
Abstract
Background and Aims:
There remains a controversy between unreamed intramedullary nailing and external fixation to treat Gustilo grade IIIB tibial fractures. To evaluate the comparative effectiveness and safeness of both methods for this type of fracture, we performed this meta-analysis.
Materials and Methods:
Relevant original studies were searched in MEDLINE, EMBASE, China National Knowledge Infrastructure, and Cochrane Central Database (all through February 2014). Studies included in this meta-analysis had to compare the effectiveness or complications and provided sufficient data of interest. The patients treated by both methods were similar statistically in demography and injury mechanism. The Stata 11.0 was used to analyze all data.
Results:
Six studies involving 163 participants were included. Unreamed intramedullary nailing was associated with reduced time to union (standardized mean difference, −1.14; 95% confidence interval, −2.04 to −0.24) and lower rates of superficial infection (odds ratio: 0.39; 95% confidence interval: 0.17–0.87) and malunion (odds ratio: 0.27; 95% confidence interval: 0.09–0.78). However, there were no significant differences in other adverse events including delayed union, non-union, deep infection, and fixation failure.
Conclusion:
The existing evidence supports unreamed intramedullary nailing to be a better method for treating Gustilo grade IIIB tibial fractures, and this might aid in the management of this sever injury.
Keywords
Introduction
The open tibia fracture is the most common open long bone fracture, and 29.6% of them were Gustilo IIIB fractures (1). Clinically, it remains a challenge for orthopedic and plastic surgeons to treat open tibia fractures due to frequent multiple injuries (2, 3). As the two commonly used methods for Gustilo grade IIIB tibial fractures, unreamed intramedullary nailing (UIN) and external fixation (EF) are still controversial. Some surgeons suggested UIN advantage in early weight-bearing, fewer incidences of infections, and reduced malalignment (4–7). However, some disadvantages had been identified in the literature including increased risk of nail failure and spreading of infections through the medullary canal (4). Similarly, positive and negative outcomes were also observed in EFs. Consequently, these frequently place the surgeons in a dilemma when making a decision on which method is better in treating Gustilo grade IIIB tibial fractures.
Some original studies have been conducted to solve this debate, but they were limited by the smaller sample size and the inclusion of fewer observational items (7–10). Fang et al. (11) undertook a meta-analysis to compare the two methods in treating Gustilo III tibial fractures. In his study, he suggested a meta-analysis for more detailed classification need to be made due to great difference in subgroups of Gustilo grade III fractures, such as IIIB fractures. Dervin (12) first conducted a comparative study in treating Gustilo IIIB fractures, and he found the potential of meta-analysis although without any significant difference observed. In his study, only two studies were included, and this might result in certain biases and heterogeneity. Subsequently, several relevant original studies were performed, but the reported results were inconsistent, which guaranteed sufficient articles for this updated meta-analysis.
Considering the above limitations, this study was accordingly performed to reflect the current status of both therapeutic methods for treating Gustilo grade IIIB tibial fractures. The relevant observed variables involve delayed union, non-union, malunion, time to union, superficial infection, deep infection, and fixation failure.
Materials and Methods
Search Strategy
We searched for relevant citations in MEDLINE, EMBASE, Cochrane central database, and China National Knowledge Infrastructure (CNKI) (all through June 2014) comparing the results between the UIN and EF for treating Gustilo IIIB fractures.The main key words were as follows: “Gustilo III” or “tibial fractures” or “Gustilo IIIB fractures” AND “treatment” AND “intramedullary nailing” AND “external fixators” AND “complications” or “effectiveness” or “results” or “outcome.” Also, a manual search of references in the identified articles and systematic reviews was performed for additional inclusion.
Inclusion Criteria
Two reviewers (F.Z. and Y.T.) independently evaluated the titles and abstracts of the identified papers. Only full-text articles without language restriction were included in this meta-analysis. The inclusion criteria were as follows: (1) randomized or case-control or cohort studies comparing the results between UIN and EF for treating Grade IIIB tibial fractures; (2) intramedullary nailing was restricted to be unreamed but without restriction for EF; (3) participants receiving UIN and EF were similar statistically in age, gender, or mechanism; (4) at least one of the comparing results of interests must be provided in the original study (e.g. infection, malunion, delayed union, fixation failure); (5) sufficient data were published for estimating an odds ratio (OR) or standardized mean difference (SMD) with 95% confidence intervals (CIs). Any disagreement was resolved by discussion and consensus.
Quality Assessment and Data Extraction
As the included studies varied in methodology, including observational or experimental and prospective or retrospective, no precise scale could be performed to assess their quality. This problem was solved by a tool recommended in the Cochrane Handbook 5.1.0, as “The Cochrane Collaboration’s tool for assessing risk of bias,” which was performed by Fang et al. (11) to solve a similar problem. This scale includes six major concerns as bias sources including sequence generation, allocation concealment, blinding, incomplete data, selective outcome reporting, and others. All the data were carefully extracted from all eligible studies independently by the same two reviewers. The following information was extracted from each study: first author’s name, publication year, country, patients’ age and gender, follow-up duration, definitions and numbers of UIN and EF groups, and numbers of citations for each observed item.
Statistical Analysis
We estimated ORs and corresponding 95% CIs and pooled across studies to assess the difference between both methods with a p < 0.05 as significance. Heterogeneity between studies was tested by Q-test statistics with significance set at p < 0.10 (13). The I2 statistics were used as a second measure of heterogeneity, with I2 more than 50% indicating significant inconsistency. A random-effects model was used to calculate pooled ORs in the case of significant heterogeneity (p < 0.10 or I2 > 50%); otherwise, a fixed-effects model was used (14). The outcome of meta-analysis for variables was summarized graphically using a forest plot. Publication bias was not assessed due to the fewer studies included for any variable. If necessary, a sensitivity analysis by excluding outlier studies was conducted to investigate the causes for heterogeneity. All analyses were performed using the software Stata 11.0 (Stata Corporation, College Station, TX).
