
Abstract
Background and aim:
Gastroesophageal junction cancer is one of the leading causes to cancer-related death and the prognosis is poor. However, progress has been made over the last couple of decades with the introduction of multimodality treatment and optimized surgery. Three-year survival rates have improved to 50% in patients receiving neoadjuvant therapy. Only a few studies have focused on the difference of postoperative complications in patients receiving neoadjuvant therapy in relation to a comparative surgery-only group. The aim of this study was to compare the prevalence of postoperative complications of patients with cancer at the gastroesophageal junction treated with either neoadjuvant chemotherapy or surgery alone in patients from “The Danish Clinical Registry of Carcinomas of the Esophagus, the Gastro-Esophageal Junction and the Stomach.”
Materials and methods:
A historical follow-up study, comparing postoperative complications between two cohorts before and after implementation of chemotherapy was completed.
Results:
In all, 180 consecutive patients treated with perioperative chemotherapy and a comparative surgery-only group of patients were identified from The Danish Clinical Registry of Carcinomas of the Esophagus, the Gastro-Esophageal Junction and the Stomach. No difference was found in demographics between the two groups, except for alcohol consumption and a lower T and N stage in the surgery-only group, and no difference in complication rates was found. Furthermore, no variable in the multivariate analysis was significantly associated with anastomotic leakage which was considered the most severe complication.
Conclusion:
Since perioperative chemotherapy does not appear to increase surgical complications, the future challenges include defining the optimal combination of chemo- and/or radiotherapy, but more importantly also to select the patients who will benefit the most from the different neoadjuvant strategies.
Keywords
Introduction
Gastroesophageal (GE) cancer is one of the leading causes of cancer-related death worldwide. In Denmark, like other western countries, mortality is high due to late diagnosis; only one-third of all newly diagnosed GE cancer patients in 2010 were considered to have operable or resectable disease (1). Thus, among patients with GE cancer undergoing intended curative resection, the 3-year survival is still as low as 28%–41% (2–4). Poor postoperative survival rates are related to recurrence in patients despite R0 resection; however, some progress has been made over the last couple of decades with the introduction of multimodality treatment and optimized surgery. Three-year survival rates have improved to 48%–56% in patients receiving neoadjuvant therapy (3–6). This has been shown in studies using pre- or postoperative chemotherapy alone, perioperative chemotherapy, and regimens using preoperative chemoradiotherapy as well as regimens using adjuvant chemoradiotherapy. Since the publication of the pivotal MAGIC-study (2), which has been supported by other randomized studies and meta-analysis (6, 7), perioperative chemotherapy has become implemented into Danish national guidelines as a standard of care for patients with resectable adenocarcinoma in the esophagus, gastroesophageal junction (GEJ), and stomach.
While survival rates have been improved, concerns have been raised about the potential for increased rates of postoperative complications after neoadjuvant therapy. An increase in postoperative complications could result in fewer patients commencing adjuvant chemotherapy, potentially off-setting the overall benefit. A difference in postoperative complications has been shown, from 16% to 27% between a surgery-only and a neoadjuvant chemotherapy group, but the trial was stopped prematurely due to poor accrual and the difference did not reaching statistical significance (p = 0.09) (8). Others, however, have not found a significant difference (9, 10). Most studies have focused on the toxicities and adverse effects of neoadjuvant therapy, but only a few studies have focused on the difference of postoperative complications in patients receiving neoadjuvant therapy compared to patients receiving only surgery (9–11).
The aim of this study was to compare the prevalence of postoperative complications of patients with GEJ cancer treated with either neoadjuvant chemotherapy or surgery alone in Denmark.
Methods and Materials
In Denmark, only four centers (Rigshospitalet, Copenhagen, Odense University Hospital, Aarhus University Hospital and Aalborg University Hospital) are performing GE cancer surgery. All four centers are high volume centers with 92, 37, 43 and 13 curative intended resection in 2012 at the respective centers (1). In 2003, it became mandatory to register information concerning diagnosis and surgical treatment for all upper GE cancer patients. All registrations are collected prospectively in the “The Danish Clinical Registry of Carcinomas of the Esophagus, the Gastro-Esophageal Junction and the Stomach” (DECV-registry).
