
Abstract
Introduction:
Obesity represents a vast and rapidly increasing global burden. Bariatric surgery is the only intervention achieving sustained weight loss, among its wide-ranging benefits.
Methods:
In this article, we describe the growing challenges presented by adolescents with severe obesity and review the literature on surgical and other treatment options.
Results:
Outcomes in terms of weight loss, metabolic and quality of life improvement, reversal of obstructive sleep apnea, insulin resistance, type II diabetes mellitus, hypertension, and dyslipidemia appear comparable to those seen in adults. However, long-term data on safety and sustainability are lacking. There is a growing acceptance of the need for surgery as a treatment for the morbidly obese adolescent population, and the number of studies reporting outcomes after adolescent bariatric surgery is increasing.
Conclusion:
Accumulating evidence suggests that the benefits seen in adult bariatric surgery can be reproduced in adolescents. Thus, adolescent bariatric surgery appears to be safe and effective in achieving benefits desired in terms of weight control and improvements in metabolic health and quality of life. However, particular care must be taken when treating a young population, and long-term outcomes are awaited to properly define indications and limitations.
Introduction
Obesity is a major global problem, and the direct costs are significant, but particularly difficult to quantify. This is exemplified by the wide variation in estimates, ranging from 1.9% to 27% of healthcare expenditure (1, 2).
In adults, obesity definitions have been used according to body mass index (BMI), with >25 kg/m2 representing overweight and >30 kg/m2 obesity. However, in childhood, such definitions are more controversial owing to the changes in the growing child and variation in the rates of growth and development. Aligning BMI to growth percentiles has been used to overcome this difficulty.
Prevalence
The prevalence of obesity is rising across the globe, yet some populations, such as Finland, Sweden, the Netherlands, and Japan, have managed to resist the trend more effectively than others (3). Contrary to skepticism regarding genetic influences on obesity, strong genetic susceptibility to obesity has been demonstrated in twin studies (4). Estimates of the prevalence of obesity begin to portray the size and rapid growth of this public health problem, prevalence in adolescents reaching as high as 35.8% in Latin America (5), 18.3% in 11- to 15-year-olds in England (6), and shown to have tripled across two decades to reach 16.5% in the United States (7).
Indeed, increasing numbers of children have reached worrying levels of overweight even within their early years of life. Reports from across Europe and North America have quoted increases of up to 100% in pre-adolescent obesity rates across the 20–30 years from the 1970s and 1980s to the late 1990s (8, 9). In urban areas of China, obesity in children aged 2–6 years rose more than eightfold from 1.5% to 12.6% across just 8 years to 1997 (10), reflecting the global nature of this disease.
Complications
The impact of obesity in adulthood is extensive, and associations between obesity and diseases continue to emerge. In childhood, the most common consequences of obesity are psychosocial, including systematic discrimination, poor self-esteem, and depression, each of which can persist into adulthood (11). Lower academic achievement, as recently observed in obese adolescents, may be related to these issues (12).
The medical consequences of obesity in children are extensive (11), and hospital admissions for obesity have risen fourfold in the United Kingdom from 2000 to 2009 (13). Hyperlipidemia has been widely reported in obese children (14, 15). Childhood hypertension, while rare at <1%, has been estimated to be nine times more common in the obese (11). A ninefold increase in the prevalence of type II diabetes mellitus (T2DM) in childhood has been reported over a 15-year period, with up to 45% of new childhood diagnoses of diabetes being T2DM (16). This increase in T2DM is seen in direct parallel to increasing levels of overweight and obesity in the same populations (16, 17). Additional medical complications related to childhood obesity include obstructive sleep apnea (OSA), pseudotumor cerebri, orthopedic complications, polycystic ovarian syndrome (PCOS), and many others (17). Several of these comorbidities require urgent and aggressive therapy, sometimes the sole intervention required being urgent weight loss (11).
A systematic review examining existing long-term follow-up studies of overweight and obese children in the United States and Europe showed significantly increased risks of premature mortality and morbidity, including diabetes, stroke, coronary heart disease, hypertension, cancer, PCOS, and asthma.
Causes
Multiple factors have been demonstrated as contributory to an individual developing obesity. Profound changes in diet have occurred, with increased access to and reliance upon processed and refined, high-energy food and drink (17). Regular consumption of fast food, high in saturated and trans fats and low in essential fiber, micronutrients, and antioxidants, is associated with obesity. Children are vulnerable to food advertising, even if exposure is brief, and heavy television use was independently associated with higher reported junk food consumption in a study of 919 Australian children (18). Unsurprisingly, family and social factors impact significantly on obesity, including television watching and time spent in physical activity (17).