Results
A total of 427 relevant citations were originally searched as candidates for the meta-analysis; 297 were excluded due to inappropriate types (e.g. abstracts, reduplicative, letters, and meeting reports), 89 were excluded for not meeting the specific therapeutic methods according to criteria, 27 were excluded for reporting results of no interest, 8 were excluded as they did not provide sufficient data for meta-analysis, and 6 studies were identified to be eligible and included in this meta-analysis. The whole research procedure is presented by a flow diagram (Supplementary Fig. 1).
All the included articles were comparative, and of them, five were published in English and one in Chinese with publication time from 1994 to 2007. Participants treated by both methods in each of the studies were similar statistically in age, gender, or injury mechanism. A summary of basic characteristics is listed in Table 1. The detailed information of quality assessment for included studies is presented in Supplementary Table 2.
Detailed information on the basic characteristics of the six included studies and participants.
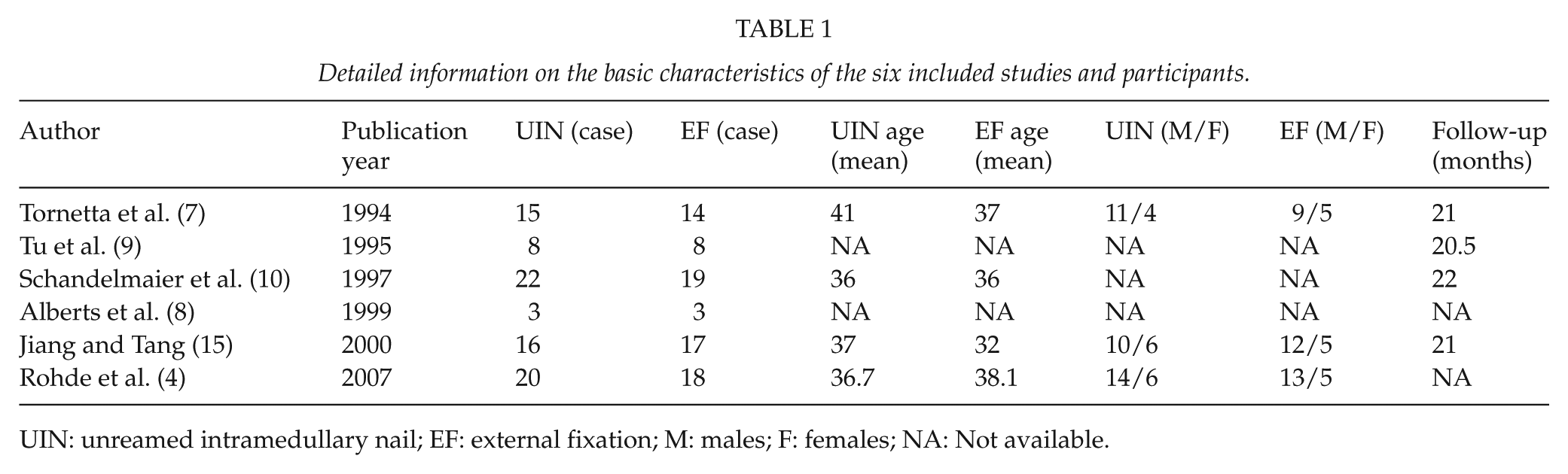
UIN: unreamed intramedullary nail; EF: external fixation; M: males; F: females; NA: Not available.
The time to union was substantially different between the two methods, namely, a consistently reduced healing time of approximately 6 weeks (26.3 versus 32.5) in UINs. Fig. 1 depicts this result by charting the mean result of each study with 95% CI and the pooled means and 95% CI limits in the lower part of the chart. After sensitivity analysis by excluding the outlier study, the result did not change.