Patients in the DECV-registry are identified and followed on the basis of the personal civil registration (CPR) number assigned to all Danish citizens at birth by The Danish Civil Registration System (CRS). CRS was established in 1968 and since then all persons in Denmark have been registered. Among other, the variables include information on gender, date of birth, place of birth, place of residence, and vital status and the information are continuously updated (12). All data collection is mandatory and is automatically uploaded and registered from the hospitals to the CRS.
Study Population
This study was designed as a retrospective follow-up study, comparing postoperative complications between a group of patients who had undergone a recently implemented perioperative chemotherapy regimen (Group 1) and a preceding surgery-only group of patients from the same centers (Group 2). Group 1 was defined as all consecutive patients from the four centers, operated on biopsy-proven adenocarcinoma at the GEJ, who had undergone preoperative chemotherapy prior to surgery as a part of the perioperative chemotherapy regimen. All patients were included according to time of their positive biopsy from the onset (2008/2009) of the perioperative chemotherapy regimen at each center to 31 December 2010. Group 2 was defined as an equal number of consecutive patients from each center, having date of surgery before the time of implementation of the chemotherapy protocol. All patients who had undergone a resection without neoadjuvant therapy was included. GEJ cancer was defined according to Siewerts classification, I–III (13). Patients with esophageal cancer, squamous cell cancer, or gastric cancer were excluded from the analysis.
Preoperative Chemotherapy
Following the presentation of the MAGIC trial (2) and the FNLCC ACCORD07-FFCD 9703 trial (6), the DECV-cancer group, who are responsible for the national guidelines, decided to implement perioperative chemotherapy in 2008 for patients with T2-4/N0 and T1-4/N+ stage GE adenocarcinoma in Denmark.
At the four centers, primarily two different chemotherapy regimens were instituted; ECX: cisplatin (60 mg/m2) and epirubicin (50 mg/m2) on Day 1 every 3 weeks and continuous peroral capecitabine (500 mg/m2) twice daily, and EOX, that is, the same regimen with cisplatin substituted by oxaliplatin (130 mg/m2). The FLOX regimen with oxaliplatin (130 mg/m2) and intravenously administered fluorouracil (400 mg/m2) on Day 1 was instituted in a minority of patients (4/191). Patients were scheduled for three series of chemotherapy preoperatively and three series postoperatively.
Surgical Procedure
Ivor Lewis esophagectomy performed for GEJ as a two-phase abdominal and right chest approach for en-bloc subtotal esophagectomy followed by an esophagogastric anastomosis and a D1 resection extended with dissection of the truncal celiac adjacent nodes are considered standard operative procedures in Denmark. However, during the study period, some procedures using laparoscopic- or thoracoscopic approach or a combination of the two procedures were performed. A few procedures were also performed with anastomosis at the neck.
Mortality
We obtained information on vital status and date of death from the CRS. Mortality was linked to the study population by CPR numbers. Patients were followed from date of surgery for 12 months or until death, if prior to before 12 months. This period was chosen as it was the maximum time span in which all patients could be followed before the censoring date.
Complications
All data concerning patient demographics, type of operation, complications, and mortality were obtained from the DECV-registry. Complications were graded using a modified Clavien–Dindo classification (14)—Grade 1: wound infection; Grade 2—pneumonia, acute myocardial infarction, pulmonary embolism, rupture of the fascia, and other leakages, not requiring surgical intervention; Grade 3/4: pleural empyema and/or anastomotic leakage; and Grade 5: death within 30 days.
Center 2 did not report any complications, besides anastomotic leakage and mortality. This was considered a reporting bias, and their data were omitted from the Grade 1 and 2 complication analysis, as shown in Table 1.
Postoperative complications in the two groups according to Clavien–Dindo classification.
