inguinal hernia operation is estimated at 27% for men and 3% for women (1), which results in a vast number of patients undergoing inguinal hernia repair, even rare adverse events would be of great impact (2).
The most common complication after widely used mesh repair in inguinal hernia surgery is chronic pain, which may occur in 51.6% of patients (3). This can have major influence on the patients’ quality of life, as well as carry serious socioeconomic impacts. Although nerve damage may be the most important pathogenic factor for development of chronic pain (4), there is also association between the rate of chronic pain and the type of mesh used for hernia repair. According to the European Hernia Society guidelines on the treatment of inguinal hernia, the parameters of an ideal mesh are not known (5). However, as prevention of chronic postoperative inguinal pain is considered the primary outcome of elective inguinal hernia surgery (6), different mesh characteristics should be studied in order to identify an “ideal” mesh.
Different mesh characteristics have been studied in order to identify a mesh whose usage would result in lower rates of chronic pain. Among these characteristics, mesh weight has probably gained the most attention. Although several studies have compared meshes with different pore sizes, these meshes differed not only in pore size but also in weight (3, 7, 8). However, according to the short-term results of this study, differences in mesh pore size do not influence the rate of chronic pain (9).
The primary aim of our research, whose short-term results have been published previously (9), was to determine whether usage of mesh with larger pores, compared with mesh with smaller pores, would result in a decreased rate of chronic pain after open inguinal hernia repair at 6-month follow-up. The secondary aim of the present study was to evaluate the rate of chronic pain and foreign body feeling at 3-year follow-up, risk factors for development of chronic pain, and hernia recurrence.
Material and Methods
All patients aged 18 years or older, who had undergone an elective inguinal hernia repair from January 2011 to April 2012, were eligible to participate in the study. The inclusion criteria were age ⩾ 18 years, unilateral primary reducible inguinal hernia, elective operation, and consent to participate in the study. The exclusion criteria were age < 18 years, irreducible, strangulated or recurrent hernia, inability to understand the questionnaire, and unwillingness to participate in the study. The study was approved by the Ethics Committee of the University of Tartu (Reference number: 198T-3; Trial registration number Registration number: NCT02500056; Agency: ClinicalTrials.gov).
The patients were randomized into one of two study groups following restricted randomization procedures. Randomization was done using a set of sealed opaque envelopes, which were all prepared by one researcher (C. N.) before the beginning of the study. The envelopes were kept in an arranged location in the operating room. Before operation, the surgeon took randomly a sealed envelope that contained a label of mesh. The patients were blinded to which mesh they received. In the UM group, the patients received Ultrapro mesh; in the OM group, the patients received Optilene LP mesh. Ultrapro is a lightweight partially absorbable mesh consisting of polypropylene and polyglecaprone with a weight of 28 g/m2 and a pore size of 3–4 mm (Ethicon, Hamburg, Germany). Optilene LP mesh is a monofilament polypropylene lightweight mesh with a weight of 36 g/m2 and a pore size of 1 mm (B. Braun, Rubi, Spain). A mesh with measurements 4.5 × 10 cm was applied; Optilene LP mesh was commercially preshaped and Ultrapro mesh was shaped by the surgeon during operation using a stencil. The polypropylene 2-0 suture material was used for mesh implantation. A tension-free repair using the modified Lichtenstein technique was performed in both study groups. All nerves in the inguinal canal were identified and preserved when possible.
The preoperative and postoperative data were documented using standardized forms. The data included demographic data, body mass index, duration of the disease, method of anesthesia, type of hernia (direct or indirect), size of hernia, hernial sac handling, duration of operation, length of hospital stay, and experience of the surgeon (trainee or staff surgeon).
The primary outcome measure was the rate of chronic groin pain, taking into account all patients who reported pain during different activities (yes-or-no questions). Foreign body feeling was the secondary endpoint.
Follow-up examination was performed 3 years after the operation. The pain questionnaire included questions about pain at rest, on coughing, when rising from lying to sitting, and during physical effort and exercise (all yes-or-no questions). When the answers to these questions were positive, pain scores were measured on a visual analog scale (VAS) ranging from 0 mm (no pain) to 100 mm (worst imaginable pain). A score of 0 was defined as no pain. A score of less than 10 was graded as mild pain, a score of 10–50 as moderate pain, and a score of more than 50 as severe pain. Such gradation has been used in earlier similar studies (10). The analysis of the distribution of pain severity was based on the highest score on the VAS during different activities (at rest, on coughing, when rising from lying to sitting, and during physical effort and exercise). The patients were also asked whether pain influenced their everyday activities. Postoperative analgesic consumption was recorded as well. Foreign body feeling was registered as a yes-or-no question. All patients underwent a clinical examination for any evidence of hernia recurrence. The results were compared with earlier short-term results (9).