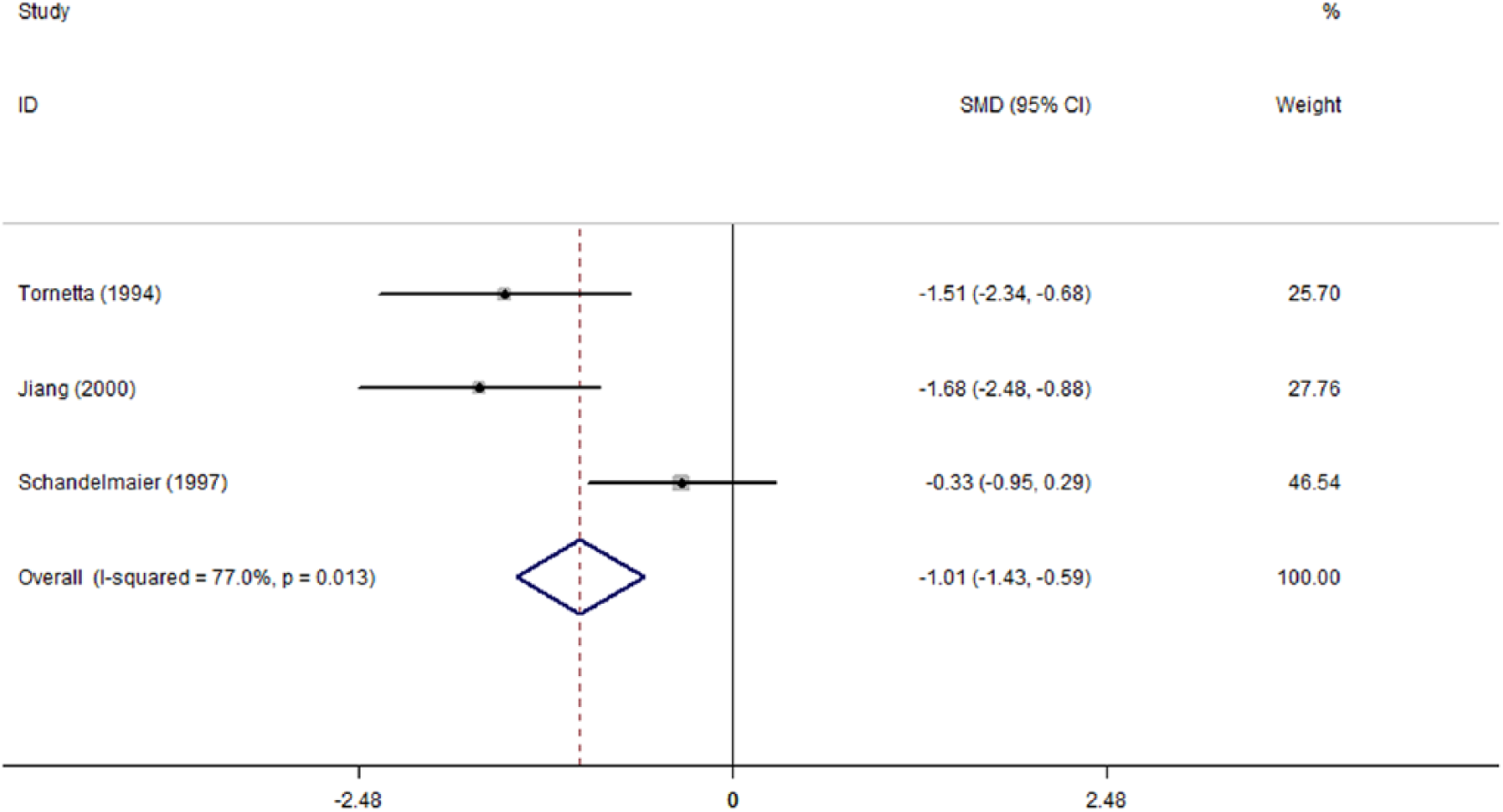
Forest plot of SMD with 95% CI for time to union.
Four studies reported the delayed union rate, with an overall rate of 8.2% (5/61) in UIN and 17.2% (10/58) in EF. EF appears to be associated with a higher delayed union rate than UIN, but it did not approach significance (OR: 2.26; 95% CI: 0.73–7.00) without any heterogeneity (p = 0.794; I2 = 0) (Fig. 2). Thus, the overall delayed union rate was calculated using a fixed-effects model. Similar to the delayed union, no significant difference was observed in non-union rate between both methods (OR: 0.68; 95% CI: 0.22–2.11), although with a seemingly discrepancy of 13.8% versus 9.3%. The detailed result is presented by a forest plot (Fig. 3).
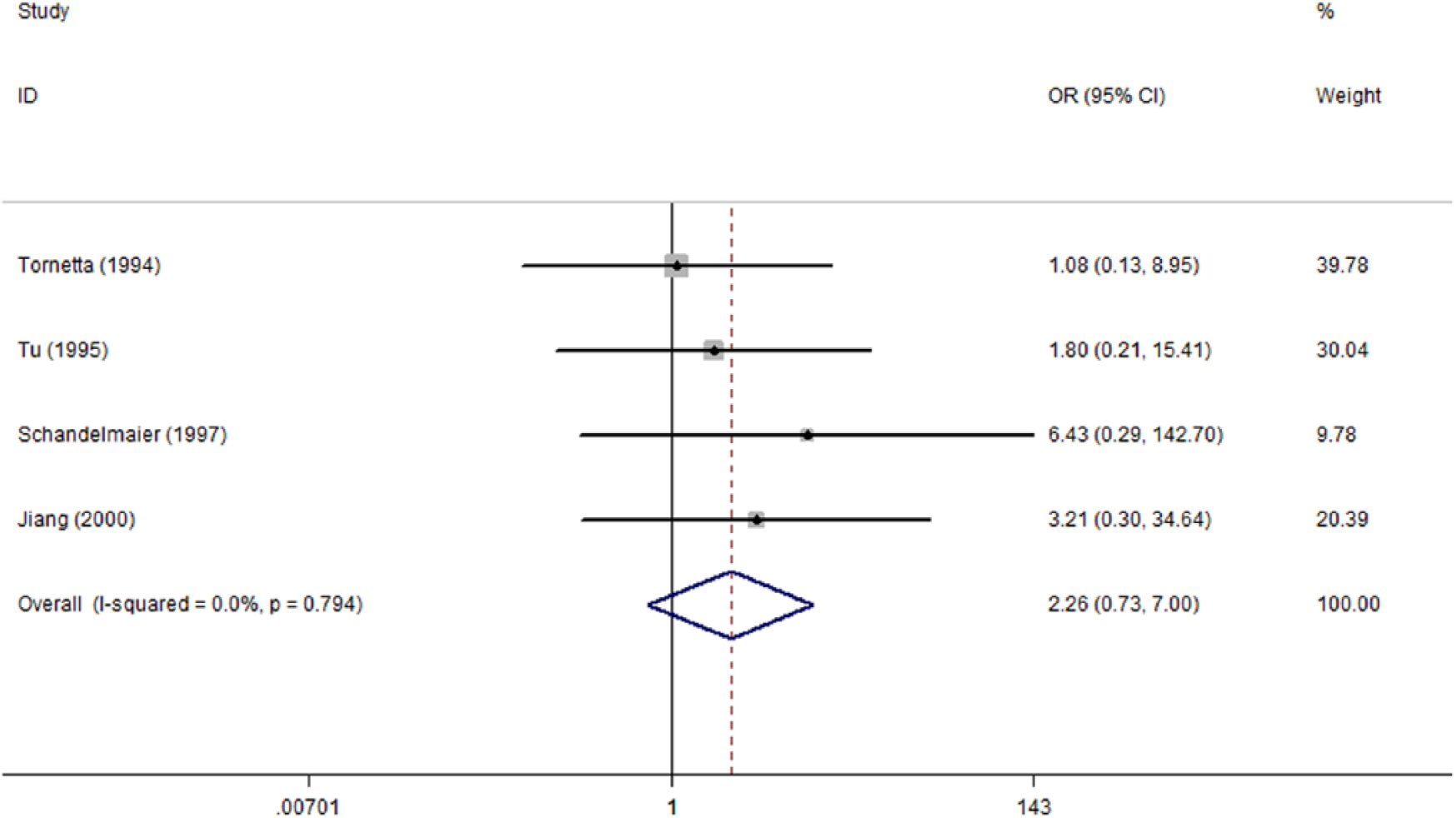
Forest plot of OR with 95% CI for the incidence of delayed union.