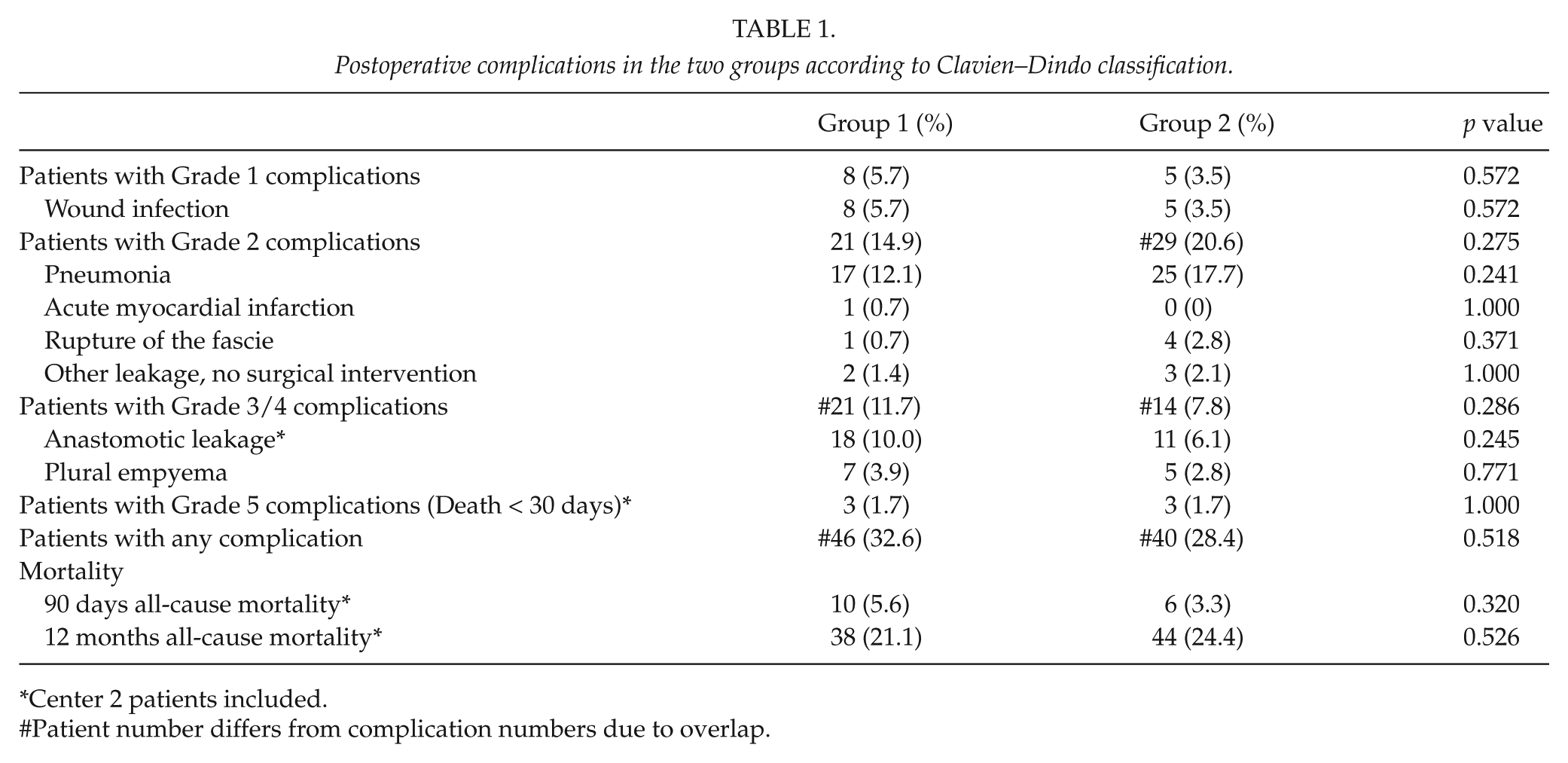
Center 2 patients included.