Slight increases in calorific consumption or small reductions in energy expenditure can lead to marked body mass increases in the long term. An example from Ebbeling et al. (17) showed a potential 50 kg weight gain over one decade from just a single additional serving of sugary drink per day.
Genetic variations causing leptin resistance have been shown to cause an excessive appetite and early obesity in childhood (19), features that reverse entirely with leptin administration. With the public health implications of the profound and far-reaching effects of obesity, effective local, national, and global interventions are urgently required to protect the adults of tomorrow from the real dangers of obesity today.
Treatment Options
Dietary and Lifestyle Interventions
Dietary and lifestyle interventions are wide-ranging and accessible to many. However, reports on such interventions have illustrated the inevitable relapse in most patients who achieve weight loss by these methods (17, 20,21). In fact, some of the most critical review evidence has emerged in recent years, describing up to two-thirds of subjects regaining more weight than was initially lost, observing bias in studies toward showing successful weight-loss maintenance, and describing an absence of consistent evidence of health benefits (21).
In adolescents, modest reductions in obesity have been achieved by intensive interdisciplinary and multimodal dietary/lifestyle approaches (22). In a school-based intervention in Chile, obesity was controlled but not reduced by intensive conservative measures. The interventions addressed both dietary intake and physical activity and were delivered within schools by nutritionists and physical education teachers (23). A recent article from the Swedish National Pediatric register demonstrated an almost absent effect of conservative interventions in adolescents (24).
Pharmacological Interventions
Pharmacological interventions have thus far proved to be of limited value in attempting to achieve significant and sustained weight reduction. The only broadly available obesity drug is the intestinal lipase inhibitor Orlistat. Its mechanism of action is to inhibit gastrointestinal fat absorption by up to 30% (25). However, the translation of this induced malabsorption of fat into weight loss, while statistically significant in some studies, is modest, BMI reductions reported at 4.2 kg/m2 at best (26).
Metformin has also been shown to result in moderate weight and BMI reductions in overweight adolescents (26). Reports on reductions in BMI, including five trials comparing to placebo or baseline, were also modest, with the highest estimate quoting only a 3.2 kg/m2 reduction (26). Clinical guidance in the United Kingdom recommends the use of Orlistat in morbidly obese adolescents with physical or severe psychological comorbidity (27).
Surgical Intervention
The vast body of the bariatric surgical literature relates to adult populations, in which surgery has been the most successful intervention for obesity, achieving considerable weight loss and, importantly, enabling maintenance of weight loss in the long term (28–30). As extensively demonstrated in this issue of the Scandinavian Journal of Surgery, surgery is the only successful approach in adults for sustained weight loss and prevention, induction of remission of comorbidities, and improvement in long-term mortality (28, 31).
Many surgical techniques have been used since the first attempts in bariatric surgery in the 1950s. Traditionally, bariatric procedures have been divided into restrictive (e.g. banding procedures) or malabsorptive (e.g. jejunoileal bypass). However, recent studies demonstrate that procedures such as Roux-en-Y gastric bypass (RYGB) have a complex mechanism of action including changes in appetite signaling as well as in energy expenditure. RYGB is to many the gold standard bariatric procedure with excellent outcomes for excess weight loss, comorbidity resolution, and eating function, with acceptable rates of morbidity and mortality (28).
Surgery in Adolescents
Bariatric surgery is not generally endorsed under the age of 18 years, except in extreme cases. Thus, few reports, mainly case series, exist in the literature on bariatric surgery in adolescents. To date, almost all studies include fewer than 100 subjects.
O’Brien et al. (32) published the only randomized trial between lifestyle intervention and bariatric surgery (laparoscopic gastric banding) for morbid obesity, demonstrating favorable weight loss and improvements in cardiovascular risk factors, as well as improved quality of life in the surgically treated group.
The most recently available pooled data analysis is a meta-analysis performed by Black et al. (33) in the United Kingdom in August 2013, which appears well conducted. It includes studies involving children with an age ranging from 6 to 18 years and examines outcomes across RYGB, sleeve gastrectomy (SG), and adjustable gastric band (AGB) (33). Findings are broadly in line with previous meta-analytical data (34).
