
Abstract
Background and Aims:
Metabolic surgery is evolving and safer, but more effective alternatives are constantly sought for. The single-anastomosis gastric bypass was first described in 2001, and although controversial, this operation is gaining fast in popularity worldwide. This review is aiming at a critical evaluation of the procedure in the light of the literature.
Methods:
The abstracts of 73 articles were reviewed, and after removal of case studies, duplicates, and irrelevant articles, 10 articles remained for closer review.
Results:
Several thousand of this operation have been performed for more than 15 years. It is claimed to be an easier, safer, faster, and more effective metabolic operation compared to the standard Roux-en-Y gastric bypass. The proponents of this operation also claim that this operation is easier to revise and reverse, leaving more options compared to the situation after standard bypass in case of failure. However, there is much controversy surrounding this method, mainly concerning the possible harmful and in the long-term even carcinogenic effects of biliopancreaticoduodenal reflux in the gastric pouch.
Conclusion:
The single-anastomosis gastric bypass may be an attractive alternative metabolic operation. However, further studies with robust, long-term follow-up are needed.
Keywords
Introduction
Morbid obesity is a chronic disease, and as it is with any chronic condition, there is no single and permanent treatment effective in all patients once and forever, although metabolic surgery has proven more effective than conservative methods. Metabolic surgery is constantly evolving and safer, but more effective techniques are continuously sought for.
The single- or one-anastomosis gastric bypass, perhaps better known under the somewhat misleading name, the “mini gastric bypass,” was introduced by Robert Rutledge (1) in 2001. This alternative in the field of metabolic surgery has gained increasing attention lately due to its simplicity and claimed safety and effectiveness (2–11). However, there is much controversy surrounding this method, mainly concerning the possible harmful and in the long-term even carcinogenic effects of bile reflux in the gastric pouch (12, 13). The mini gastric bypass (MGB) is not to be confused with its earlier version, the Mason loop gastric bypass that was abandoned mainly because of problems related to symptomatic biliary esophagitis. Symptomatic biliary reflux, gastritis, and esophagitis have been reported after MGB as well (3, 7, 13), but the longer, lesser curvature based gastric pouch is believed to reduce reflux to a greater extent compared to the Mason loop gastric bypass (11, 14, 15). The long pouch has some resemblance with the Magenstrasse–Mill operation (16), but is more effective due to the added bypass. Nevertheless, concerns have been raised about chronic alkaline reflux and the risk for gastric cancer in the long term (12, 13, 17, 18).
The advantages with this technique as claimed by those speaking in favor of it are many: fewer sites for leakage and internal hernia, easier and faster to learn and perform, easy to reverse and revise, and with results at least comparable with the result following standard Roux-en-Y gastric bypass (RYGB).
Methods
An English-language literature search was performed through Medline, Cochrane Library, Embase, Scopus, and Google Scholar for any study on (key words) “mini gastric bypass,” “single-anastomosis gastric bypass,” “omega loop gastric bypass,” “Mason loop gastric bypass,” “one-anastomosis gastric bypass,” or “loop gastric bypass.” Only full-length articles in English language were considered, and some articles were obtained from the references of these articles. Searches were carried out between January and 13 April 2014. The abstracts of 73 articles were reviewed, and after removal of case studies, duplicates, and irrelevant articles, 10 articles remained for closer review (Table 1). Only one prospective, randomized study was found.
Resolutions of comorbidities as reported by the authors.