Patient number differs from complication numbers due to overlap.
Statistical Analysis
Data were analyzed using Mann–Whitney test (Kolmogorov–Smirnov test), or χ2 when appropriate. Independent variables associated with the development of anastomotic leakage were analyzed by using a logistic regression model. Variables with p-value < 0.1 in univariate analyses were incorporated into a multivariate logistic regression analysis using a forced entry model. p values < 0.05 were considered significant. Statistical analysis was performed using SPSS® version 20.0 (SPSS, Inc., Chicago, IL).
Results
Patient Characteristics
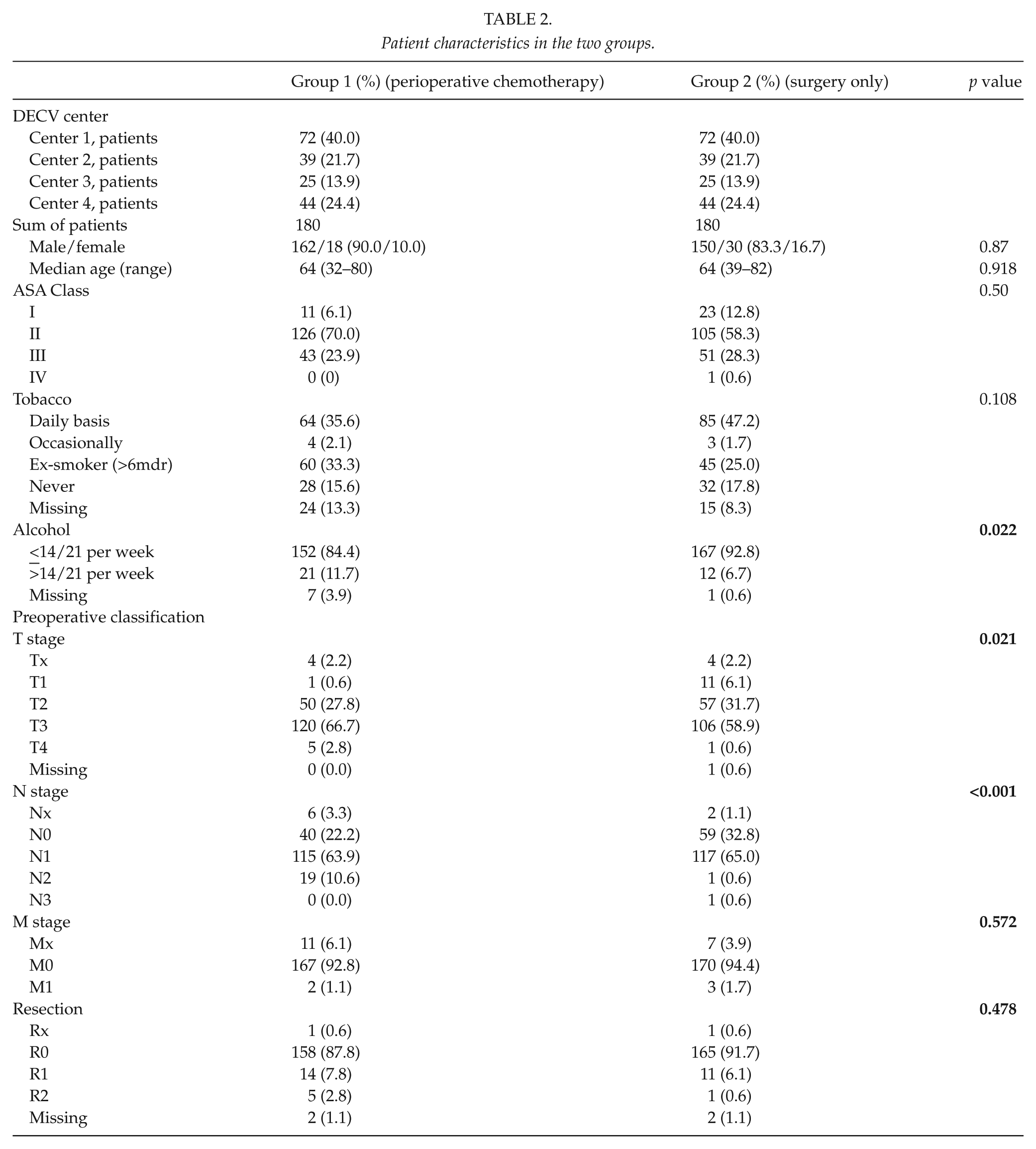
Baseline demographics of the patients are shown in Table 2. In Group 1, after the implementation of the perioperative chemotherapy regime, a total of 180 consecutive patients (90% male, 10% female) from four centers underwent preoperative chemotherapy and surgery for GEJ adenocarcinoma from May 2008 until December 2010. According to the inclusion criteria, Group 