
Abstract
Background and Aims:
Fast-track protocols have been used to optimize the perioperative care and to enhance postoperative recovery. This study examined short-term clinical outcomes and determinants affecting the length of postoperative hospital stay.
Material and Methods:
From 2007 to 2009, 180 patients underwent laparoscopic or open bowel resection (N = 138) or sacrocolporectopexy (N = 42) in the Central Hospital of Central Finland for various colorectal diseases in the fast-track setting. The main measures of outcome were time to functional recovery, 30-day morbidity, and readmission rates, with hospital stay and patient satisfaction as secondary outcomes.
Results:
There were no deaths. Time to functional recovery was median 2 (interquartile range 2–3) days. The overall 30-day postoperative morbidity was 14.5% after bowel resection and 0% after sacrocolporectopexy. Relaparotomy rate was 3.6% and 30-day readmission rate 7.2%. Postoperative hospital stay was median 3 days after small bowel and ileo-colic resection, 4 days after segmental colectomy, and 6 days after rectal resection and subtotal colectomy. Patient’s body mass index > 30 kg/m2, malignant disease, complexity of surgery, recovery of bowel function later than 2 days after surgery, time to functional recovery > 2 days and postoperative morbidity were patient- and treatment-related determinants increasing postoperative hospital stay. Protocol compliance–related determinants increasing postoperative hospital stay were intake of normal food and mobilization ≥ 6 h/day later than 2 days after surgery and removal of urinary catheter later than 1 day after surgery.
Conclusion:
Postoperative functional recovery was fast, morbidity and readmission rates were low, and postoperative hospital stay short indicating that fast-track care should form the mainstay of elective colorectal surgery.
Introduction
Fast-track or enhanced recovery after surgery protocols have been used to reduce the surgical stress response and organ dysfunction, thereby enhancing recovery and reducing postoperative morbidity (1). The concept is based on multimodal evidence-based care platform and includes preoperative education and optimization of patients, attenuation of surgical stress response, optimized pain control, and postoperative rehabilitation with enforced oral nutrition and early ambulation (1–4). Randomized trials have now demonstrated the safety and efficacy of fast-track care in colorectal surgery, not only in reducing postoperative hospital stay and morbidity but also in improving patient convalescence and satisfaction when compared with traditional care (4–13).
However, despite strong clinical evidence effective implementation of all fast-track elements has proven difficult because it mandates a multidisciplinary collaboration between surgeons, anesthesiologists, and surgical nurses; a high rate of protocol compliance; and a good organizational structure (1). A significant variability in the components of different fast-track protocols has also been reported (14). Particularly, it is questioned whether all fast-track elements are of equal importance and which are the key factors that determine short-term clinical outcome in the fast-track setting (15, 16). The aim of this study was to investigate the impact of multimodal rehabilitation program on early functional recovery and short-term clinical outcomes and examine determinants affecting the length of postoperative hospital stay.
Material and Methods
A written fast-track protocol for colorectal surgery and manual for patient instruction was made in 2006 after several multidisciplinary meetings to discuss the critical, evidence-based fast-track elements. Staff nurses received an extensive education. Implementation of the protocol started in January 2007. Included were patients with a good mental and physical performance status and the American Society of Anesthesiologists (ASA) score I-III and having an attending person at home. Elderly patients fulfilling the predefined criteria were also included. Excluded were patients who underwent emergency surgery or a major multiorgan resection or palliative surgery for cancer. The protocol included 20 evidence-based elements in accordance with a recent international consensus review (3). Data regarding the surgical outcome and applied fast-track elements were collected daily by staff nurses using standardized forms and assessed on a weekly basis by the working group to monitor the outcome. A telephone call was made 2 days after discharge by a trained staff nurse to check the patient’s recovery and satisfaction. All patients were followed up for 30 days to assess morbidity and readmissions. The study was approved by the ethics committee of the hospital (K-Sshp no. 25-2007).
Surgical Technique
The operations were performed by senior staff surgeons with participation of the residents. The decision to do laparoscopic or open surgery was left to the surgeon’s discretion. Laparoscopic bowel resection was performed using the 5-trocar technique for right and left hemicolectomies and rectal cancer surgery. Specimens were extracted through a Pfannenstiel incision (left hemicolectomy, rectal cancer surgery) or a peri-umbilical horizontal incision (small bowel and ileo-colic resection, right hemicolectomy). Open surgery was performed using transverse incision for right hemicolectomies and midline incision for left hemicolectomies.