The meta-analysis provides good initial evidence in support of surgical intervention. The mean change in BMI at 12 months was −13.5 kg/m2 (95% confidence interval (CI) −15.1 to −11.9). The authors were unable to provide summary estimates for complications in this meta-analysis, but data extracted from the currently available reports show complication rates of 22%−33% for RYGB (35, 36), 4.3% for SG (37), and 10%−48% for AGB (32, 38).
Additional outcomes, summarized from Black’s meta-analysis and the wider literature, are shown by procedure and combined in Table 1 (33, 35–37, 39 –51). Direct comparison between adolescent and young adult populations (<18 vs 18−21 years) has shown comparable reductions in BMI (52), with RYGB shown as the most effective procedure. The largest series of adolescents undergoing RYGB showed a BMI reduction of 13.3 kg/m2 at 2 years, with 93% achieving >50% excess BMI loss (36).
Short-term outcomes following bariatric surgery in adolescents.
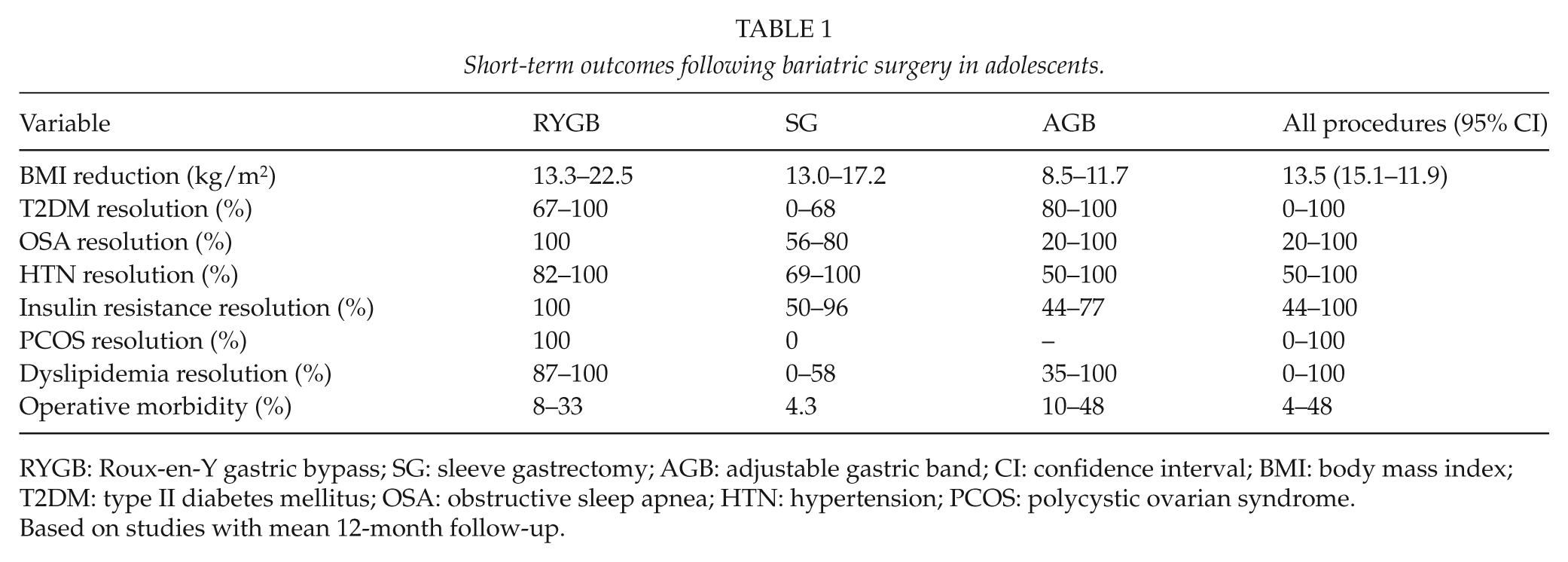
RYGB: Roux-en-Y gastric bypass; SG: sleeve gastrectomy; AGB: adjustable gastric band; CI: confidence interval; BMI: body mass index; T2DM: type II diabetes mellitus; OSA: obstructive sleep apnea; HTN: hypertension; PCOS: polycystic ovarian syndrome.
Based on studies with mean 12-month follow-up.