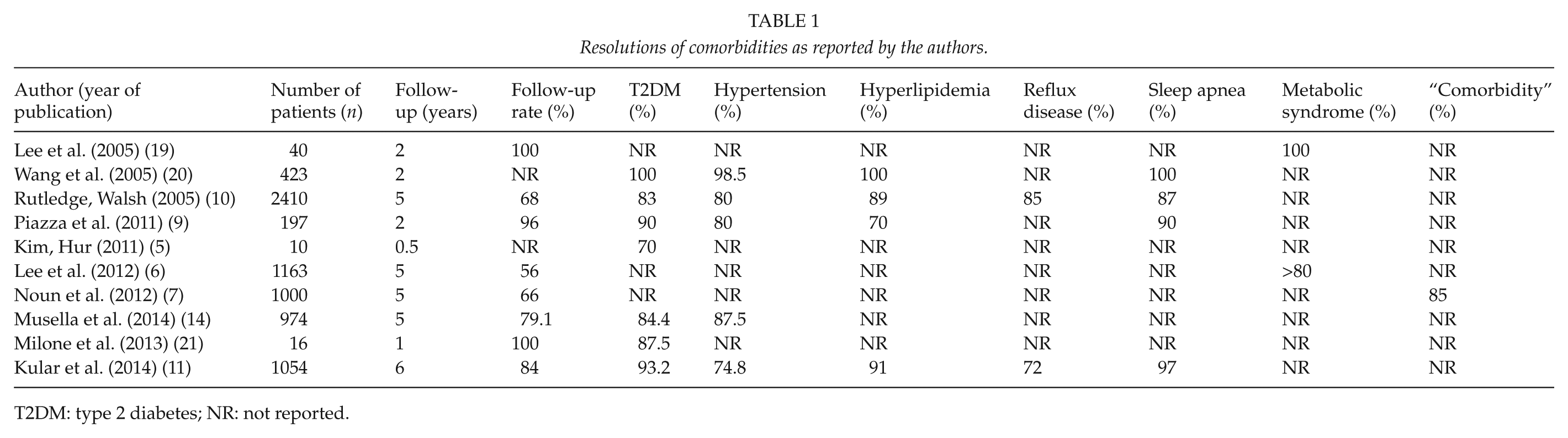
T2DM: type 2 diabetes; NR: not reported.
Results
Operative Technique
The original technique has been described by Rutledge (1) in detail. In short, five ports are used and the stomach is stapled along the lesser curvature with a calibration tube inserted and starting from the gastric incisura in order to create a long tube. The jejunum is lifted usually 200 cm from the ligamentum of Treitz and anastomosed to the gastric tube. The length of the biliopancreatic limb may be tailored according to baseline body mass index (BMI) (22). Garcia-Caballero and Carbajo (23) have described an alternative technique for the gastro-jejunal anastomosis in an attempt to reduce exposure of the gastric mucosa to biliopancreatic secretions because of their potentially carcinogenic effects with longer-term exposure, which is the major criticism of the original technique. In short, they claim that by “fixing the jejunal loop to the gastric pouch some centimeters up to the gastro-jejunal anastomosis the biliopancreatic secretions have less possibility of coming into the gastric cavity (gravity force)” (23). However, it is unclear on what evidence this opinion is based on.
Excess Weight Loss and Quality of Life
Robert Rutledge (1) reported excess weight losses (EWLs) of 68% at 1 year and averaging 77% at 2 years. In his later report, with a complete follow-up of 68%, the mean EWL at 1 year was 80% and weight loss was maintained within 10 kg of the maximum in >95% of patients up to 5-year follow-up (10). He reported an average operative time of 37.5 min and a median length of stay (LOS) of 1 day. In a very recent article by Kular and Rutledge from the Indian subcontinent, including 1054 patients with an 84% follow-up rate at 6 years (Table 1), the reported mean EWLs were 84%, 91%, 88%, 86%, 87%, and 85% at years 1–6, respectively (11). They stated that patient satisfaction was high, but no formal quality of life measure was used.
Others have reported mean EWL at 1 year between 55% and 88% (2, 10, 19, 20). Musella et al. (14) reported the Italian experience with outcomes from 974 consecutive cases in a multicenter review. The EWL at 5 years averaged 77%. Lee et al. (6) reported an improved EWL at 5 years of 73% compared to 60% following RYGB. However, the follow-up rate in their series of 1163 MGB patients was only 56% (6). In the study by Noun et al. (7), 95% and 90% of the patients achieved at least 50% EWL at 18 and 60 months, respectively, and the mean EWL was 69.9% at 1 year and 68.6% at 5 years. In the only randomized controlled trial (RCT) comparing laparoscopic Roux-en-Y gastric bypass (LRYGB) with laparoscopic mini gastric bypass (LMGB), the percentages of EWL at 1 and 2 years was 58.7% and 60% in the LRYGB group, and 64.9% and 64.4% in the LMGB group (19). These differences were not significant, but significantly more patients achieved EWL > 50% in the LMGB group (95%) compared to the LRYGB group (75%). Primary results from a French university hospital specialized in obesity surgery showed EWL percentages of 35%, 51%, and 63% after 3, 6, and 12 months, respectively (3).
