
Abstract
Background and Aims:
Periprosthetic supracondylar fractures after total knee arthroplasty are often associated with poor bone stock, fracture comminution, and loose components. Current operative methods include plating, intramedullary nailing, and re-arthroplasty, depending on the fracture type. The aim of the study was to assess the outcome of operatively treated periprosthetic supracondylar fractures at our institute with special interest on the use of strut grafts in association with plating.
Materials and Methods:
In all, 68 patients were included in the study. They had been treated operatively due to a periprosthetic supracondylar fracture at our center between 2000 and 2010. The data of these patients were retrospectively collected from the electronic patient archives. Fractures with a fixed prosthesis component were treated using internal fixation provided that there was enough bone for osteosynthesis in the distal fracture fragment (39 patients). Fractures with a loose prosthesis component were treated using re-arthroplasty (29 patients). The demographics of the two treatment groups did not differ statistically significantly. Death or any re-operation was chosen as the endpoint of follow-up. Cumulative survival percentages were estimated for each treatment group.
Results:
There was no statistically significant difference between the treatment groups regarding clinical outcome. Clinical outcome was not assessable in nine patients. A positive clinical outcome was reported in 52 cases (88.1%). The survival of both laminofixation and re-arthroplasty was 75% at 3 years, but the survival of laminofixated fractures with strut graft was 80% compared to that of 51% without strut grafts. In all, 16 patients (24%) had a post-operative surgical site complication: seven infections (10%), six non-unions (15%), and three patellar dislocations (11%).
Conclusions:
Post-operative surgical site complications were relatively common in these mainly elderly female patients. The survival percentages of the re-arthroplasty and laminofixation groups were similar. The use of strut grafts in association with plating may decrease re-operation rate.
Keywords
Introduction
Periprosthetic fractures of the distal femur are a relatively rare complication following total knee arthroplasty (TKA). There is only limited knowledge about the incidence of these fractures, but previous studies show incidence ranges from 0.3% to 2.5% (1–3). However, as the number of performed TKAs rises and average lifespan increases, the incidence of periprosthetic fractures of the distal femur could expect to rise. They usually result from low-energy injuries such as falling from a standing position. Several predisposing factors have been associated to them including high age, female sex, osteoporosis, smoking, rheumatoid arthritis and other diseases treated with systemic corticosteroids, cardiovascular and neurological diseases, previous revision arthroplasty, and anterior femoral notching during the primary TKA (4 –6). The role of anterior femoral notching has been disputed, but there is a consensus that it should be avoided (7, 8).
Development of modern fixation techniques such as locking plates has altered the treatment of these difficult fractures. Current operative methods include plating, retrograde intramedullary nailing, and re-arthroplasty, depending on the fracture type (3, 5, 9). Structural onlay allografts can be used in association with plating to further stabilize the fracture and enhance the bone stock. Strut grafts become re-vascularized and incorporated into the surrounding bone tissue if the fit is stable (9).
The aim of our study was to assess the outcome of operatively treated periprosthetic fractures of the distal femur at our institute with special interest on the use of strut grafts in association with plating.
Material and Methods
From 2000 to 2010, 69 patients with a previous TKA were operatively treated at Turku University Hospital due to a periprosthetic fracture of the distal femur. After approval of the study protocol by the Ethical Committee of the Hospital District of Southwest Finland, the data of these patients were retrospectively collected from the electronic patient archives and followed up. Death or any revision surgery was chosen as the endpoint of follow-up. From those, 39 patients were treated by plating and 28 were treated by re-arthroplasty. One patient was treated simultaneously by plating and re-arthroplasty, and was categorized as re-arthroplasty. Only one patient was treated by retrograde intramedullary nailing and was excluded from the study. Thus, 68 patients were included in the study with 39 patients in the plating group and 29 in the re-arthroplasty group.
The patients were divided according to the operative method into two groups: plating and re-arthroplasty. The patients’ periprosthetic fractures were categorized according to Rorabeck classification—Type I: non-displaced with an intact prosthesis, Type II: displaced with an intact prosthesis, and Type III: displaced or non-displaced but with a loose prosthesis component (10). Also the operation duration, American Society of Anesthesiologists (ASA) class, post-operative surgical site complications, clinical outcome, possible re-operations, and medical co-morbidities such as coronary heart disease or heart failure, diabetes, osteoporosis, rheumatic diseases, alcoholism, and neurological conditions were recorded.