Results on resolution of comorbidities at 1 year vary widely across the literature, as illustrated in Table 1. From studies reporting follow-up of hypertension, OSA, T2DM, insulin resistance, PCOS, and dyslipidemia, most comorbidities resolved within the first postoperative year following RYGB (Table 1). Resolution rates following AGB were wide-ranging, and very limited data were available on SG (Table 1). A recent article including subjects aged 5–21 years offered some further insight into outcomes following SG in young patients, with the vast majority of subjects experiencing resolution of OSA (91%), prediabetes (100%), T2DM (94%), prehypertension (83%), hypertension (75%), and dyslipidemia (70%) (39). A further article from France showed similar outcomes at 2 years in a cohort of 61 patients aged 18−20 years, bariatric surgery being prohibited for under 18-year-olds in France (53).
With available reports generally containing few subjects and limited follow-up, the encouraging figures given must be treated with caution. In the study with the most long-term follow-up, the generally sparsely performed malabsorptive procedure, biliopancreatic diversion (BPD) was used. A longitudinal observation of 76 adolescents aged mean 16.8 (range 14−18) years for a mean duration of 11 (range 2–23) years revealed that prolonged weight loss was achievable, with 78% excess weight loss at longest follow-up. Comorbidity resolution was impressive, with 100% resolution of diabetes and dyslipidemia and >80% resolution of hypertension (54). This article also gives a good insight into the evolution of a bariatric procedure and the associated improvement in outcomes as the authors concluded that the incidence of protein malnutrition improved across the study, albeit including adult patients (54).
Concerns
Operative Morbidity and Mortality
Surgery is not without risk, and while we know the mortality in adults across all procedures to be 0.22%–0.34% (95% CI) (31, 55), a similar risk in the adolescent population is likely to be more difficult to accept. The death of a child is an exceptionally emotive and complex issue, with profound and lasting psychological and social implications for the family (56) and recognized impact upon the clinicians involved. In the literature to date, we could find only one single report of operative death following bariatric surgery in the “adolescent” population (57), although this was in a 19-year-old male and could therefore actually be classed as adult. Regardless of age, the operative death of this young male provided an important lesson on concomitant cardiovascular disease and its potentially lethal complications in bariatric surgery in the young (57).
Nutritional deficiencies commonly exist in adolescents with severe obesity before bariatric surgery and often persist in the postoperative population (58). Protein deficiency predominates among the macronutrient deficiencies potentially encountered. However, micronutrient deficiencies are more common, including trace elements, essential minerals, and water-soluble and fat-soluble vitamins. Surgical sequelae, such as small intestinal bacterial overgrowth, can promote such deficiencies, especially in patients with T2DM (58).
Dumping syndrome is related to the rapid transit of calorie-dense food into the small bowel following the removal of normal anatomical sphincter-controlled gastric emptying. It is characterized by symptoms including tremor, sweating, palpitation, fatigue, and diarrhea (59). Some consider this a positive result of surgery as it introduces a powerful feedback mechanism for avoidance of wrong foods.
Concerns have been raised regarding the potential impact of micronutritional deficiencies, both in the preconception period and during pregnancy, upon maternal and fetal health. It has been suggested in the United States that testing for such deficiencies is underperformed, although the prevalence of these deficiencies in preconception and pregnant women is unknown. With an appreciable increase in fertility representing one of the myriad benefits of surgery (60), counseling regarding folic acid and other nutritional supplementation is important in female adolescents undergoing obesity surgery. Specific concerns have been raised regarding iron deficiency anemia, which is a substantial risk in girls at reproductive age.
Of real importance in contextualizing these risks are the well-documented benefits to maternal and fetal outcome that result from bariatric surgery, with significantly lowered rates of gestational diabetes and eclampsia and no increase, or even a reduction in risks to the neonate (60).
Concern exists regarding the impact of bariatric surgery on the skeleton. There is objective evidence of reduced bone mineral density and bone mineral content within a year following gastric bypass surgery (61), requiring counseling, monitoring, and nutrient and mineral supplementation. The potential impact remains unknown, and particular attention is therefore needed, especially in young patients.
A recent review has drawn attention to the increased risks of re-operative surgery (62), as seen across most domains of surgery. The implications of this will become more apparent from long-term follow-up studies in the adult population in coming years, and similar studies in adolescent populations will provide the evidence of its true implications.
The anatomical implications of some bariatric procedures can include relative inaccessibility of parts of the gastrointestinal tract by conventional methods. This presents difficulty in diagnostic and therapeutic approaches such as gastroscopy or endoscopic cholangiography. However, in response to these challenges, novel approaches and techniques have been proposed and developed, including computerized tomography virtual gastroscopy (62), double-balloon techniques for enteroscopy after RYGB (63), and even prophylactic cholecystectomy, which subsequently lost support following meta-analysis (64). Additionally, reversal of the RYGB has been reported as technically feasible, without significant complication in the short term (65).