Four studies have included formal quality of life measures in their outcome analyses following MGB. Lee at al. (6) used the gastrointestinal quality of life index to measure quality of life after LRYGB and LMGB and noted a significant increase after operation in both groups with no significant differences at 5 years. In the RCT of LMGB and LRYGB published by the same group, the gastrointestinal quality of life index score was significantly higher in both groups compared to preoperative values but without significant differences between the groups at 1 year (19). Carbajo et al. (2) found significant improvement in the impact of weight on quality of life (IWQoL) 3 months postoperatively compared to preoperative values. Wang et al. (20) concluded that the gastrointestinal quality of life index improved significantly 1 year after the operation.
Resolutions of Comorbidities
A summary of reported resolutions of comorbidities is seen in Table 1. Remission of type 2 diabetes (T2DM) varies between 70% and 100%; hypertension between 80% and 98.5%; hyperlipidemia remission, although not reported in most of the studies, varies between 70% and 100%; and sleep apnea remission is reported in 87%–100% at 1–6 years of follow-up (5–7, 9–11, 14, 19–21). According to Rutledge (10), 85% of the patients had improvement in their reflux disease, but he does not explain how this was measured. Lee et al. (6) stated that >80% of their patients had resolution of metabolic syndrome at 5-year follow-up, but they did not report any more details. In the RCT by the same group, the reported remission of metabolic syndrome at 2 years was 100%, again without giving any further details (19). The study by Milone et al. (21) was a small and nonrandomized comparison of sleeve gastrectomy versus MGB in the treatment of type 2 diabetes where MGB showed a clear trend toward higher diabetes remission rates (87.5% vs 66.7% for sleeve at 1-year follow-up). Noun et al. (7) reported only that 85% of their patients had remission of comorbidities and neither did they provide any further details. Kim et al. (5) studied 10 nonobese patients (mean BMI 27.2 kg/m2) and demonstrated the resolution of hyperglycemia in 70% of these T2DM patients.
Morbidity, Mortality, Conversion Rates, Los, and Follow-Up
Table 2 shows the experiences from five centers with around 1000 or more patients each included with 56%–84% follow-up rates at 5 years or more (6, 7, 10, 11, 14). Mortality is reported in 0.0%–0.18%, 30-day morbidity varies from 2.7% to 6.7%, leakage either from the gastric tube or from the anastomosis is reported in 0.2%–1.3%, conversion rates vary between 0.0% and 1.2%, mean operative time between 37.5 and 115.3 min, and mean LOS between 1.0 and 4.0 days. The mean time of follow-up was reported only by Rutledge (38.7 months). The follow-up rate at 5–6 years is incomplete in most studies and varies between 56% and 84%.
Mortality, morbidity, operative time, length of stay (LOS), follow-up (FU) as reported by the authors.
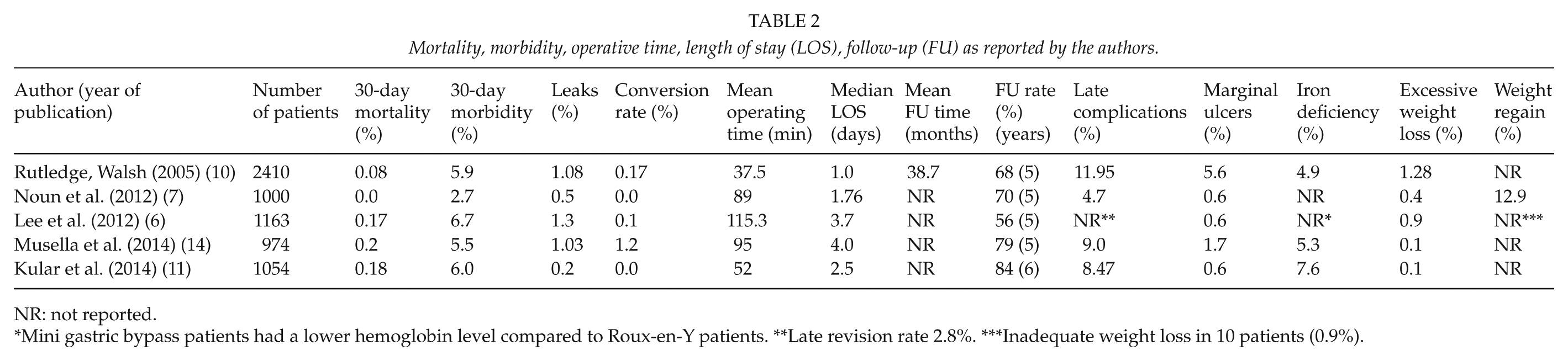
NR: not reported.