The demographic data of the study patients are presented in Table 1. The mean age of the patients was 79 years (range 43–95). Of the patients, 10 (15%) were men. Neither ASA classification nor the prevalence of any medical co-morbidities differed significantly between patients treated by plating compared to those treated with re-arthroplasty. According to the Rorabeck classification, there were 6 Type I fractures, 45 Type II fractures, and 15 Type III fractures. Data of two patients’ fracture classification were not available. Of the 66 cases with fracture classification available, all Type I fractures were treated by plating whereas all Type III by re-arthroplasty. Of the 45 Type II fractures, 33 were treated by plating (73.3%) and 12 (26.7%) by re-arthroplasty (6, 10). Strut grafts were used in 33 (84.6%) of the 39 platings and in 5 (17.2%) of the 29 re-arthroplasties.
The demographics, fracture type, use of strut graft, ASA class, mean operation duration, and co-morbidities of the study patients.
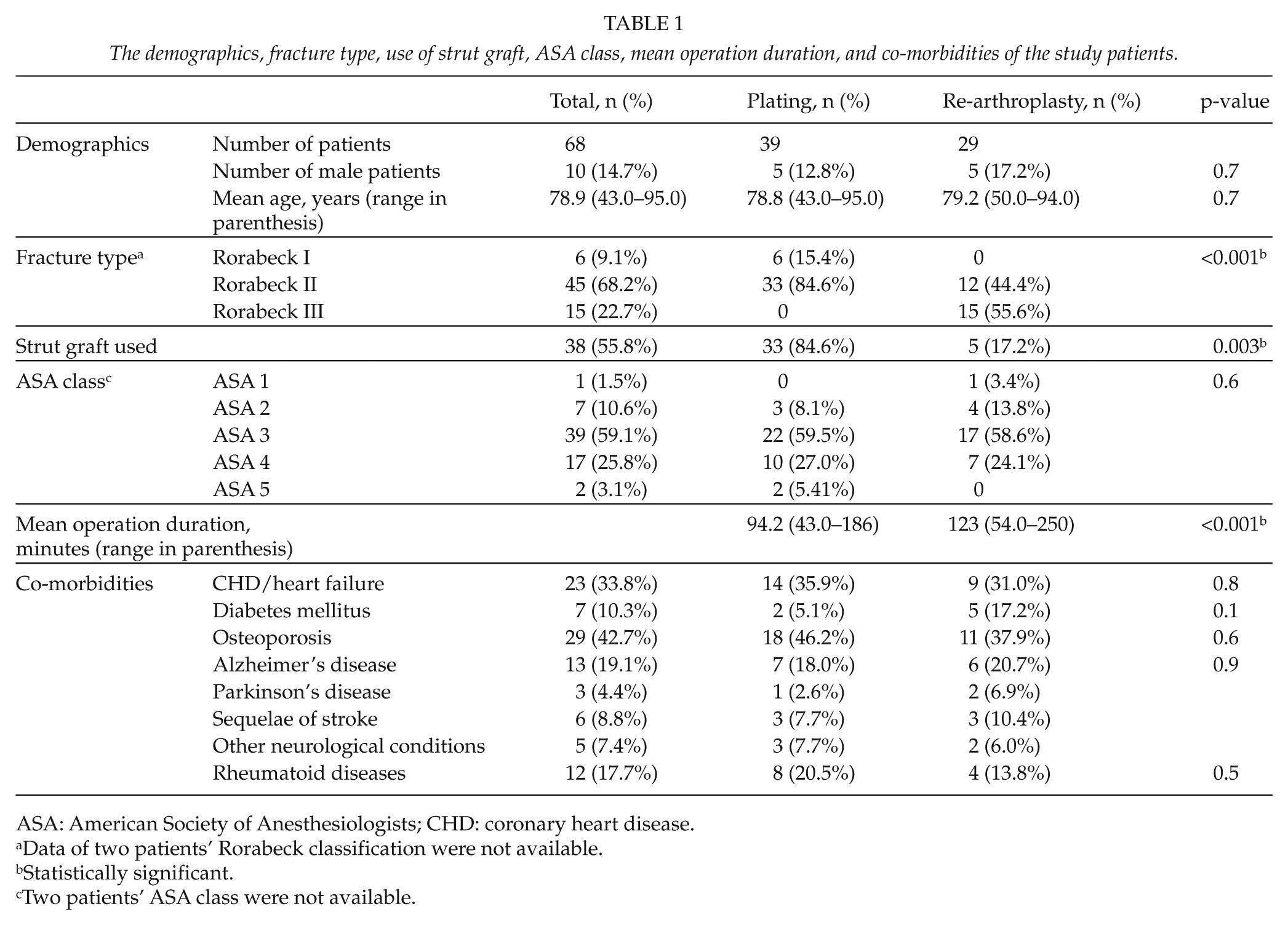
ASA: American Society of Anesthesiologists; CHD: coronary heart disease.