Statistical Analysis
In our previous study, the rate of chronic pain in the Optilene LP group was 47.8% (11). In a study of Śmietański et al. (12), the rate of pain (VAS > 0) after inguinal hernia repair with Ultrapro mesh was 21.2%. Based on our previous study and aiming at a difference of about 27% in the rate of chronic pain at 6-month follow-up (primary aim) between the study groups (48% for OM vs 21% for UM) according to Fisher’s exact test at the 5% significance level (power 80%), it was clear that sample size had to be 56 in both study groups. Assuming a dropout rate of 5%, a minimum of 118 participants were needed for the study.
The patients who were lost during follow-up were excluded from the analysis; only the patients who completed the questionnaire were included.
The data were analyzed using the STATISTICA version 12.0 software package (StatSoft, Tulsa, Oklahoma) (under Windows XP Professional). To test the rate of chronic pain for the two study groups at 3-year follow-up, Fisher’s exact test was used. Also, the rate of foreign body feeling was evaluated using Fisher’s exact test. To describe associations for the binary outcome variables, risk ratios with 95% confidence intervals (CIs) are presented. McNemar’s test was used to assess paired observations on a dichotomous outcome at 6-month and 3-year follow-up. A logistic regression model was used to control for confounding variables (adjusting for sex, age group, that is, age < 65 versus ⩾65 years, severe preoperative pain, and severe early postoperative pain). All statistical tests were two-sided and P ⩽ 0.05 was considered significant.
Results