Particular Considerations in Adolescent Obesity Surgery
There is wide agreement that non-surgical options should be explored first, including lifestyle interventions and behavioral modification (27, 66), in a stepped-care approach. Consideration of the adolescent’s motivation to lose weight may be of importance in the selection process. Particular consideration of the family situation, home environment, and motivations of the parents are important additional factors for assessment of the adolescent patient enabling postoperative support. However, there are no studies demonstrating a correlation between patients’ motivation and outcome.
An experienced multidisciplinary team (MDT) is important, especially in the adolescent group in relation to psychological issues such as dietary control, self-esteem, coping, and emotional eating (52). The members should include a suitably qualified and experienced pediatrician, surgeon, adolescent/child psychologist, pediatric nutritionist, exercise physiologist or physical therapist, nursing support staff, and a patient coordinator. A social worker can also prove helpful.
Psychiatric disorders have been shown to be commonplace among adult bariatric surgical candidates, with reported prevalence ranging from 20% to 60% (67), in particular mood, anxiety, and eating disorders (68). Higher rates of psychopathology have been reported in surgical candidates than in obese individuals in the community or, indeed, those seeking community-based weight-loss treatments (69).
Direct links have been widely demonstrated between severity of obesity and specific psychopathology, including depression and binge eating (68). Additionally, the physical illness associated with obesity is likely to predispose obese individuals to such psychiatric disorders (68).
However, little is known about the impact of bariatric surgery on psychological health in the adolescent. From the limited reports available, there is agreement that adolescents seeking weight-loss surgery demonstrate higher levels of depressive symptoms (70, 71) and impaired health-related quality of life (70, 71).
A study from our own unit examined psychological outcomes in 37 adolescents, comparing psychological health at baseline and again at 4 years following RYGB (72). Our results confirmed a difference between preoperative and follow-up psychological state. Significant self-reported improvements in anxiety, depression, and self-concept were evident, as well as non-significant reductions in anger and disruptive behavior (72).
High rates of suicide are observed in post-bariatric surgery populations, and a 2% rate of attempted suicide was observed in adolescents in the 2 years after bariatric surgery (36). This emphasizes the need for particularly heightened attention to support potentially vulnerable adolescents, as well as the real need for research exploring factors associated with and contributing to this risk.
A number of endocrine and other genetic syndromes can cause obesity in the adolescent, the commonest being Prader–Willi syndrome (PWS) (73). These must be considered in any assessment program for surgical obesity intervention, although reports of successful surgery in PWS have begun to emerge (39).
The required duration of action of a bariatric procedure in an adolescent is anticipated to be decades longer than in adult bariatric patients. Therefore, long-term outcomes are of particular importance.
Guidelines and recommendations have emerged, taking into account the available evidence (74 –78). They are drawn mostly from experience in the adult population, and the recommendations set out by the US National Institutes of Health (NIH) for adults with severe obesity (79) remain applicable today. Recent iteration has incorporated the limited but growing body of Level 1–4 evidence, with an inevitable reliance in part on Level 5 evidence. These are incorporated into a summary of existing guidance, given in Tables 2 and 3.
Criteria for adolescent bariatric surgery.