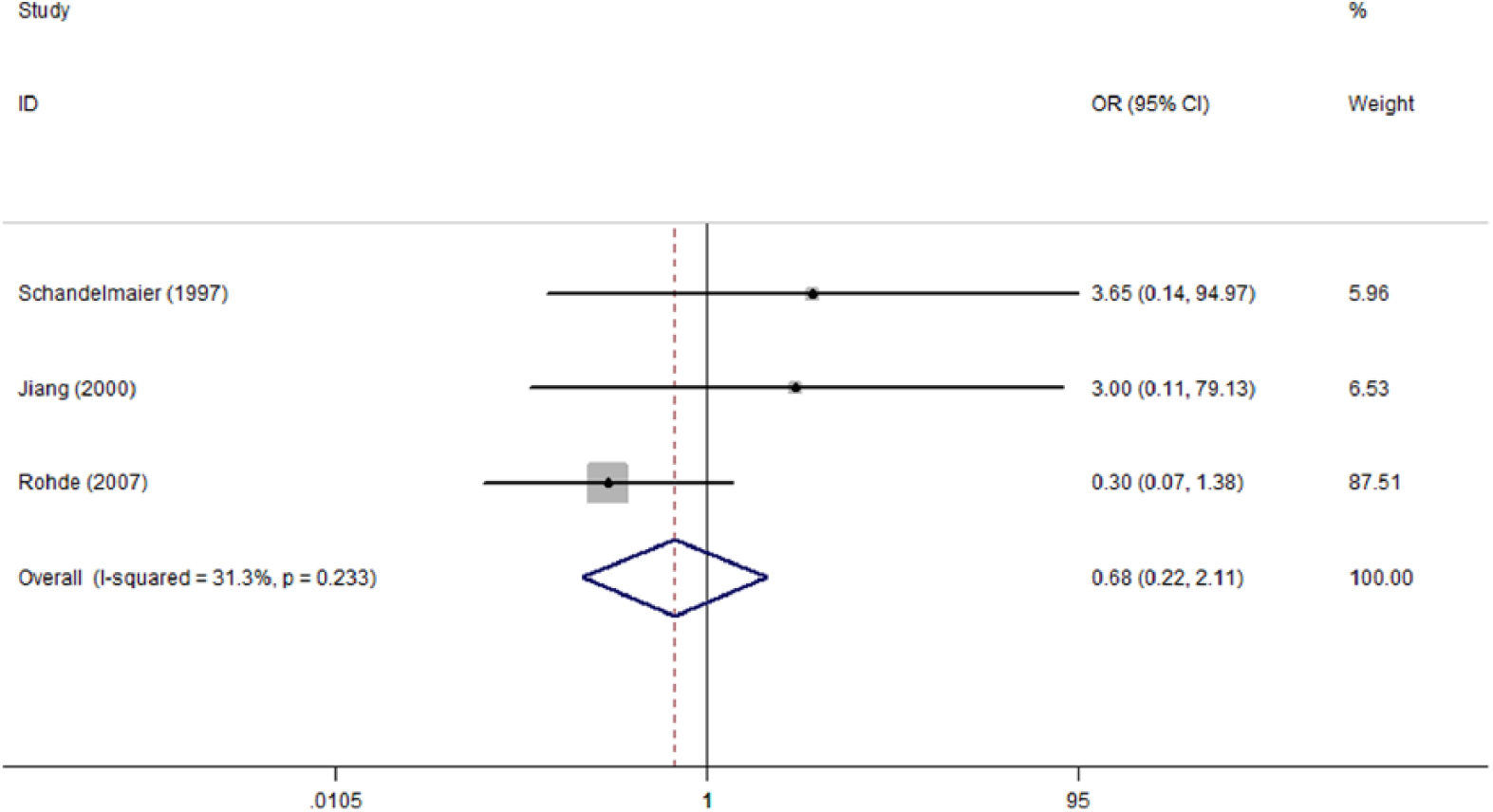
Forest plot of OR with 95% CI for the incidence of non-union.