Data of two patients’ Rorabeck classification were not available.
Statistically significant.
Two patients’ ASA class were not available.
We collected data of post-operative mobilization and weight bearing for each patient. It is our standard procedure that all revision TKAs have immediate full weight-bearing and immediate mobilization, pain permitting. Patients treated by laminofixation with or without strut grafts generally have 6 weeks of light or no weight bearing. All patients in the study conformed to this weight-bearing schedule.
Post-operative surgical site complications were categorized as infection, fracture non-union, and recurrent dislocation of the patella. All cases of radiological non-union, plate failure, and continuing pain leading to re-fixation were classified as non-union.
The clinical outcome was evaluated based on information of radiological outcome, subjective pain, knee stability, flexion and extension restrictions, and pre- and post-operative ambulatory capability. Each case was individually assessed with regard to pre-injury state and aim of treatment, and the clinical outcome then categorized as excellent, satisfactory, dissatisfactory, or initially satisfactory but followed by a re-operation. Each patient’s ability to live at home before and after the treatment was also evaluated.
Statistical analyses were carried out using SAS system for Windows, Version 9.3 (SAS Institute Inc. Cary, NC, USA). Continuous variables were characterized by mean values and range whereas categorical variables by frequency or percentages. Differences in background variables between treatment methods were tested using the Mann–Whitney U-test in continuous variables and using the chi-square or Fisher’s exact test in categorical variables. Cumulative survival percentages were estimated by the Kaplan–Meier technique. Follow-up time was calculated from the operative treatment due to a periprosthetic supracondylar fracture (PSF) to death or revision surgery. Cox proportional hazard models were used to test the difference in survival between operation techniques. Results are presented using hazard ratios (HRs) with 95% confidence intervals (CIs). P-values less than 0.05 were considered statistically significant.
Results
The data of clinical outcome and post-operative complications are presented in Table 2.
Data of clinical outcome, gained form of ambulation, complications, revision surgery, death during follow-up, and mean follow-up time.