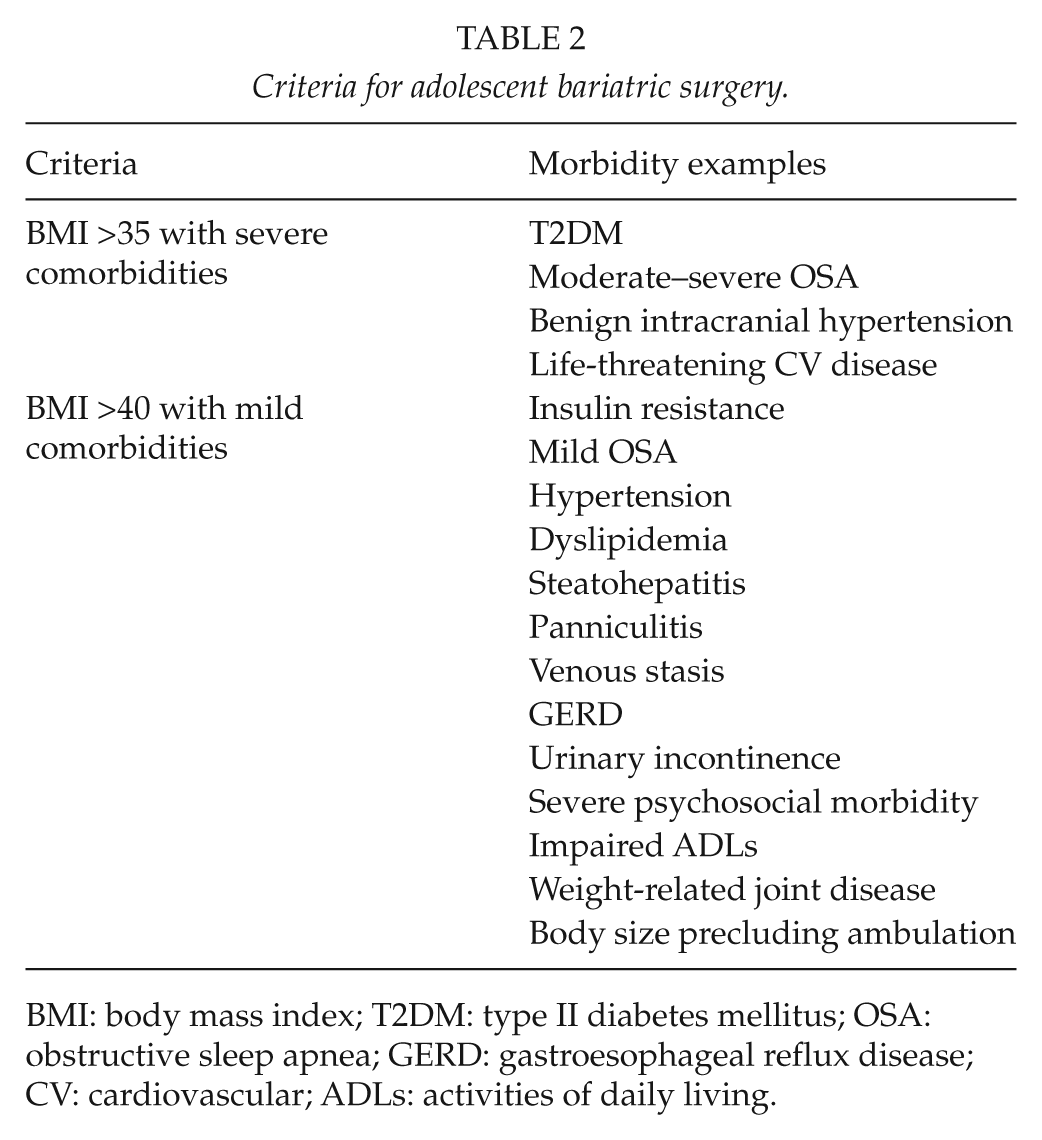
BMI: body mass index; T2DM: type II diabetes mellitus; OSA: obstructive sleep apnea; GERD: gastroesophageal reflux disease; CV: cardiovascular; ADLs: activities of daily living.
Pre-requisites for adolescent bariatric surgery.
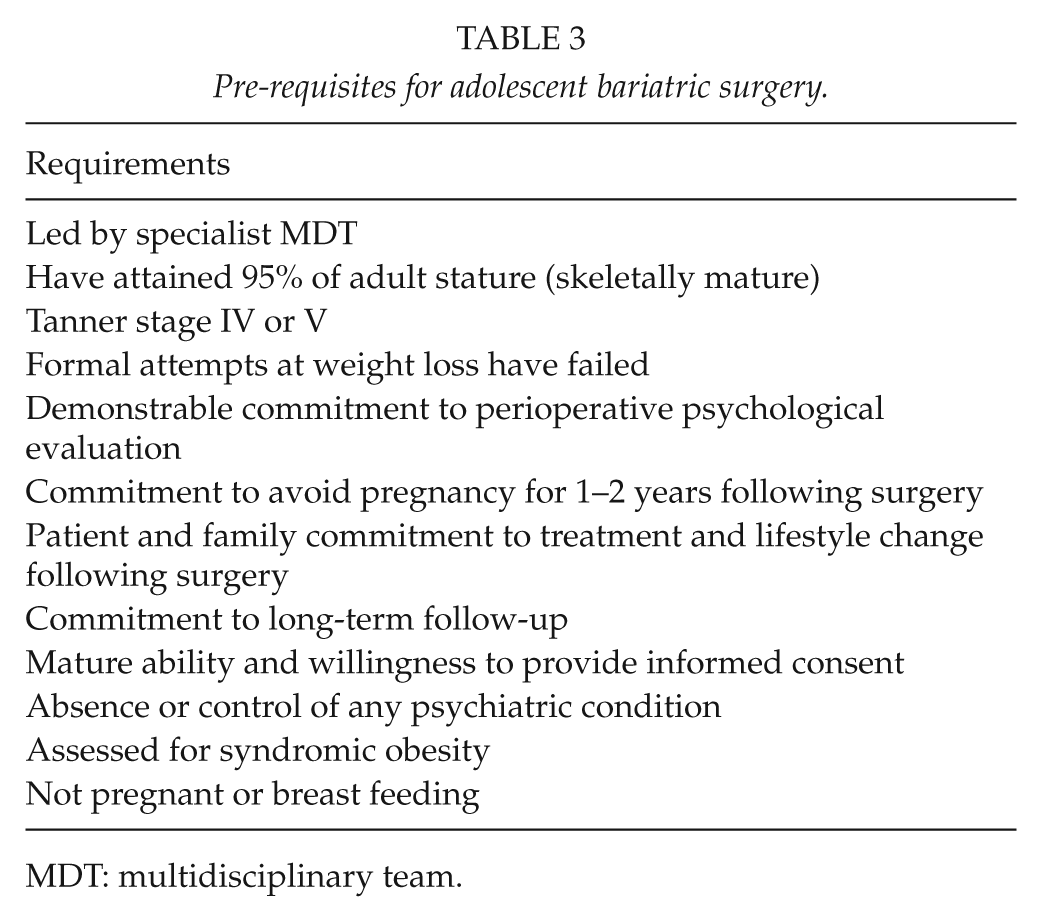
MDT: multidisciplinary team.
Considerations Regarding Choice of Surgical Technique
Data are currently insufficient to make any recommendations regarding preferred surgical technique in adolescents. In most series, surgeons appear to use the same surgical techniques for adolescents as those used in adults. As mentioned, the results in adolescent series regarding weight loss appear to replicate results in adults. Thus, the variability in weight loss is greater in series using AGB (32), while in series using complex bariatric techniques, greater and more predictable weight loss is observed (36). Long-term results will be pivotal in adolescents owing to the inherent requirement for sustained effect over many decades.
An argument used in favor of AGB is the reversibility of the procedure. Conversely, surgeons preferring RYGB argue that a superior long-term weight control and favorable dietary compliance suggest this technique should suit adolescents best. The relatively new bariatric technique, SG, has also been shown to be a viable option in adolescents, with short-term weight outcomes resembling those after RYGB. A possible advantage may be lower risk for long-term nutritional deficiencies, although long-term weight outcome remains unclear. The resection of stomach and inability to restore the anatomy after SG could also be regarded as a disadvantage with this technique.
Our Experience From the Swedish Adolescent Morbid Obesity Surgery Study