Malunion is commonly defined as follows: (1) valgus or varus from frontal view or sagittal line deformity; (2) malrotations; and (3) limb length discrepancy, more than 1.5 cm. And in this study, UIN was associated with a lower overall malunion rate (26.7% versus 48.8%) than EF, and the discrepancy approached significance (OR: 0.27; 95% CI: 0.09–0.78) without any heterogeneity (I2 = 0) (Fig. 4).
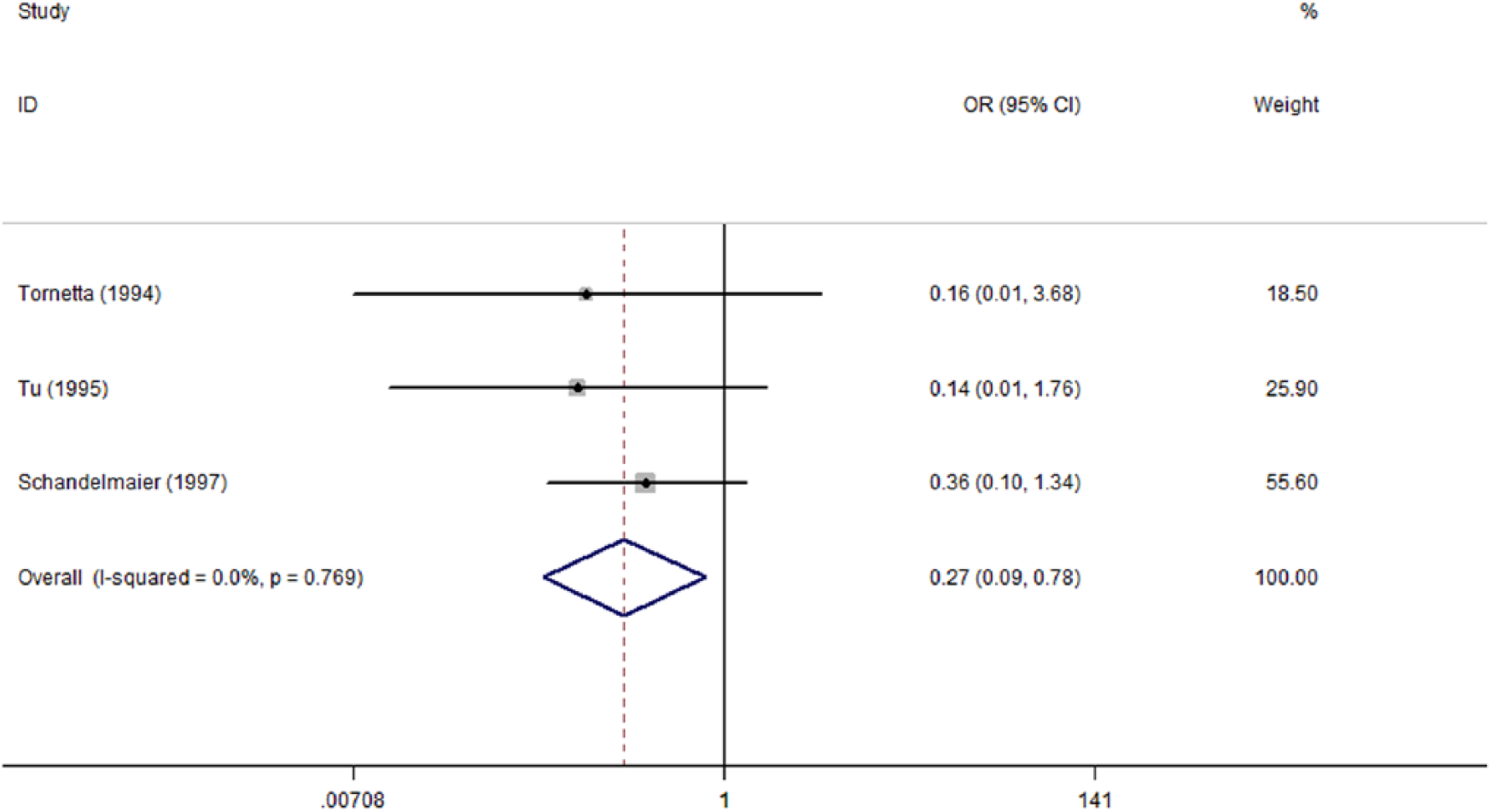
Forest plot of OR with 95% CI for the incidence of malunion.
Regarding the infections, superficial infection mainly includes pin site infection in EF and incision infestation in UIN. The result revealed a significantly lower superficial infection rate in UIN than EF (OR: 0.39; 95% CI: 0.17–0.87) in the context of partial heterogeneity (I2 = 47.6%) (Fig. 5). Deep infection including osteomyelitis is an important observation item in grade III open fracture for a surgeon’s consideration to prevent amputation or even more severe results. The meta-analysis for six studies involving 84 UINs and 79 EFs did not investigate a significant difference between both methods (OR: 1.07; 95% CI: 0.43–2.63) (Fig. 6).