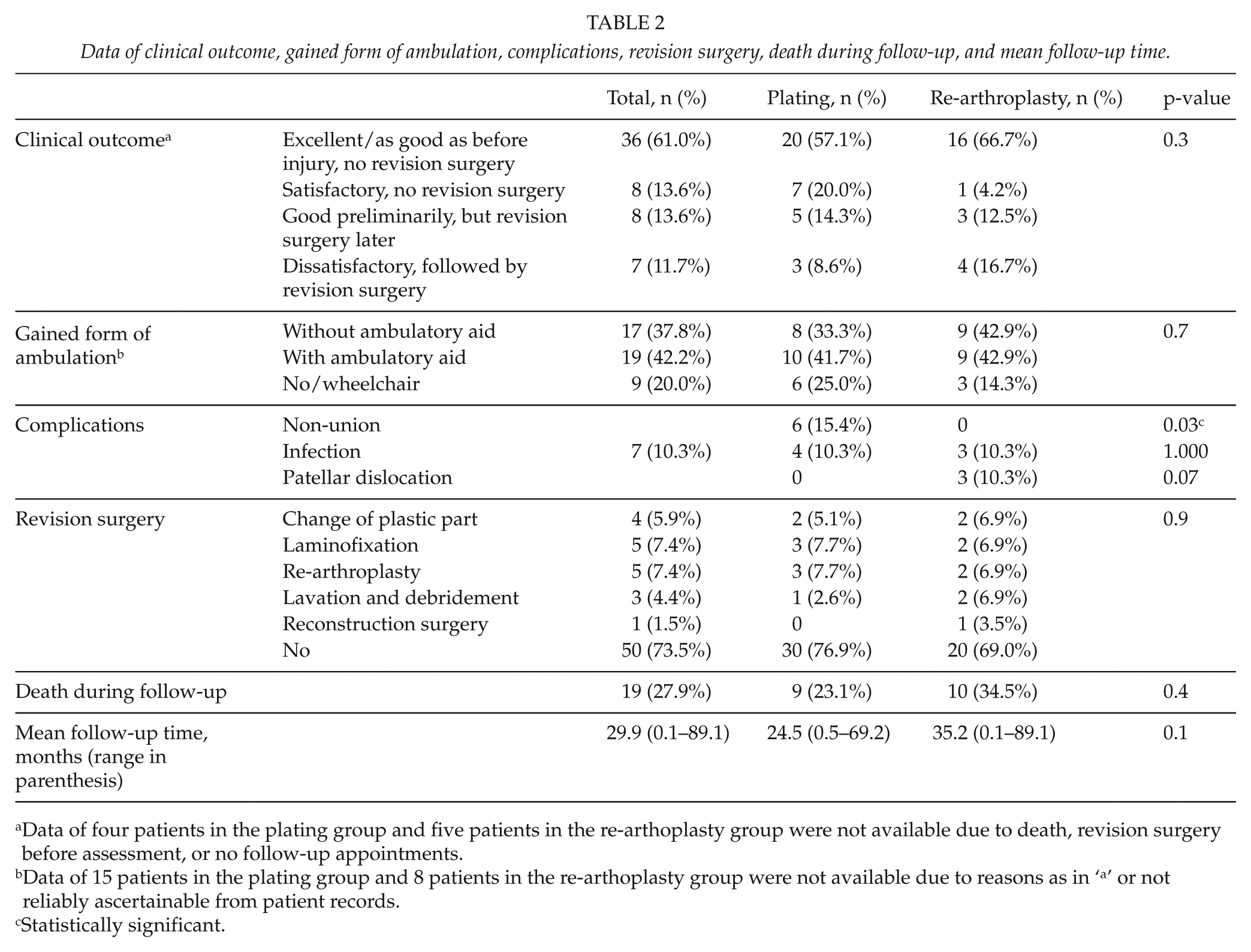
Data of four patients in the plating group and five patients in the re-arthoplasty group were not available due to death, revision surgery before assessment, or no follow-up appointments.
Data of 15 patients in the plating group and 8 patients in the re-arthoplasty group were not available due to reasons as in ‘a’ or not reliably ascertainable from patient records.
Statistically significant.
There was no statistically significant difference between the treatment groups regarding clinical outcome. A positive clinical outcome was reported in 52 (88.1%) cases: excellent in 36, satisfactory in eight, and initially good in eight cases which later had a re-operation. In all, 55 (79%) patients had lived at home before the index procedure, and only 4 (7%) of these patients were eventually not able to return home but had to be institutionalized. See case examples (Figs 1 and 2).

Pre- and post-operative radiographs of a female patient, 74, who had fallen on her knees and suffered a distal Rorabeck type II fracture. A total of 12 months after re-arthroplasty a.m. GMRS (global modular replacement system) she was pain-free and walking without ambulatory aid.

Pre- and post-operative radiographs of a female patient, 87, who had fallen at home and suffered a Rorabeck type II fracture. A total of 4 months after open reduction and laminofixation with a cortical strut graft, she was pain-free and walking with a walker device. The patient was rehabilitated to pre-trauma condition and was able to continue to live at home.