Mini gastric bypass patients had a lower hemoglobin level compared to Roux-en-Y patients. **Late revision rate 2.8%. ***Inadequate weight loss in 10 patients (0.9%).
Late Complications
The incidence of marginal ulcers was reported in 0.6%–5.6%. Iron deficiency anemia was not reported in two studies (6, 7), although Lee at al. (6) stated that the hemoglobin levels were lower following LMGB compared to LRYGB. In the remaining three studies, iron deficiency anemia occurred in 4.9%–7.6% of the operated patients (10, 11, 14). Excessive weight loss occurred in 0.1%–1.28% of the patients (Table 2). Excessive weight loss is not defined in most studies but is assumed to mean EWL > 100%. It is also unclear whether all authors reporting excessive weight loss equals this with malnutrition? At least Rutledge (10) reported excessive weight loss “with malnutrition” in 1.1% of his patients and a revision rate of 1% (31 patients) for this reason. Overall, revision surgery in his report was 1.3%, and in the report by Wang et al. (20), it was 1.7%. The revision rates are missing in most studies and probably underreported (13). However, there is a need for some revision surgery after standard RYGB as well. In the study by Lee at al. (6) comparing RYGB with MGB, the overall revision rates did not differ significantly (3.6% and 2.8%, respectively), but the need for revision surgery caused by malnutrition was five times higher after MGB (0.2% vs 0.9%, respectively). In the multicenter study by Johnson et al. (13), the main reason for revision surgery was pancreaticoduodenal reflux followed by malnutrition and marginal ulcer (13). The extent of malnutrition that does not need revision or the number of patients not being able to have revision surgery (for various reasons) is unknown.
Discussion
A total of 10 studies were included in this review, reporting some data on 7287 patients. Only 1 study was randomized and controlled, and only 4 studies included quality of life analyses. The follow-ups are short and most often incomplete. Late adverse symptoms are often poorly defined, and what is reported varies greatly between the studies making comparisons difficult. More randomized, prospective studies with longer follow-up including adequate analyses of quality of life are clearly needed.
The greatest criticism against the MGB has been raised by Johnson et al. (13). They reported data derived from five medical centers on 32 patients having revisions following MGB that all had been performed in other hospitals. Insufficient follow-up in centers performing MGB operations, and therefore a clear underreporting of late complications, was strongly suspected (13). This suspicion seems justified taking the insurance based health-care system in the United States into consideration. The extent of needed revision surgery in patients not having coverage by third party payers is unknown. On the other hand, this problem is probably equally present following any kind of bariatric surgery.
Those who are speaking in favor of the LMGB believe this is a safer, faster, and more effective procedure with a shorter learning curve compared to the standard LRYGB (3, 6, 11). It also seems to be associated with a lower complication rate both in short and long term (6, 7, 10, 11, 14). Obviating the need for a jejuno-jejunostomy and division of the omega loop reduces the number of sites for leakage and internal herniation. Until today, there is no report in the literature of internal hernia or bowel kink after LMGB. In case of inadequate or excessive weight loss, revision procedures (lengthening or shortening the biliopancreatic limb) are claimed easy to perform (2–10), and should there be a need for reversal of the procedure, the gastrojejunostomy can be taken down and the gastric tube reconnected to the stomach which in effect will lead to a Magenstrasse–Mill operation that is believed by some not to be completely without bariatric effects (16, 24). In other words, there seem to be more and easier options available compared to the standard LRYGB in case of failure.