A total of 143 patients were randomized: 73 to the UM group and 70 to the OM group. Fifteen patients were lost during follow-up (dropout rate 10.5%): 4 patients died (the causes of death were all non-hernia surgery related), 10 patients did not attend their follow-up visits, and 1 patient in the OM group developed a recurrent hernia (all dropouts were excluded from the analysis). There was no significant difference in the dropout rate between the two study groups (P = 0.999). A total of 65 patients in the UM group and 63 patients in the OM group were investigated 3 years after the operation (Fig. 1).
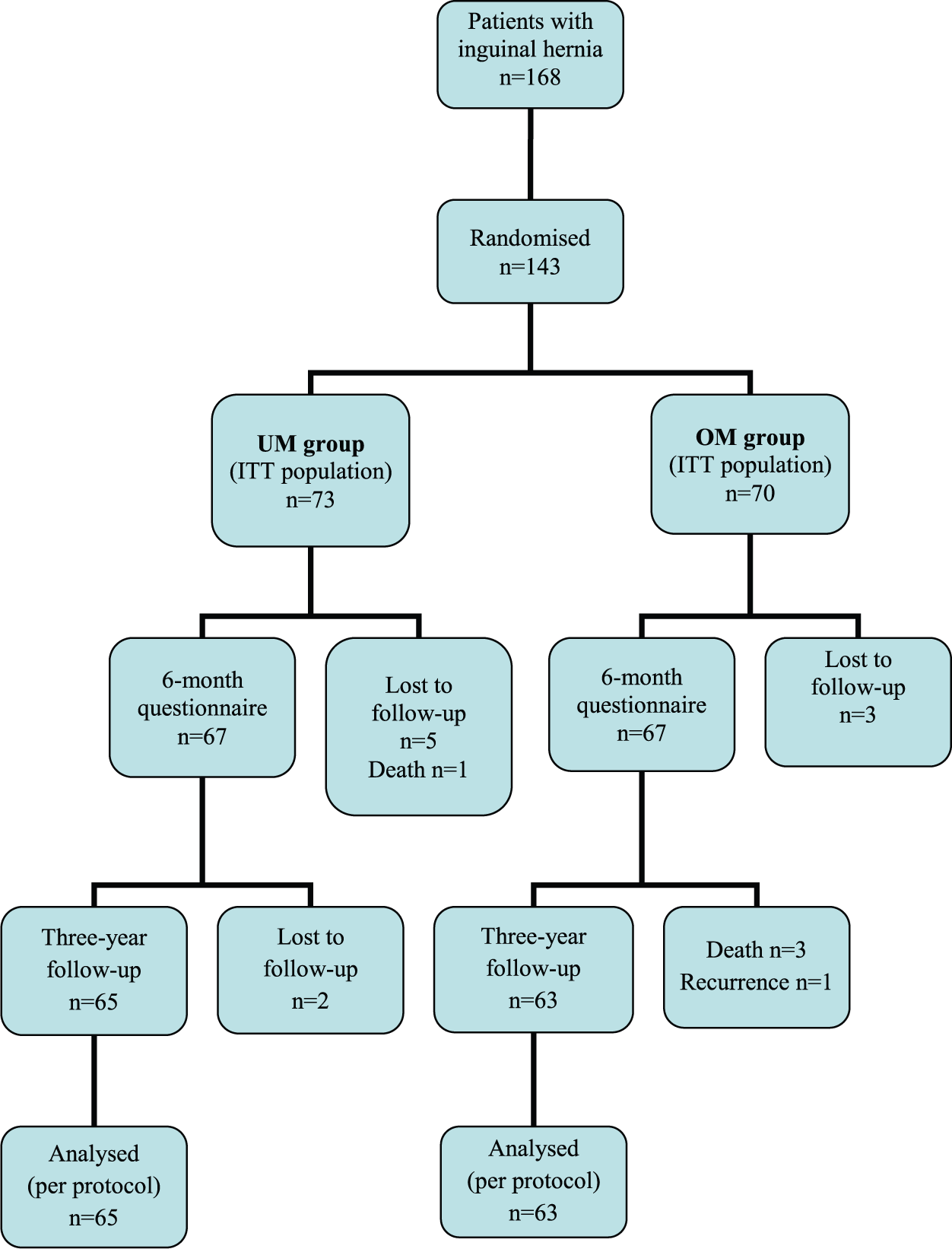
Study flow chart.
The preoperative data, the intraoperative data, and the short-term results have been published previously (9). Of the patients, 33.9% (22/65) in the UM group and 15.9% (10/63) in the OM group reported having experienced any pain during different activities at 3-year follow-up (P = 0.025). The risk ratio for chronic pain at 3-year follow-up was 2.13 (95% CI = 1.13–4.14). Comparison with the results of 6-month follow-up (46.3% in the UM group, 34.3% in the OM group) showed that the rate of chronic pain had decreased significantly in the OM group (P = 0.009) but not in the UM group (P = 0.113). Positive answers to the pain questionnaire regarding different activities at 3-year follow-up are presented in Table 1. In the UM group, 48.4% (15/31) of the patients who reported chronic pain at 6-month follow-up had no pain at 3-year follow-up, and 17.7% (6/34) who had no chronic pain at 6-month follow-up developed it by the third postoperative year (P = 0.078). The respective results for the OM group were 69.6% (16/23) and 7.5% (3/40) (P = 0.004).
Positive answers to the pain questionnaire at 3-year follow-up after inguinal hernioplasty.
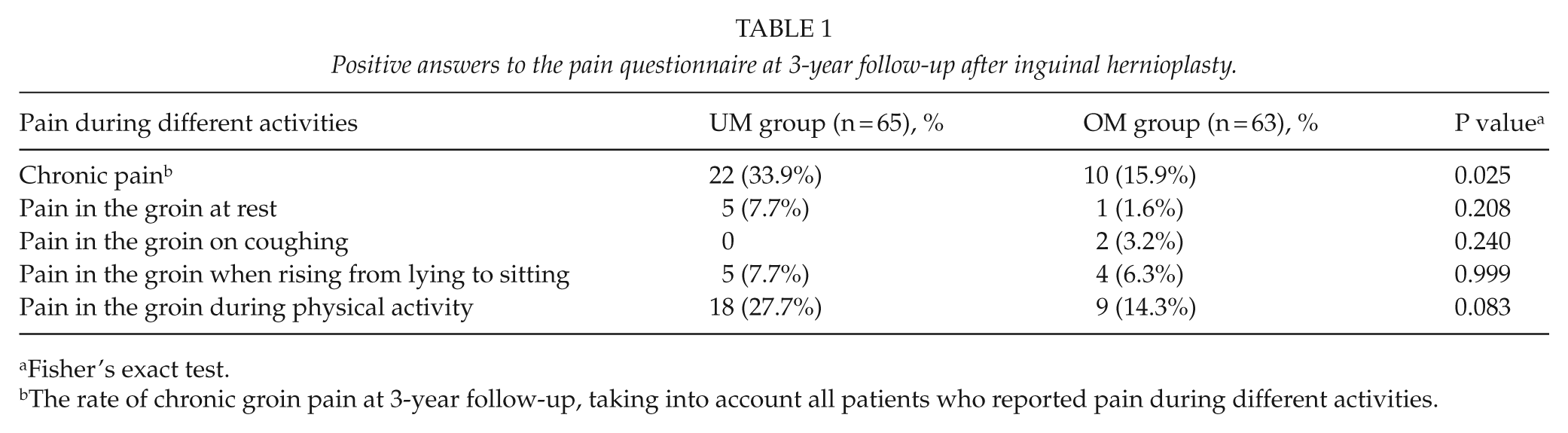
Fisher’s exact test.