Survival analyses in both the plating and re-arthroplasty group showed an initial decline to about 75% during the first six post-operative months, which was followed by a clear plateau during a 36-month follow-up period (Fig. 3). The difference in survival between groups was non-significant (p = 0.729, HR = 1.19, 95% CI: (0.46, 3.09)). A similar analysis was performed for the plating with the combined strut graft group and the plating-only group (Fig. 4). The strut graft group reached a plateau at 80%, but the plating-only group continued down to 50%. This difference was non-significant (p = 0.108, HR = 3.12, 95% CI: (0.78, 12.50)).
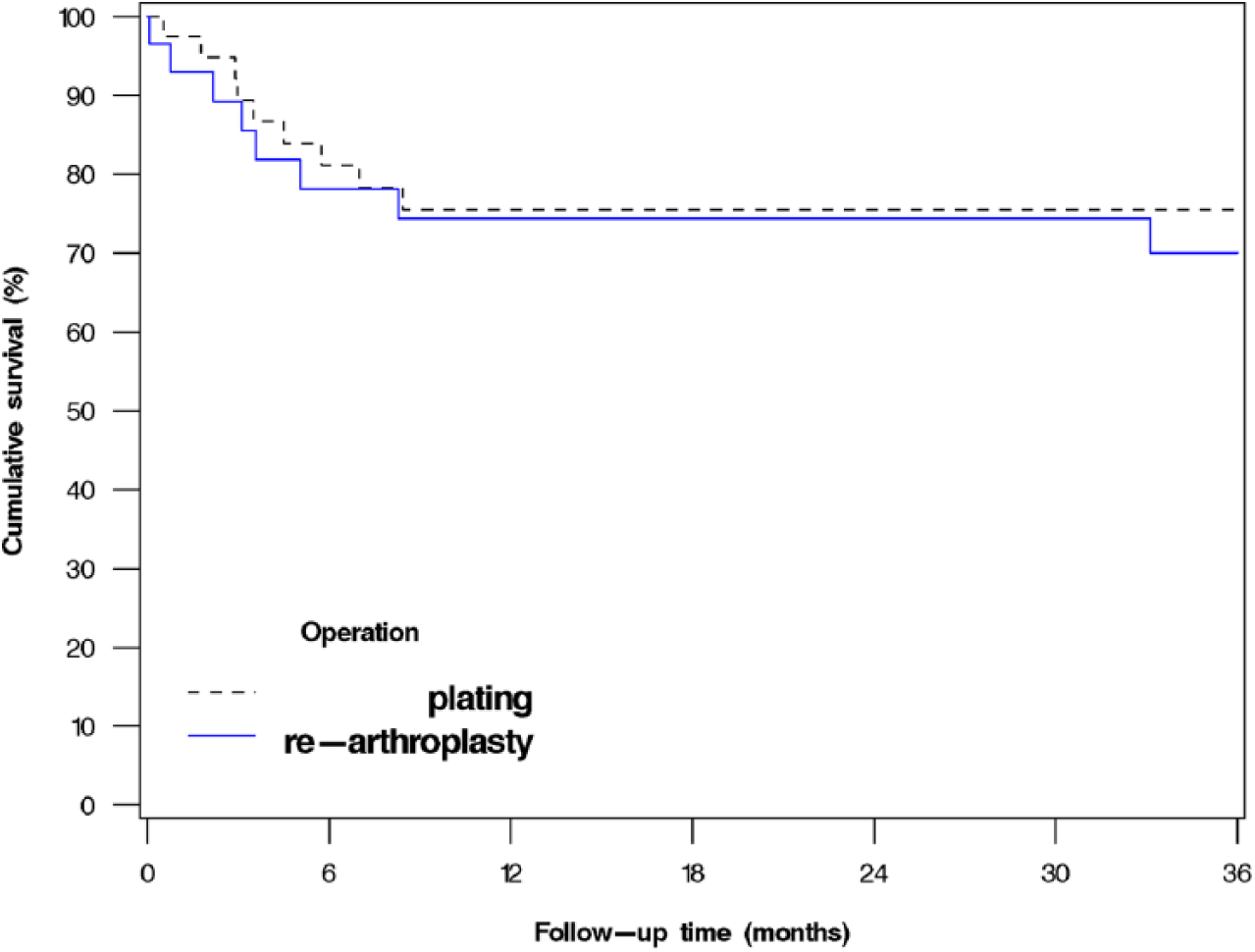
Cumulative survival of plating and re-arthroplasty groups with re-operation for any reason as the endpoint (n = 68, p = 0.729, HR = 1.19, 95% CI: (0.46, 3.09)).