A Swedish nationwide study within our unit is addressing the safety and efficacy of using laparoscopic RYGB in severely obese adolescents. Patients have been followed for up to 5 years postoperatively, and data regarding 2-year outcomes of weight loss, comorbidity, and quality of life, as well as adverse events up to 5 years, are published (36, 80).
RYGB was used as the intervention, recognizing the superior sustainability of the procedure and in the absence of evidence of age-related negative effects. In parallel, a conventionally treated, matched adolescent group and a third group, comprising matched adults undergoing the same surgery, have been followed. Our inclusion and exclusion criteria were aligned to the recommendations discussed earlier in this review (Tables 1 and 2) and have been described in previous reports (36, 80).
Details of the Patients
In total, 82 adolescents were recruited between February 2006 and April 2009, each having completed a comprehensive conventional treatment program for at least 1 year and following formal assessment by a dedicated pediatrician, psychologist, and dietician. One patient refused surgery on the day of the operation; thus, 81 individuals (35% boys) underwent surgery.
The control groups comprised 81 conservatively managed adolescents (43% boys), selected from the Childhood Obesity Register in Sweden (BORIS), and 81 gender-matched obese adults (aged 35–45 years) undergoing gastric bypass, within ±1 month of the operated adolescents.
In the adolescent surgical group, 25 (31%) had neuropsychiatric diagnoses, 13 (16%) had existing or previous self-destructive behavior, and 33 (41%) had contacts with pediatric psychiatric units. Poor school performance (truancy, leaving school without a diploma) was frequently reported (>50%). A total of 26 adolescents (32%) had no recorded psychosocial problems.
Outcomes
Median surgical time was 63 min (range 38–106 min) in the adolescent group. Median postoperative inpatient stay was 4 days (range 2–11 days). Three minor complications occurred (80).