2 consisted of 180 consecutive patients (83.3% male, 16.7% female) from January 2004 until January 2009, the time of implementation of the perioperative chemotherapy regimen. There were no statistically significant differences in demographics between the two groups (Table 2), except for alcohol consumption and a lower T and N stage in Group 2, which could reflect patient selection to preoperative neoadjuvant therapy (T2-4/N0 and T1-4/N+ stage). Median follow-up was 12 months (range 0–12) in both groups.
Patient characteristics in the two groups.
Operative Parameters
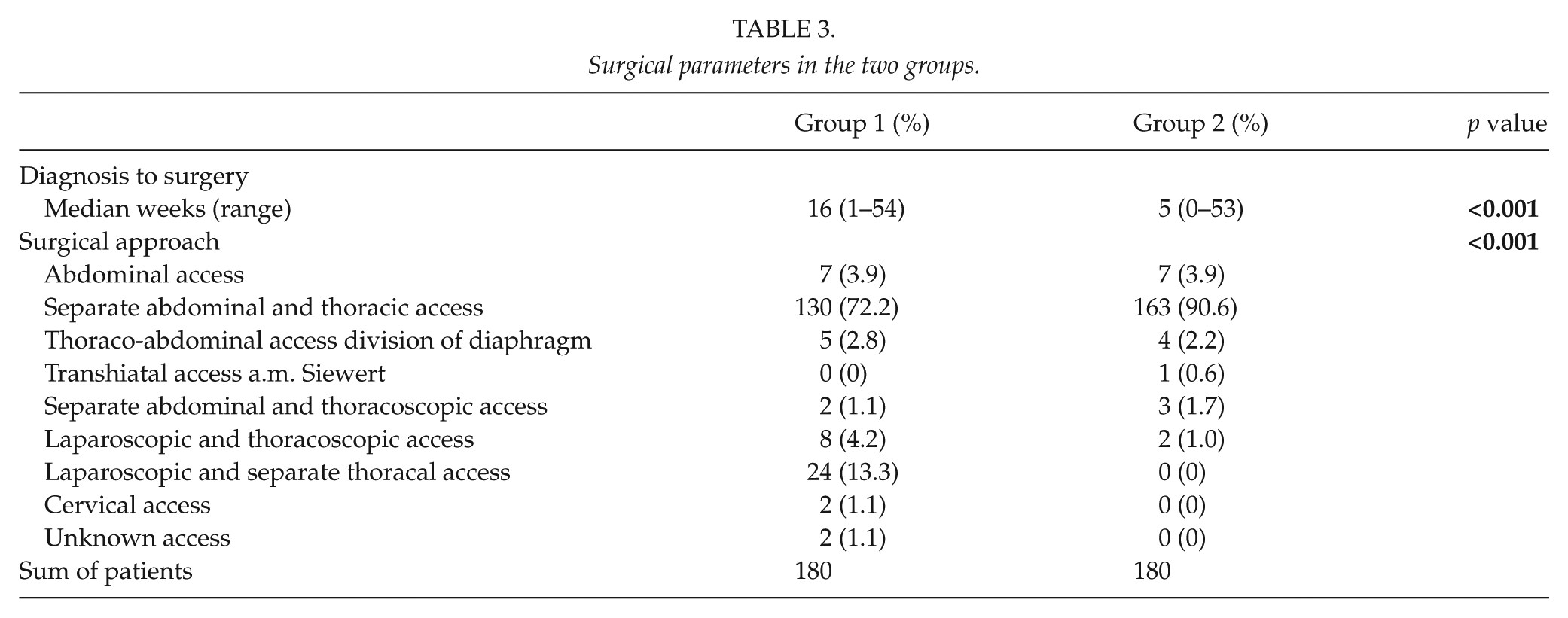
Time from positive biopsy to surgery is shorter in Group 2 as shown in Table 3, which also shows the operative parameters. The surgical approach is predominantly separate abdominal and thoracic access for GEJ resection. One exception, however, is the minimal invasive (laparoscopic and thoracoscopic) only approach, which was introduced in Center 3 in 2008 and is now the standard approach at the center.