The rate of chronic groin pain at 3-year follow-up, taking into account all patients who reported pain during different activities.
The mean VAS scores based on the highest score for different activities were 31.6 in the UM group and 38.0 in the OM group (P = 0.410). The results of distribution of pain severity in the UM group and in the OM group are presented in Table 2.
Distribution of pain severity based on the highest pain score on the visual analog scale during different activities at 3-year follow-up.
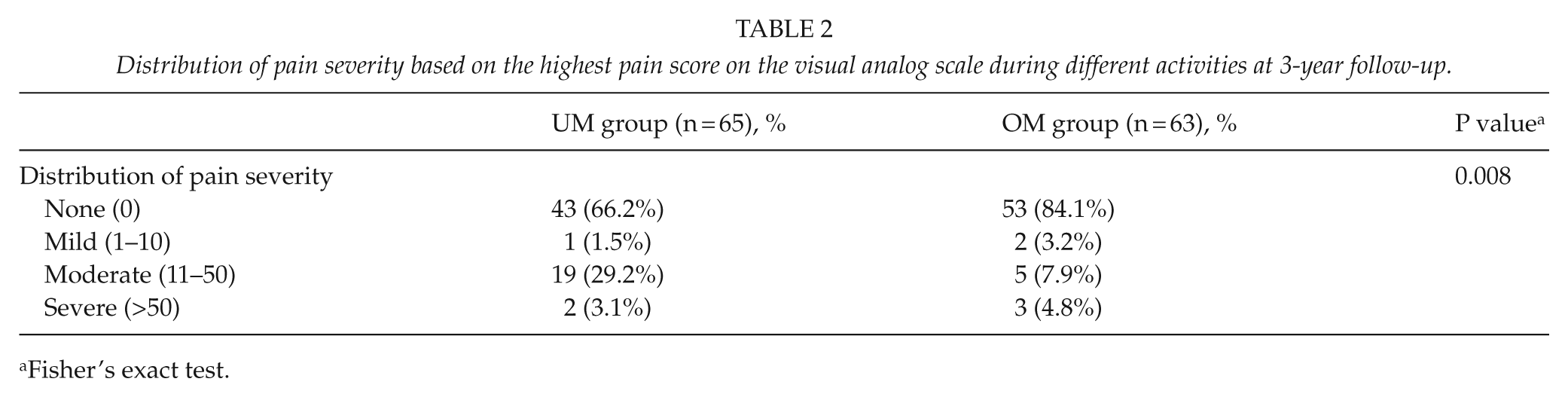
Fisher’s exact test.
At 3-year follow-up, one patient (1.5%) in the UM group and two patients (3.2%) in the OM group used analgesics for groin pain (P = 0.616). One patient (1.5%) in the UM group and two patients (3.2%) in the OM group had pain at the operation site at 3-year follow-up, which influenced their daily activities (P = 0.616). Among the latter, one patient in the UM group and one patient in the OM group used analgesics for inguinal pain.
The feeling of a foreign body in the inguinal region was experienced by 23.1% (15/65) of the patients in the UM group and by 15.9% (10/63) in the OM group (P = 0.375). The risk ratio for foreign body feeling was 1.45 (95% CI = 0.72–2.97). In the UM group, 64.5% (20/31) of the patients who reported foreign body feeling at 6-month follow-up had no foreign body feeling at 3-year follow-up, and 11.8% (4/34) of the patients who had no foreign body feeling at 6-month follow-up developed it by the third postoperative year (P = 0.002). The respective results for the OM group were 63.2% (12/19) and 6.8% (3/44) (P = 0.035).
Of all studied patients under age 65, 30.4% (24/79) reported chronic pain at 3-year follow-up. The corresponding result for patients aged 65 or more was 16.3% (8/49) (P = 0.094).
At 3-year follow-up, 48.6% (17/35) of all studied patients who had had severe pain preoperatively reported pain during different activities, and 16.1% (15/93) of the patients who had not had severe preoperative pain (VAS score 0–50) reported pain during different activities (P = 0.0004).
Of all studied patients, 34.3% (12/35) who had severe pain on the seventh postoperative day also had pain at 3-year follow-up. However, 21.5% (20/93) of the patients who did not report severe pain on the seventh postoperative day had pain during different activities (P = 0.170).
However, when using logistic regression, we found that besides the type of mesh, also age < 65 years (odds ratio (OR) = 3.21; 95% CI = 1.25–8.25) and severe preoperative pain (OR = 6.21; 95% CI = 2.40–16.09) were significant risk factors for development of chronic pain.