Definitions
Patients were considered functionally recovered when they were pain free (visual analog scale (VAS) ≤ 4) on oral analgesics, fully mobilized, and able to eat normal food. Conversion to open surgery was defined as a necessity to interrupt the laparosopic procedure and to proceed using conventional technique. Paralytic ileus was defined as the absence of bowel function for ≥5 days or the need for reinsertion of a nasogastric tube after starting oral diet in the absence of mechanical bowel obstruction. Postoperative hospital stay during the primary admission was defined as days spent in the hospital after surgery. Total hospital stay was defined as preoperative, postoperative, and readmission-related days spent in the hospital. Discharge was considered delayed when postoperative hospital stay was over 3 days after sacrocolporectopexy, small bowel, ileo-colic, and colonic resections in line with a previous study (17) and over 6 days after rectal surgery.
Statistical Analysis
Results are given as mean (standard deviation (SD)) or median (interquartile range (IQR)). The comparison between groups was made using t-test, Mann–Whitney test, or chi-square test. Analysis of patient-related, treatment-related, and protocol compliance–related determinants affecting postoperative hospital stay was done using univariate and multivariate zero-truncated Poisson regression models with robust standard errors or negative binomial regression (zero-truncated) models, when overdispersion was present. Only those fast-track elements with an adherence rate less than 100% were entered in the uni- and multivariable models. The length of hospital stay ratio (LOS ratio) was expressed as the ratio of mean hospital days. Variables with P ≤ 0.20 at univariate analysis were entered in the multivariate analysis. All statistical tests were two-sided. A P-value less than 0.05 was considered significant. STATA (StatCorp 2009. Stata release 12, Statistical Software. College Station, TX: StataCorp LP) was used for statistical analysis.
Results
Baseline clinical and treatment characteristics of the 180 patients are shown in Table 1. A total of 32 patients (17.8%) were older than 70 years and 27% of the patients had comorbid conditions (ASA grade > 2). The degree of adherence to the 20 predefined fast-track elements is shown in Table 2. Conversion to open surgery was necessary in 7 of the 131 laparoscopic procedures (5.3%) due to severe adhesions in 6 and difficult tumor localization in 1 patient.