There was a 100% follow-up rate at 1 and 2 years for weight and height in both groups undergoing surgery. In the conventionally treated adolescent group, there was a 100% follow-up for weight after 1 year, but this dropped to 73% (59 individuals) after 2 years. There were similar reductions in weight over 2 years in surgically treated adolescents (−32%; CI, −35% to −30%) and in adults undergoing surgery (−31%; CI, −34% to −29%). An excess weight loss greater than 50% was achieved by almost all (95%) operated adolescents. Conversely, a weight gain of 3% (CI, 0%–7%) was observed in the conventionally treated adolescents.
There were no significant differences in weight loss between genders. Of the adolescents in the surgical group, 57% had a continuing weight loss, while 43% increased in weight during the second year after surgery (range −9·7 to +4·2 kg).
We found substantial and broad improvements in cardiovascular risk factors, including glucose metabolism, blood lipids, inflammatory markers, as well as systolic and diastolic blood pressure. After 2 years, significant quality of life improvements compared to baseline were evident in all four physical health domains, in the physical component summary score, and in two of the four mental health domains. Minor decreases in SF-36™ (QualityMetric Inc., Lincoln, RI, USA) scale scores between 1- and 2-year follow-up did not reach statistical significance.
Levels of iron, vitamin D3, and vitamin B12 increased at a group level over the 2 years, but some adolescents developed deficiencies. The adherence to suggestions for supplementation was generally low.
Adverse Events
During the 2-year follow-up, 12 adolescents (15%) underwent additional surgical interventions. Surgery for internal hernia and cholecystectomies dominated. Five patients (6%) required surgery for internal hernia (three behind jejunojenunostomy and two at Petersen’s space), and five (6%) underwent cholecystectomy due to symptomatic gallstones. One patient was laparoscopically operated with a finding of adhesions and another underwent emergency laparotomy due to abdominal pain without obvious pathology. Four others (5%) visited an emergency ward due to non-specific abdominal pain.
Somewhat surprisingly, most adolescents experienced problems with excessive skin following weight loss. Some 80% expressed a wish for plastic reconstructive surgery, and the complaints were equally common among boys and girls.
Six patients (7%) had periods of impaired psychiatric health. Two girls attempted suicide with medication overdoses, one (aged 15) suffered from continued bullying, and the other (aged 16) had persistent depression and anxiety. An 18-year-old boy demonstrated self-destructive behavior and expressed suicidal ideation. Three girls were referred to an adult psychiatric unit due to depression and anxiety. No psychiatric adverse event occurred in patients who were mentally healthy at baseline.
In addition, five patients (5.2%, three girls and two boys) reported excessive use of addictive substances (drugs and alcohol) postoperatively. All of them had an existing, but hidden, addiction at inclusion.
No psychosocial adverse event occurred in patients who were mentally healthy at baseline, and there was, therefore, no indication that surgery was associated with debut of psychosocial illness among adolescents without any psychological morbidity before surgery.
In summary, the Adolescent Morbid Obesity Surgery (AMOS) project demonstrates that gastric bypass surgery results in similar weight loss in adolescents with high prevalence of psychopathology as in adults over 2 years. Furthermore, we found a substantial improvement in cardiovascular risk factors and quality of life. Nonetheless, the psychiatric adverse events appearing in this psychosocially vulnerable cohort require careful attention and might indicate limitations of the surgical strategy.
The Future
Although bariatric surgery has been used for several decades in adults, it is a comparatively young field of specialization. The literature base is growing rapidly, but remains thin in relation to adolescent surgery. Future studies must build on these promising findings, with randomized controlled trials incorporating long-term follow-up. It will be important to collaborate across international borders sharing practice and experience in order to refine surgical technique and MDT approaches.
Conclusion
The literature is emerging regarding bariatric surgery in adolescents, but remains limited at present. Based on existing evidence, bariatric surgery appears to offer substantial weight loss and improvements in health and quality of life resembling those reported in adults. Studies to determine long-term outcome and quantify the benefits to society and healthcare budgets are warranted.
Bariatric surgery is certainly not the only answer to tackle the obesity epidemic in adolescents, and effective prevention and conservative treatment strategies are urgently needed. However, bariatric surgery appears to offer significant benefits for adolescents suffering from severe obesity.
Footnotes
Declaration of Conflicting Interests
None declared.
Funding
This research received funding from the Royal College of Surgeons of England (A.J.B.) and the Swedish Research Council (T.O.).