Surgical parameters in the two groups.
Complications
Complications occurred in 89 of 360 patients (24.7%), but after the omission of Center 2, complications occurred in 86 of 282 patients (30.1%) in the remaining three centers. Complications were not statistically significantly different between the two groups in the different complication categories. Concerning the occurrence of anastomotic insufficiency, the data of Center 2 were included in the analysis of anastomotic leakage, Grade 3/4 and 5 complications, and no difference between the groups could be found. For anastomotic leakage, which is considered the most severe complication, besides death, three variables (groups, center, and alcohol) were associated with anastomotic leakage in the univariate analysis. However, the multivariate analysis revealed no independent association.
Early death/Grade 5 complications (<30 days) and 90 days mortality were 1.7% and 5.6%, respectively, in the preoperative chemotherapy group (Group 1) versus 1.7% and 3.3% in the surgery alone group (Group 2). This was not significantly different between the groups (p = 1.000 and p = 0.320). Survival (12 month) was 79.3% in Group 1 compared with 76% in Group 2. This was not significantly different between the groups (p = 0.526).
Discussion
This study found no difference in the prevalence of postoperative complications, of any grade between groups who received preoperative chemotherapy or surgery alone. Furthermore, no variable in the multivariate analysis was significantly associated with anastomotic leakage which is considered the most severe complication. In addition, our data did not show a significant difference in survival between the two groups at <30 days (Grade 5 complication), 90 days, or at 12 months.
The postoperative complications were 32.6% and 28.4% for Groups 1 and 2, respectively, and the 30 days mortality was and 1.7% for both groups in this study. This is in line with other retrospective studies that found a postoperative complication rate of 18%–29% and 1.4%–3.8% mortality for a perioperative chemotherapy and surgery-only regimes (15). The Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial (2) found higher postoperative complications in 45.7% and 45.3% of the groups of chemotherapy and surgery alone and a mortality of 5.6% and 5.9%, respectively. One possible explanation for this difference is the centralization of care in Denmark, which has reduced the number of centers performing GE cancer surgery from 26 to 4 (16). In comparison, the MAGIC trial had significantly higher heterogenicity with more than 45 centers from six countries participating. The higher volume per center, just as the implementation of the D1+ resection, is among plausible reasons for the lower complication rates.
Our results found no statistically significant survival benefit in the chemotherapy group. Whether our results reflects the fact that only GEJ cancers and no gastric cancers were included needs to be addressed in later studies. However, our study did demonstrate a trend from a higher 90-day mortality rate to a lower 12-month mortality rate in the preoperative chemotherapy group compared to the surgery-only group. Although this finding was not statistically significant, it may represent an overall survival benefit in the preoperative chemotherapy group, which was not demonstrated due to the short follow-up period. Hypothetically, this could have attributed to the effect of chemotherapy on micrometastasis, which would not be evident at 90 days postoperatively. Several studies have shown a significant overall survival increase in groups receiving perioperative chemotherapy (2, 4, 17), which could indicate that a potential survival benefit could be seen at a later time of follow-up for our Group 1.