Baseline characteristics of the 180 patients.
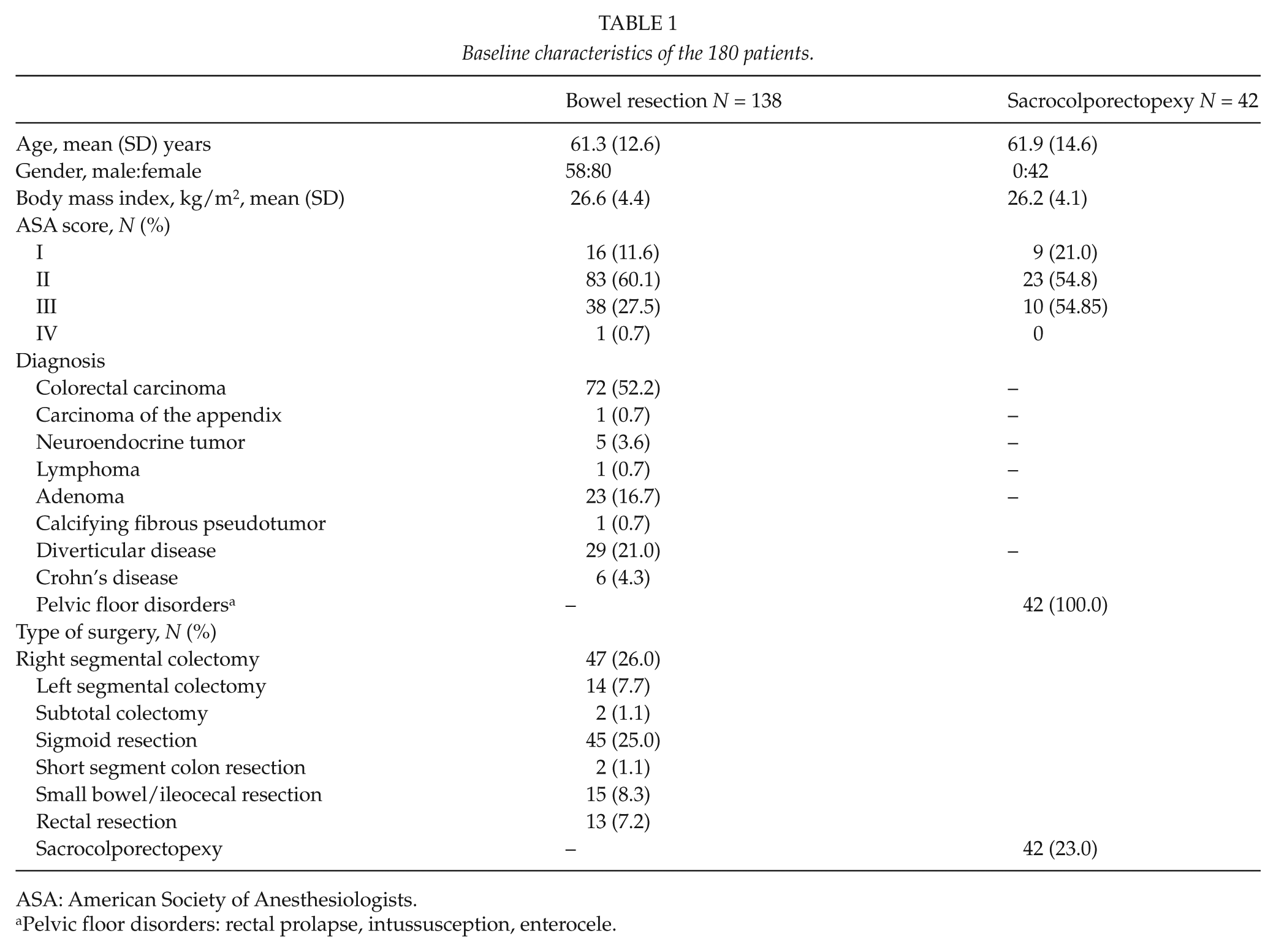
ASA: American Society of Anesthesiologists.
Pelvic floor disorders: rectal prolapse, intussusception, enterocele.
Compliance with fast-track protocol.
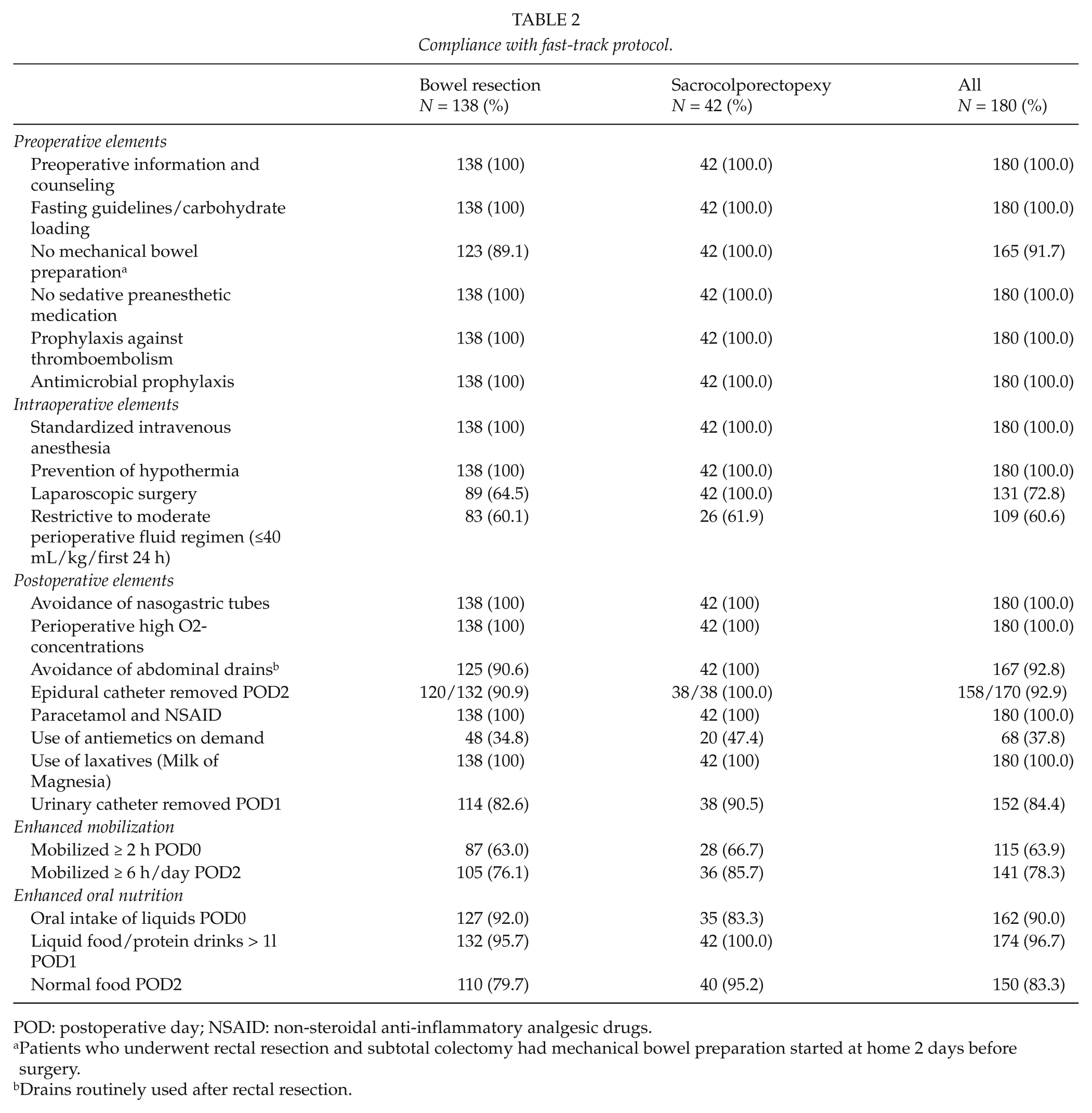
POD: postoperative day; NSAID: non-steroidal anti-inflammatory analgesic drugs.
Patients who underwent rectal resection and subtotal colectomy had mechanical bowel preparation started at home 2 days before surgery.
Drains routinely used after rectal resection.
Functional Recovery
Time to functional recovery was median 2 (IQR 2–3) days after sacrocolporectopexy, small bowel, ileo-colic, and colonic resection, and 4 (IQR 2–5) days after rectal resection and subtotal colectomy. Side-effects of anesthesia and surgery were observed in 37 of the 180 patients (20.6%) during the recovery room period and in 58 patients (32.2%) during the basic ward care within the first 2 postoperative days after surgery ( Fig. 1 ). Paralytic ileus was observed in 6 of the 138 patients (4.3%) who underwent a bowel resection.
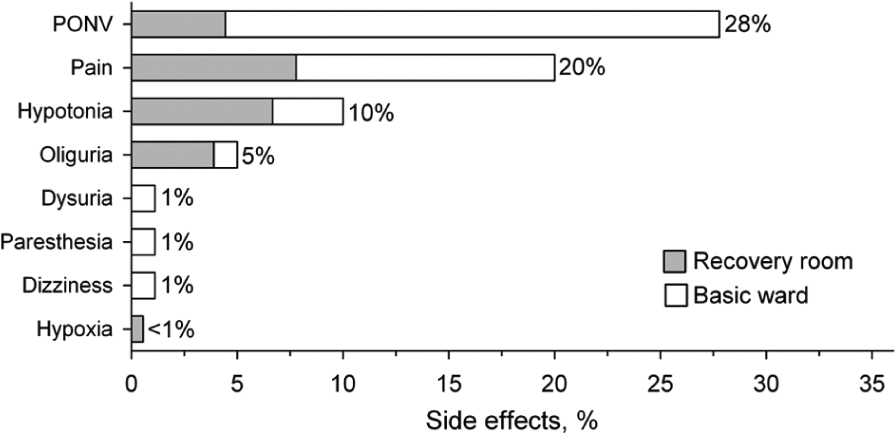
Side-effects of anesthesia and surgery during recovery room period and basic ward care (N = 180).