The MGB is believed to be more malabsorptive than the standard RYGB due to its longer biliopancreatic limb. The only RCT comparing LRYGB with LMGB reported a 100% follow-up at 2 years and better results with LMGB (19). Shorter operative time, lower complication rates (7.5% compared to 20%), shorter LOS, and less postoperative pain were associated with the LMGB compared to LRYGB. Furthermore, significantly more patients undergoing LMGB achieved EWL of >50% (95% compared to 75% after LRYGB). There was no difference in the gastrointestinal quality of life index between the groups after 1 year, although the more malabsorptive nature of the LMGB could be expected to lead to more long-term morbidity, such as diarrhea and deficiencies (19). The incidence of marginal ulcers was slightly higher after LMGB (5%) than after LRYGB (3%). However, this study has been criticized for not meeting all the Consolidated Standards of Reporting Trials (CONSORT) requirements of an ideal RCT (15). Furthermore, the authors do not state their endpoints, nor do they explain how sample sizes were calculated. The authors have also been criticized for lack of experience with the LRYGB. Nevertheless, it is a significant study with a robust follow-up.
In this review, the incidence of iron deficiency anemia following MGB was reported from 4.9% to 7.6% (Table 2). Marginal ulcers and iron deficiency anemia were also the most frequent long-term complications reported by Rutledge (10) in his series of 2410 patients. The risk of these complications following MGB seems comparable or slightly higher than after RYGB (10, 11, 14, 20).
In a recent review by Mahawar et al. (15), the controversial aspects of the MGB were discussed in detail. Most of the criticism to this operation is derived from fear of biliary reflux and its potentially detrimental effects. Objective studies actually measuring the amount of bile reflux following MGB with esophageal impedance monitoring are missing. Anyway, there are persisting concerns regarding the potential risk of gastric and esophageal cancers due to biliary and pancreaticoduodenal reflux following MGB (12, 13, 17, 18, 25). These concerns are supported by an animal study showing that not pure biliary reflux but more specifically pancreaticoduodenal reflux caused gastric stump carcinoma in 10 out of 14 rats (25). Although till date no cases of gastric or esophageal cancers have been reported in humans after MGB, we have to remember the relatively small number of patients and short follow-up so far when evaluating the significance of this fact. Billroth II partial gastrectomy is associated with biliary reflux into the remnant stomach and at least was believed to be the explanation for the higher incidence of gastric stump carcinoma reported in these patients (26–32). These observations, however, were made before the bacterium Helicobacter pylori (H. Pylori) was discovered in 1984 (33). This bacterium is nowadays known to be a common etiological factor for both ulcers and cancers. Not only the Billroth II gastrectomy but all kinds of ulcer surgeries are associated with the increased risk of gastric cancer (26, 34, 35). This may imply that H. pylori rather than bile reflux plays the major role in the carcinogenesis. Or there may be a synergistic role of both bile reflux and H. pylori (36)? In the previously mentioned experimental animal study, the authors claim that it is unlikely that pancreaticoduodenal secretions alone are carcinogenic; rather they “perpetuate the hyperplastic response to a chronic irritant” (25). Could that “chronic irritant” be the presence of H. pylori? Whether bile reflux (or pancreaticoduodenal reflux) alone, without simultaneous H. pylori infection will result in a higher risk of cancers in the stomach or esophagus is a controversial matter and beyond the scope of this review.
In summary, the MGB may be an attractive alternative metabolic operation gaining in popularity worldwide. Several relatively large series and one RCT all report fairly similar results; shorter operative time, fewer short- and long-term complications, shorter LOS, better EWL and better sustained EWL at least during mid-term follow-up, and more effective in terms of resolutions of comorbidities compared to standard RYGB. However, the risk of symptomatic biliopancreaticoduodenal reflux, iron deficiency anemia, and marginal ulcers has to be kept in mind as well as the controversial issue of the possibly increased long-term risk of cancers in the gastric sleeve or esophagus. Further studies with robust, long-term follow-up are needed.
Footnotes
Declaration of Conflicting Interests
The author, Mikael Victorzon, declares no conflicts of interest or financial ties to disclose.