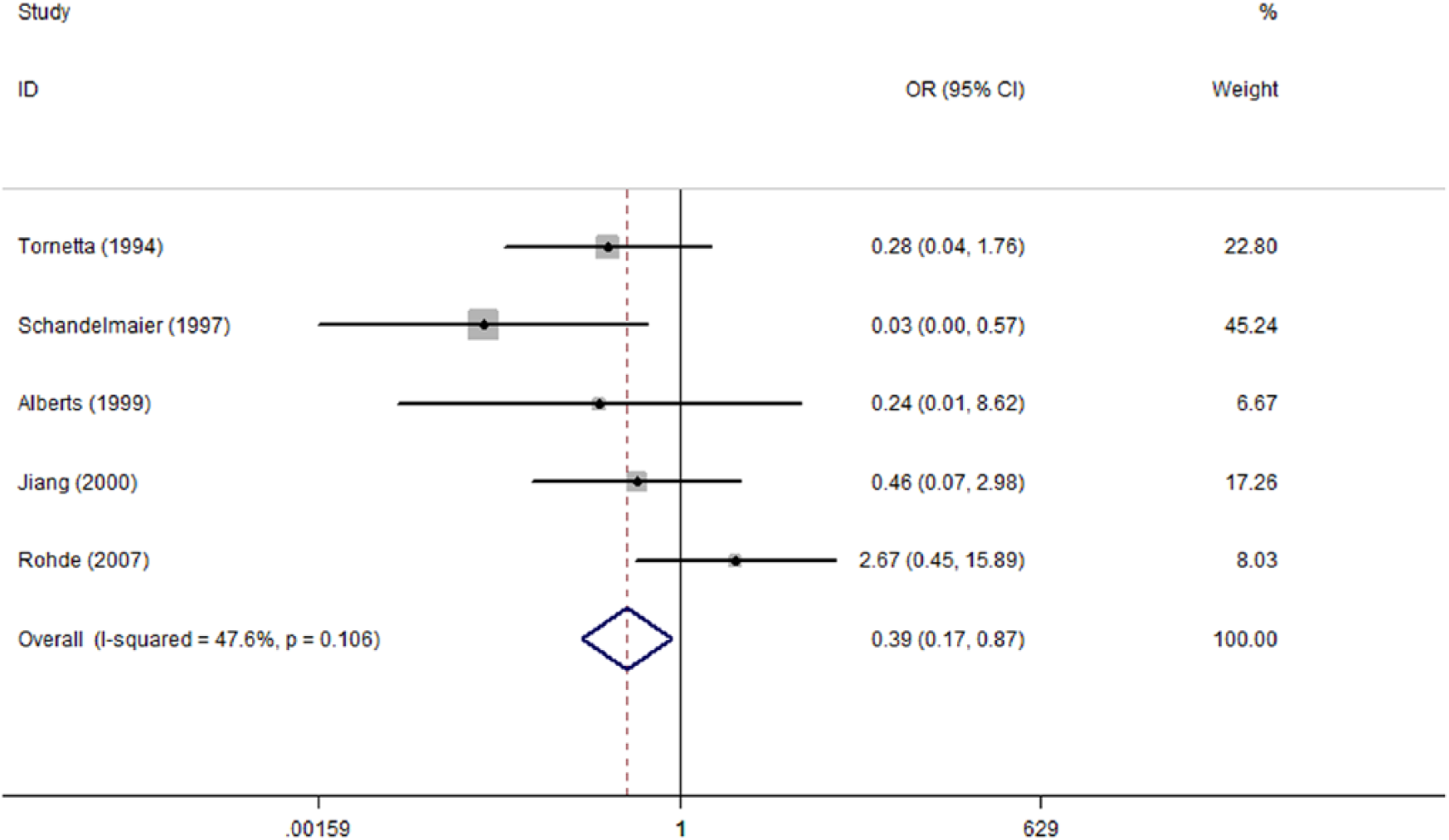
Forest plot of OR with 95% CI for the incidence of superficial infection.
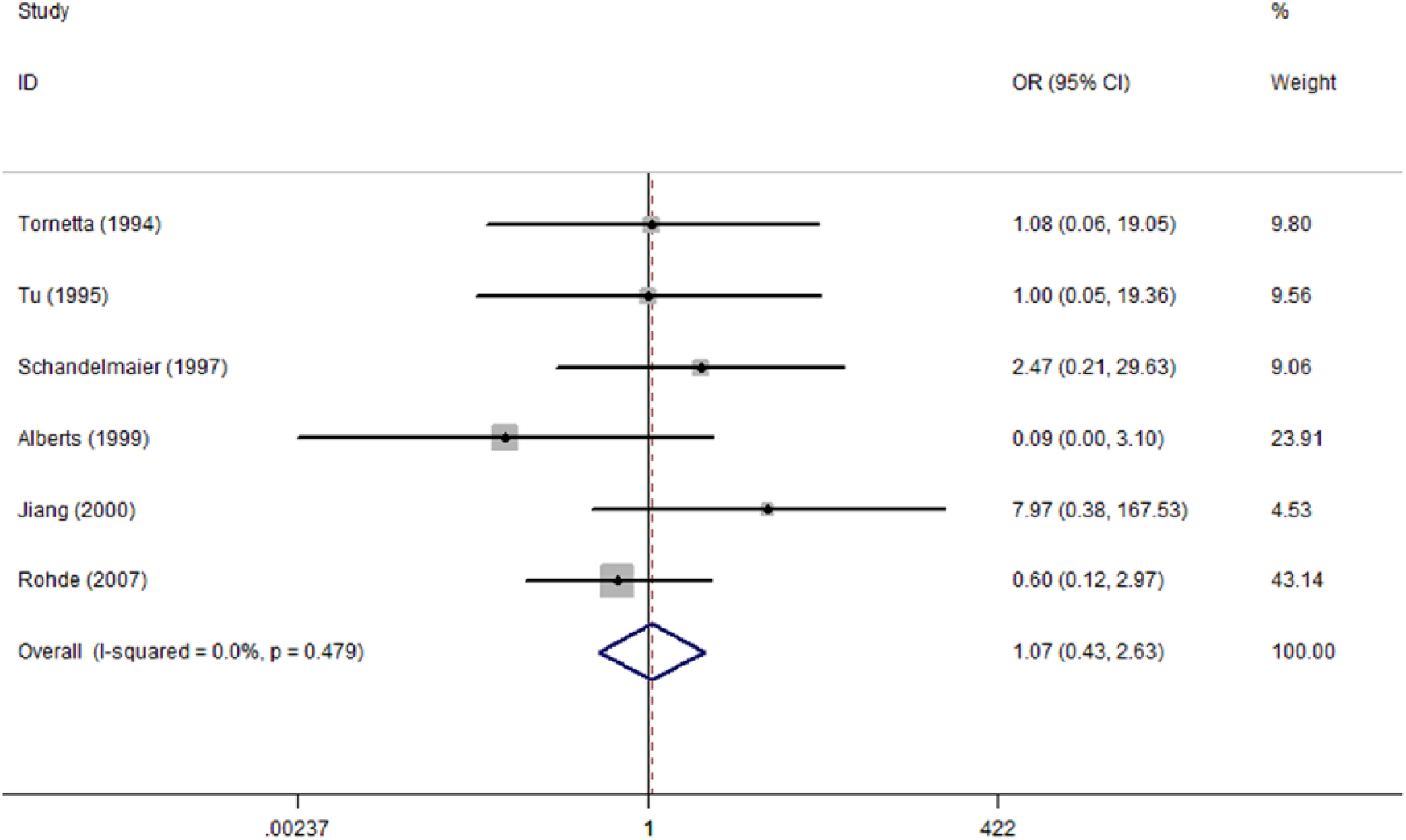
Forest plot of OR with 95% CI for the incidence of deep infection.