30-day Morbidity and Readmission Rates
Intraoperative data and short-term clinical outcome are shown in Table 3. There was no mortality. The 30-day postoperative morbidity was 14.5% (95% confidence interval (CI): 9.1–21.5) in patients who underwent bowel resection. Three patients with an anastomotic leak were reoperated and two were managed conservatively with antibiotics. One patient was reoperated for pelvic abscess and one for pelvic hematoma. Two anastomotic bleedings were managed conservatively. Overall reoperation rate was 3.6%. One late ureteral stenosis was treated with nephrostomy and later with stenting. Of the 180 patients, 13 patients (7.2%) were readmitted to hospital within 30-days after surgery: 3 patients with subileus were managed conservatively, one patient was readmitted for anastomotic leak, one for constipation, one for urinary catheter removal, one for the treatment of ureter stenosis, 2 for fever, 2 for abdominal pain, one for dysuria and one for vomiting.
Intraoperative data and surgical outcome.
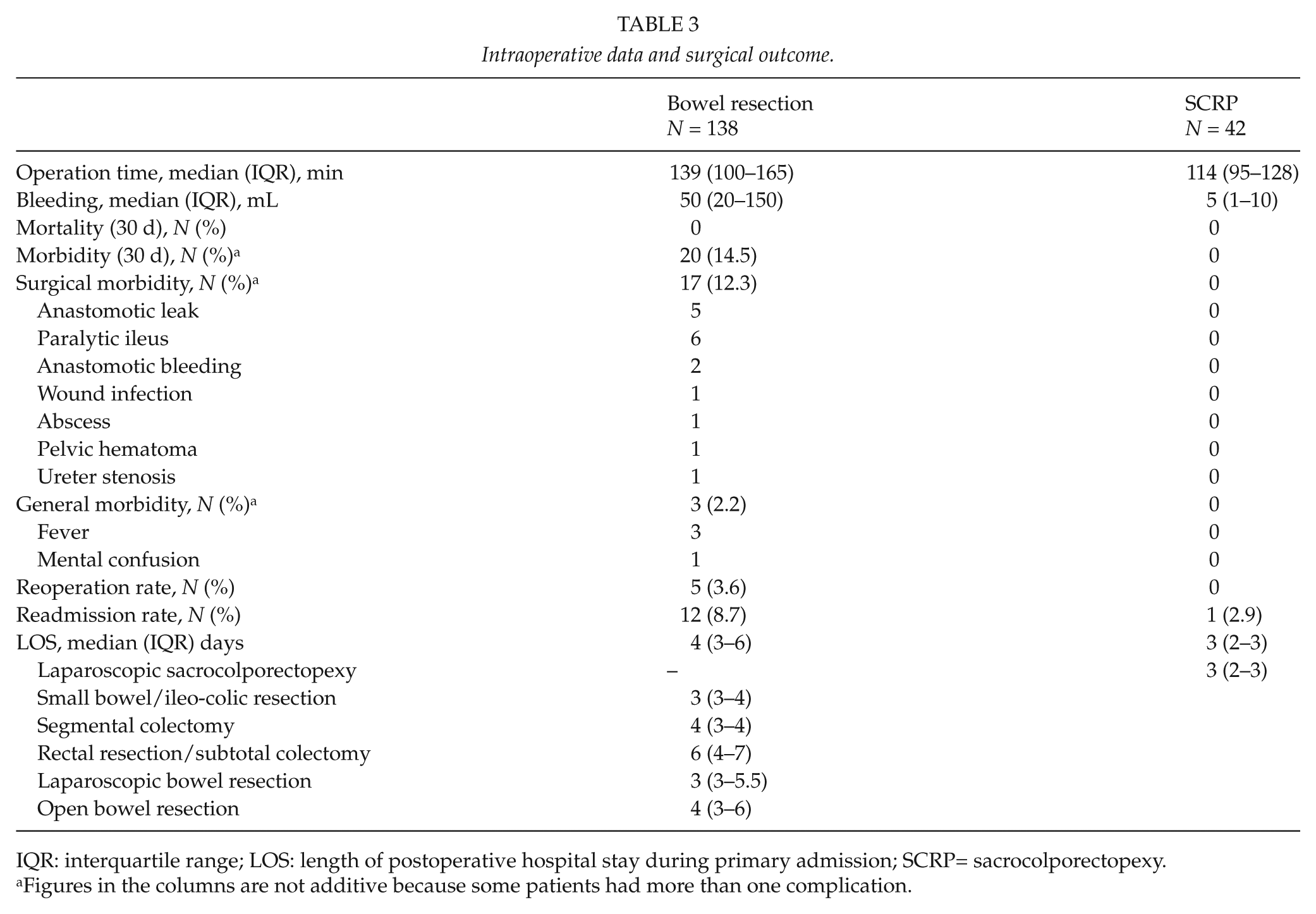
IQR: interquartile range; LOS: length of postoperative hospital stay during primary admission; SCRP= sacrocolporectopexy.