By now it is widely accepted that surgery alone is no longer an adequate therapy for resectable adenocarcinoma at the GEJ. Options include perioperative chemotherapy, preoperative chemoradiotherapy, adjuvant chemotherapy, and postoperative chemoradiotherapy. While adjuvant chemotherapy has been proven effective in gastric cancer studies in Asian populations, it is not well established in the western population (18, 19). In Europe, perioperative chemotherapy is a documented strategy for patients with resectable adenocarcinoma in the esophagus, GEJ, and stomach (2, 6). However, after the recent publications of the CROSS study (5), increased interest in preoperative chemoradiotherapy has emerged. With the combined therapy, median overall survival was improved (49.4 months versus 24.0 months, hazard ratio (HR) = 0.66, 95% confidence interval (CI) = 0.495–0.871; p = 0.003) with significant improvement in R0-resection rate (92%–69%, p < 0.001) and high pCR (complete response) rate (adenocarcinoma 23%). In a recently updated meta-analysis (7), a hazard ratio (HR) for all-cause mortality for neoadjuvant chemoradiotherapy versus surgery alone was 0.78 (95% CI = 0.70–0.88, p < 0.0001). In the meta-analysis, two studies (n = 194) compared neoadjuvant chemoradiotherapy versus neoadjuvant chemotherapy; the HR for the overall indirect comparison of all-cause mortality for these two strategies was 0.88 (0.76–1.01; p = 0.07) in favor of chemoradiotherapy. Thus, whether perioperative chemotherapy or neoadjuvant chemoradiotherapy is the optimal treatment for GEJ adenocarcinoma remains debatable.
The strengths of the current study are attributed to the DECV cancer group, which have implemented national guidelines. This has resulted in a few highly specialized centers and a very uniformly operative approach combined with a mandatory reporting procedure to the DECV-registry leading to a 97% reporting completeness (1). In addition, the CRS, which supplies every person in Denmark with an individual, unique number by which they are identified and registered all through life, ensures the ability to accurately follow each patient treated for GEJ cancer.
The weaknesses of this study are due to the issues associated with historical follow-up and a lack of randomization, as the collection of data were strictly from the DECV registry. Data are occasionally missing, insufficiently reported, and/or could be incorrectly coded. This makes a direct comparison between the groups difficult, which is further accentuated by the fact that patient selection criteria for the two groups are different. This is also evident from the difference in the preoperative T and N stage. However, the T and N stage along with other variables like groups, centers (minimal invasive vs. open surgery), smoking, and alcohol was not associated with anastomosis leakage. A possible underestimation of the difference in complication rates could be due to improvement in the perioperative setting over time, favoring the preoperative chemotherapy arm, but this reflects the retrospective design of the study. Likewise, a possible difference in complication rates may have been missed due to underpowering of the study, just as there is an inbuilt selection bias in the group of patients found fit enough for the perioperative chemotherapy. Furthermore, the group of patients who deteriorate during neoadjuvant chemotherapy and never make it to surgery may have added to the complication rate in the perioperative chemotherapy group. Caution should also be taken, when looking into the survival dates as the data are retrospective and not designed specifically for this. However, we found it interesting as survival data in all the studies on neoadjuvant therapy focus on survival and complications to the new treatments.
Conclusion
No difference in complication rates and mortality was found between the combined modality-group and the surgery-only group, but underpowering of the study cannot be ruled out. Since perioperative chemotherapy does not appear to increase surgical complications, future research should focus on surgical complications due to the different surgical (lymphadenectomy, laparoscopic, robot assisted, etc.) techniques and different oncological modalities to define the optimal combination of chemo- and/or radiotherapy. However, most importantly, future investigations should aim to determine which patients will benefit the most from the different neoadjuvant strategies.
Footnotes
Declaration of Conflicting Interests
All named authors hereby declare that they have no conflicts of interest to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.