Four studies reported hardware failure (4, 9, 10, 15), and the overall incidence rates were 14.7% (10/68) and 14.3% (9/63) in UIN and EF, respectively. After meta-analysis, there was no significance (OR: 1.01; 95% CI: 0.40 to 2.58) with heterogeneity contributing partially (I2 = 23.6%) (Fig. 7).
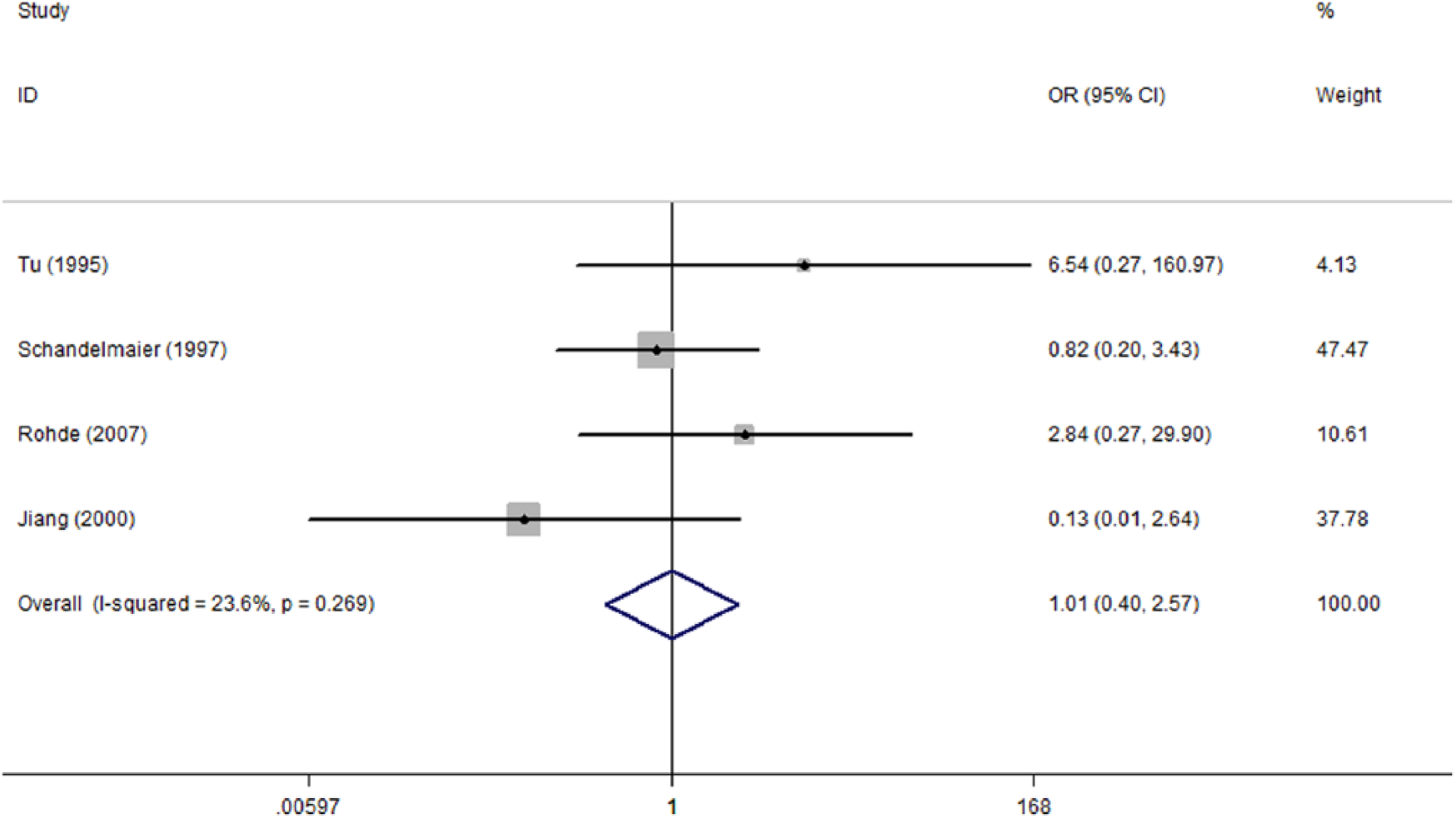
Forest plot of OR with 95% CI for the incidence of fixation failure.