Figures in the columns are not additive because some patients had more than one complication.
Hospital Stay and Patient Satisfaction
Total hospital stay including primary admission–related and readmission-related days was median 6 (IQR 5–7) days. Postoperative hospital stay of all patients during the primary admission was median 3 (IQR 3–5) days: patients younger than 70 years, median 3 (IQR 3–5) days versus those 70 years or older median 4 (IQR 3–4.5) days, P = 0.73; laparoscopic bowel resection, median 3 (IQR 3–5.5) days versus open bowel resection, median 4 (IQR 3–6.0) days, P = 0.060 (Table 3). Of the 180 patients, 78 (43.3%) were discharged later than 3 days after small bowel, ileo-colic, and colon resection and later than 6 days after rectal resection. The reasons were surgeon’s delay (no apparent reason) in 42 of the 78 cases (23.3%), complications in 19 (10.6%), and various other reasons in 17 (9.4%). After discharge, 11 patients (6.1%) were transferred to a general practitioner-guided nursing facility, whereas other patients were discharged home. Patient satisfaction was excellent/good in 70.0%, moderately good in 20.0%, acceptable in 3.9%, and poor in 1.1% of patients. In all, 5 % of the patients gave no answer.
Determinants Affecting Postoperative Hospital Stay
In multivariate model, patient-related characteristics increasing the length of postoperative hospital stay were body mass index > 30 kg/m2 (LOS ratio 1.37 (95% CI 1.14–1.66), P = 0.031) and malignant disease (1.30 (1.12−1.51), P = 0.001). Treatment-related determinants were complexity of surgery (rectal resection and subtotal colectomy 1.61 (1.19−2.17), P = 0.003), recovery of bowel function later than 2 days after surgery (1.49 (1.21−1.85), P < 0.001), time to functional recovery > 2 days (1.34 (1.10−1.62), P = 0.003), general (1.54 (1.00−2.38), P = 0.050), and surgical (2.59 (2.12−3.17), P < 0.001) complications. Protocol compliance–related determinants increasing postoperative hospital stay were removal of urinary catheter later than 1 day after surgery (1.51 (1.24−1.83), P < 0.001), intake of normal food (1.47 (1.16−1.86), P = 0.001), and mobilization ≥ 6 h/day (1.47 (1.07−2.01), P = 0.003) later than 2 days after surgery.
Discussion
This study shows that fast-track protocol for colorectal surgery is effective in reducing the length of hospital stay without compromising patient safety, and results in good patient satisfaction. Patient’s body mass index > 30 kg/m2, malignant disease, complexity of surgery, time to functional recovery > 2 days, recovery of bowel function later than 2 days after surgery, and the presence of general and surgical complications were patient- and treatment-related determinants increasing postoperative hospital stay. Protocol compliance–related determinants were removal of urinary catheter later than 1 day after surgery, intake of normal food, and mobilization ≥ 6 h/day later than 2 days after surgery.