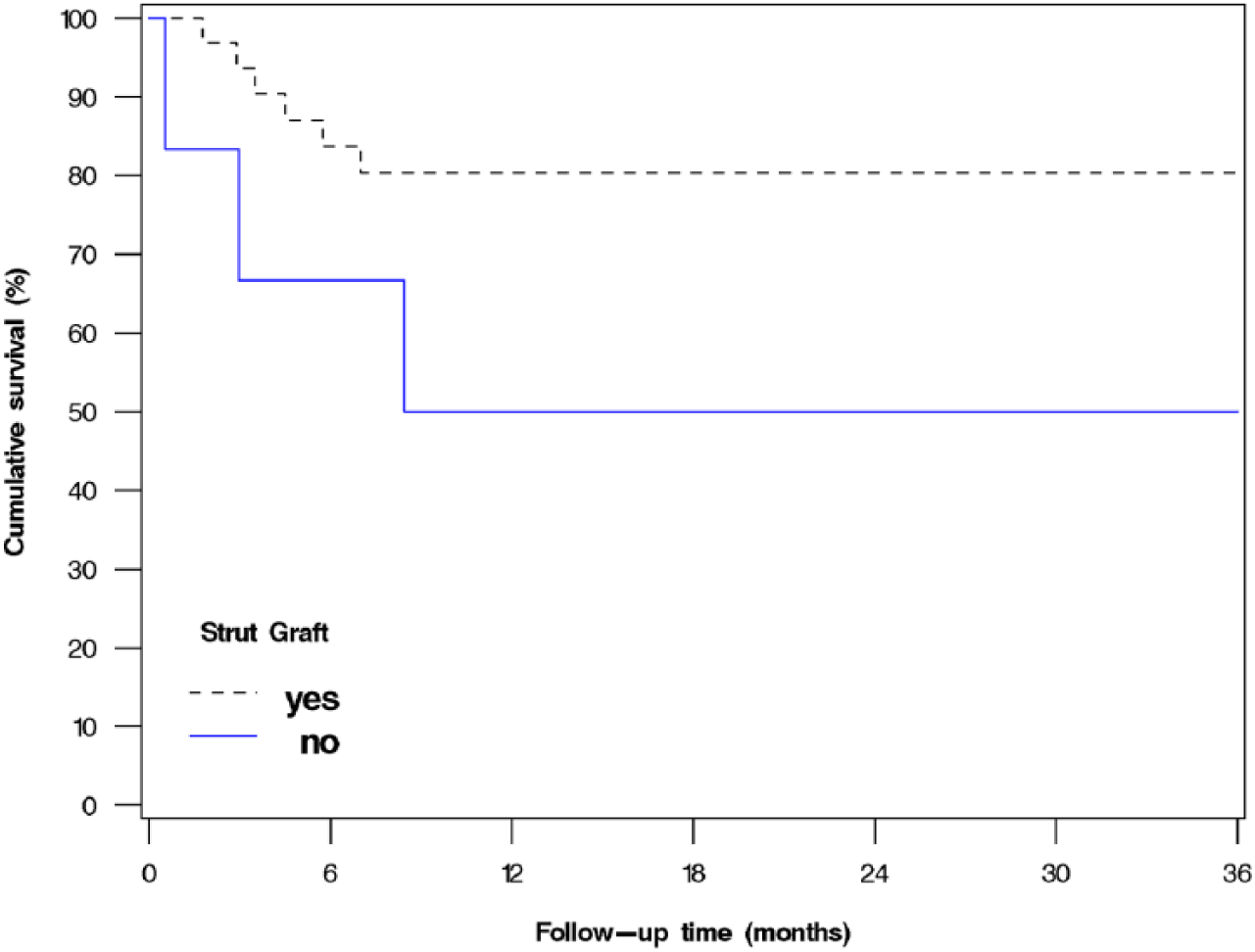
Cumulative survival of plating with or without strut grafts with re-operation for any reason as the endpoint (n = 39, p = 0.108, HR = 3.12, 95% CI: (0.78, 12.50)).