Discussion
Severe open fracture has been a troublesome problem for clinical orthopedic and plastic surgeons due to combined and multiple injuries (16–18). Gustilo et al. (19) first proposed a new classification (IIIB) for type III open fractures based on the varied severity and prognosis, and grade B was defined as “extensive soft-tissue injury loss with periosteal stripping and bone exposure.” Management of type IIIB fractures is a challenge and undergoing controversy. Meta-analyses in this study revealed a superiority of UIN in treatment of Gustilo IIIB tibial fractures, being associated with reduced time to union and lower superficial infection and malunion rates. And in other adverse events, no significant differences were observed. The results should aid surgeons in making a more rational decision of therapeutic choice.
Patients’ infection status was commonly documented in the literature, and both superficial and deep infections could affect UIN and EF. Superficial infections commonly referred to internal fixations’ incision infestation and external fixators’ pin site infection or shared local erythema. Consistent with several studies, a high superficial infection incidence was more likely to exist in EF but with lower severity (7, 10, 12). And in clinics, the priority of infection prevention was commonly applied in EF patients; thereby, it could be effectively controlled by oral antibiotics (7, 11, 20). In contrast with the slighter superficial infection, almost all studies emphasize the deep infections including osteomyelitis due to its utmost importance in judging patients’ prognosis of limb salvage and function reserve (21), especially for patients treated by UIN, as required thorough exposure of the marrow cavity potentially increases the risk of further contamination and even amputation. And as for EF, most of the osteomyelitis patients generally have early infection and massive soft-tissue defects, and very few of them developed from the pin tract infection. Tielinen et al. (22) investigated the favorable functional outcomes of 19 consecutive patients with Gustilo IIIB open tibial shaft fractures with extensive soft-tissue injury while without any infection, with muscle flaps used in all patients. However in Rohde et al.’s (4) study, he investigated a higher osteomyelitis incidence in UIN groups, but participants in his study were all covered by microvascular free flaps. Compared to free flaps, muscle flaps possess more abundant blood supply, more powerful anti-infective ability, and are easier to survive. Therefore, in Gustilo IIIB tibial fractures with extensive soft tissues, the muscle flaps might be a better alternative. Of course, both procedures must be completed rigorously in the context of adequate debridement and operative care of tissue to minimize deep infection (7).
Consistent with some studies, UIN was identified to be associated with a reduced time to union (7, 10, 23). Several procedures including thorough debridement, exact alignment, better stabilization, and timely coverage of fracture and hardware might determine the union process (11, 23). However, in clinics, the length of time to union was not the first consideration item for surgeon, and if favorable coordination of bony fixation and a predictably reduced incidence of complications could be achieved, a slightly longer time to union should be acceptable (11). The lower incidence rate of malunion was another significant advantage investigated in UIN over EF in this study, which was in accordance with several studies (7, 24, 25). However, one study by Inan et al. (26) reported that, as for severely comminuted fractures, UIN did not provide an adequate stability and the malunion occurred likely secondary to technical errors, which was not reported in any other studies. Meanwhile, the technique of intramedullary nail insertion in general requires a relatively short learning curve; therefore, this problem is not difficult to solve (27). Regarding avoiding the malunion, Inan et al. (26) suggested Gustilo IIIA fracture site be stabilized by cast or brace for 6 weeks after external fixator removal, but whether this method was suitable for IIIB was unclear. If malunion occurred, corrective osteotomy and plating had to be performed to achieve an acceptable alignment of uttermost (7).
This meta-analysis has some limitations to be mentioned. First, not all the six included studies in the current meta-analysis satisfy the adequate randomization criteria; furthermore, some studies were retrospective rather than prospective; both of these might generate some biases and thereby lower test credibility. Second, all the provided ORs were computed based on frequency in the original studies, namely, crude ORs, but participants were statistically similar in demography and injury mechanism, indicating the pooled estimates reliable. Third, there were no allocation concealment measures taken in the studies, but lack of complete blinding might not greatly affect the treatment outcome. Fourth, the small sample size in the original and the fewer studies included in the meta-analysis might contribute to less powerful final and fixed conclusion. Therefore, more randomized controlled trials with larger sample size and better design are still in urgent need to obtain a persuasive result.
Despite the above limitations, this meta-analysis has several strengths. First, both computer and manual search were performed, which ensures a complete inclusion of relevant studies. Second, there was no significant heterogeneity in observational variables except for time to union, and even if so, heterogeneity was further investigated using sensitivity analysis. Above all, this meta-analysis to date first gives a definitive result of preference for either of the two methods in treatment of Gustilo IIIB tibial fractures, reflecting the current status on this issue.
In conclusion, as an updated meta-analysis concerning treatments for Gustilo IIIB tibial fractures by now, our study suggests UIN to be associated with a significantly lower superficial infection and malunion rates and a reduced healing time, while without increasing the risk of other adverse events (delayed union, non-union, deep infection, and fixation failure) compared to EF. Therefore, UIN should be preferred to treat Gustilo IIIB tibial fractures, and more multi-centre randomized controlled studies with large sample and better design are required in the future to verify this viewpoint.
Footnotes
Acknowledgements
Fei Zhang and Yanbin Zhu contributed equally to this article. The authors are grateful to J.C. and Z.W. of the Department of Orthopedics and to X.C. and G.W. of the Department of Statistics and Applications for their kind assistance.
Declaration of Conflicting Interests
All the authors declare that they have no conflict of interest with any organization that sponsored the research.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 81401789).