Previous studies have shown that functional recovery can be achieved within 2 to 3 days after laparoscopic or open colon surgery (16, 18). In keeping with that, functional recovery in this study was 2 days after sacrocolporectopexy, small bowel, ileo-colic, and segmental colectomy. Data on functional recovery in high-risk patients, after complex surgical procedures, such as extended colectomies and rectal cancer resections with associated prophylactic stoma and pelvic drainage, are limited (19). In this study, time to functional recovery was prolonged up to 4 days after rectal resection and subtotal colectomy. Postoperative nausea and vomiting are the most frequent side-effects of anesthesia and surgery occurring in some 30% of unselected patients (19, 20). In line with that postoperative nausea and/or vomiting, pain, hypotension, oliguria, dysuria, paresthesia, and dizziness were common side-effects during the early recovery phase but they had no apparent impact on the length of postoperative hospital stay, if appropriately treated. Use of prophylactic antiemetic drugs and dexamethasone given preoperatively has been found to be useful in decreasing nausea and vomiting but were not routinely used in our study. Paralytic ileus (21, 22) commonly seen in some 3%–32% of the patients undergoing abdominal surgery was rarely observed in our study. Chewing-gum therapy and alvimopan, a specific µ-opioid antagonist, are recent innovations to reduce the period of postoperative ileus, although the role of alvimopan after laparoscopic surgery is still controversial (21).
Effective analgesia is a prerequisite to decrease surgical stress response and to enhance mobilization (1). Continuous thoracic epidural analgesia has been considered beneficial in major open abdominal procedures to control pain and to decrease catabolism, paralytic ileus, nausea, and vomiting (1, 22), and was therefore used in most patients in this study. However, a recent study (7) reported no advantage of thoracic epidural analgesia over patient-controlled anesthesia and another study (23) demonstrated a detrimental effect of epidural analgesia on recovery after laparoscopic colorectal surgery when compared with spinal anesthesia or patient-controlled analgesia. Further studies are needed to establish the optimal analgesia in laparoscopic colorectal surgery.
In this study postoperative morbidity was low, but the development of complications had the strongest adverse impact on the length of postoperative hospital stay in line with the results of a national audit report (24). Patient’s body mass index was an independent determinant affecting the length of stay. Obesity is often accompanied by comorbidities and may increase operative difficulties, postoperative morbidity, and the length of hospital stay after open and laparoscopic surgery (25).
The role of laparoscopy to improve the postoperative outcome in the fast-track setting has been controversial (8, 9) but a recent large randomized trial reported a shorter hospital stay and reduced morbidity after laparoscopic than open colonic surgery in the fast-track setting (12). Although 73% of the patients in the present study were operated using laparoscopic technique, our study was not designed to compare laparoscopic and open surgery in the fast-track setting and the type of surgical approach did not emerge as an independent determinant affecting postoperative stay.
Overall postoperative hospital stay in this study was short but an increased length of stay was observed with increasing surgical complexity. Although the day of functional recovery may be considered as a time point to discharge patients, a recent study (16) reported that only a small proportion of the patients were actually discharged on the day of functional recovery in line with our results. In addition, Andersen et al. (17) have shown that readmission rates can be halved from 20% to around 10% by planning hospital discharge 3 days instead of 2 days after colon surgery. In our study readmission rate was well below 10%. Rectal cancer surgery is known to be associated with higher complication rates and longer hospital stay than is colon resection. However, a reduction in the length of stay was found in patients who underwent laparoscopic rectal resection in this study when compared with 8–10 days in other studies (26, 27), although shorter hospitalization time has also been reported (28). Our results are in keeping with Delaney et al. (29), who reported a reduced length of stay among patients who underwent complex pelvic and abdominal procedures such as total proctocolectomies and abdominoperineal resections in the fast-track setting.
Our study has some limitations. The major limitations are weaknesses inherent to the methodology of an observational single-center cohort study, the heterogeneous patient population, and the small sample size. Our results may also reflect the lack of experience during the early phase of implementation. On the other hand, adherence to different fast-track elements and the number of elements applied was higher than usually reported (4–13). Inclusion of patients with different colorectal diseases, with different types of procedures, and elderly patients is also likely to provide a realistic picture of the feasibility of the fast-track care in daily clinical practice. Further research is needed to define the optimal, procedure-specific analgesia in fast-track colorectal surgery.
Conclusion
The effectiveness of fast-track colorectal surgery, as reflected by a relatively good adherence to predefined fast-track elements, low morbidity, reoperation and readmission rates, short postoperative hospital stay, and good patient satisfaction, indicates that our fast-track protocol was successfully implemented and should form the mainstay of elective colorectal surgery.
Footnotes
Declaration of Conflicting Interests
The authors have no conflict of interests to declare.
Funding
This study was funded by the local EVO-funding of Central Hospital of Central Finland.