Discussion
When companies started to produce a variety of prosthetics, the weight of meshes became the most widely discussed topic in hernia surgery, and the goal of all mesh developers was to produce lighter meshes in order to improve biocompatibility (13). However, in their experimental study, Weyhe et al. (14) reported that the main determinant of biocompatibility was the pore size of mesh rather than the amount implanted. The inflammatory intensity of foreign body reaction depends on the porosity of meshes (15, 16). According to Klinge et al. (16), increased pore size had a major impact on the biological response. In the case of small pores, a dense scar plate will develop around the entire mesh (15, 16) and the extent of foreign body reaction does not permit the ingrowth of the local tissue (16). Larger pores are filled with the local fat tissue forming a thin scar network, which results in the proper elasticity of the implant (15, 16). Large pores will also preserve elasticity and hamper the bridging of inflammation across the pores (16). For polypropylene meshes, 1000 µm is the least distance that prevents the bridging of the scar tissue, which then fills out the entire pore (17). Klinge and Klosterhalfen (18) have even classified the meshes used for hernia repair, based mainly on porosity.
In a clinical study, O’Dwyer et al. (3) reported significantly lower rates of chronic pain for the study group where a mesh with larger pores was used. Similarly, in a study of Bringman et al. (7), the usage of mesh with larger pores resulted in less pain on examination and when rising from lying to sitting at 3-year follow-up. However, contrary to our study, in the above studies, the meshes used differed not only in pore size but also in weight. Surprisingly, in our study, significantly more patients reported pain at 3-year follow-up in the study group where the mesh with larger pores was used. One explanation for this could be the different composition of the meshes at implantation. In an experimental study of Orenstein et al. (19), a mesh of polypropylene and polyglecaprone induced significant chronic inflammatory response. However, considering the fact that the absorbable component of Ultrapro, polyglecaprone, is fully absorbed during 84–140 days (20), it is therefore unlikely that the different composition of the meshes is the only reason why more patients reported pain in the UM group.
According to the European Hernia Society guidelines on treatment of inguinal hernia in adult patients, the risk factors for development of chronic pain are preoperative pain and severe early postoperative pain. It has also been found that the risk of chronic pain after hernia surgery decreases with age (5).
Younger age was a risk factor for development of chronic pain also in other studies (21, 22) and in a systematic review of Nienhuijs et al. (23). This can be explained by the fact that younger people are usually more active (24). According to the short-term results of the present study (9), younger age was a significant risk factor for development of chronic pain, too. At 3-year follow-up, we noted only a trend for less pain among patients aged 65 years or older. However, logistic regression analysis confirmed that younger age is a strong risk factor for development of chronic pain. Poobalan et al. (21) and Wright et al. (25) have reported that preoperative pain increases the risk for development of chronic pain. As in our study the majority of the patients had pain preoperatively, we decided to evaluate whether severe preoperative pain (VAS score > 50) was a risk factor for development of chronic pain. According to our short-term results (9), severe preoperative pain turned out to be a risk factor for development of chronic pain also at 3-year follow-up. Similarly, in our study comparing the weight of meshes, severe preoperative pain was a significant risk factor for development of chronic pain at 3-year follow-up (26). Contrary to the study of Callesen et al. (27), where the rate of chronic pain at 1-year follow-up was higher among patients who had a high pain score 1 week after operation, severe early postoperative pain did not predict the development of chronic pain in our study.
Although the requirements for an ideal mesh in hernia surgery are known, a mesh satisfying all these requirements has not yet been found (17). As each product has its own unique advantages and disadvantages, therefore, one product might never address the wide spectrum of inguinal hernia disease (28). However, other mesh parameters, particularly their combinations, should still be explored.
A limitation of the present study might be the fact that we could not make any conclusions about nerve damage as we did not record whether the nerves in the inguinal canal were sacrificed. Also, as development of chronic pain after hernia repair might be multifactorial, it is difficult to compare different meshes and hence the true reasons for development of chronic pain might be very hard to clarify.
In summary, our study could not demonstrate an advantage of larger mesh pores related to long-term postoperative chronic pain or foreign body feeling. We speculate that the reason for the higher rate of chronic pain in the study group where the mesh with larger pores was used might have been the different composition of the meshes at implantation. Also, as development of chronic pain after inguinal hernia repair is multifactorial, we failed to find a plausible explanation for this difference. Considering that younger age is a strong risk factor for development of chronic pain, inguinal hernia repair could perhaps be postponed in asymptomatic cases among younger patients until they develop complaints. Low recurrence rates were achieved with both meshes used in our study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.