There were 16 cases of post-operative surgical site complications: seven infections (four in the plating group and three in the re-arthroplasty group), six cases of non-union in the plating group and three cases of recurrent patellar dislocation in the re-arthroplasty group.
Infections in the plating group were treated by lavation and debridement in three cases with combined change of the plastic part in two cases. One patient was treated only with antibiotics. All of these patients healed well, and one of them was able to walk without aid, and two with the help of a walker device. Of the three infection cases in the re-arthroplasty group, one was treated by lavation and debridement, one by re-arthroplasty, and one patient with a necrotic wound infection by reconstruction with a gastrocnemius graft. This last patient later developed a fistula and underwent another re-operation but eventually the limb had to be amputated above the knee.
Non-union was reported only in the plating group. Of the six non-union cases, two were treated by re-arthroplasty and three were treated by re-laminofixation (of which two later also underwent re-arthroplasty). One patient was immobile due to a neurological condition and was not treated operatively.
Three patients developed recurrent patellar dislocation after re-arthroplasty. Two of these patients were treated by changing the plastic part of the prosthesis and performing a soft-tissue re-alignment procedure of the patella. Afterward, the knee was stable in both cases. One patient was treated by re-arthroplasty with a Link endomodel hinged prosthesis and a soft-tissue re-alignment procedure of patella.
There was at least one re-operation after the index procedure in 18 patients (26.5%). Three of these patients were not re-operated due to one of the complications mentioned above. An 86-year-old man treated by re-arthroplasty showed an iatrogenic diaphyseal fracture in the post-operative radiograph close to the proximal edge of the stem of the femoral component. This was treated the following day by laminofixation and strut graft. An 86-year-old female patient treated by plating fell in the ward during recovery and had a new fracture above the plate. She healed well after re-laminofixation and was able to walk with the aid of a walking stick. A 76-year-old woman with a history of Parkinson’s disease healed well after re-arthroplasty, but was wheelchair-bound because of her disease and problems with her other knee. Almost 5 years after the operation, she had a new periprosthetic fracture above the stem of the femoral component after falling out of her wheelchair. She was then treated by laminofixation.
Clinical outcome was not assessable in nine patients. Four of these patients did not have a follow-up visit at our unit. In all of these cases, fixation was reported stabile and post-operative radiographs were good. One patient, as mentioned before, fell in the ward and suffered a new diaphyseal fracture right after the index procedure. Another patient fell and had a diaphyseal fracture of the tibia 2 months after re-arthroplasty. Three patients died before a follow-up appointment. One of these, a 73-year-old female patient with a history of Alzheimer’s disease represented hemiparesis symptoms after surgery and died shortly after. Two other female patients (84 and 94 years of age) were in poor medical condition both pre- and post-operatively and died a few days after surgery.
Discussion
We found out that post-operative surgical site complications were relatively common after the treatment of periprosthetic supracondylar femoral fractures. The survival rates after re-arthroplasty and laminofixation were similar. However, the survival of laminofixated fractures with strut grafts was higher than that without strut grafts. In half of the patients, the clinical outcome was comparable to pre-fracture status.
Herrera et al. reviewed systematically 29 studies of periprosthetic supracondylar femoral fractures. The mean age of the patients was 69 years. The mean age of the patients in our study was 79 years, so the results are not directly comparable. The previously reported results show an overall non-union rate of 9%, a fixation failure rate of 4%, an infection rate of 3%, and a revision surgery rate of 13% (3). In our study, the non-union rate of the plating group was 15%, but this figure included fixation failures. We consider the combined non-union and fixation failure rate in our study comparable to that of previous studies. In a study of Hoffmann et al., the non-union rate was 22%. This study pointed out the increasing age of patients from a mean of 67 years in 1986 to 73 years in 2006 and up to 78 years in 2010 (11). The mean age of 79 years of our patients, and high co-morbidity rate conform to these findings.
A mean non-union rate of 5.3% has been reported for osteosyntheses using locking plates, which is lower than that for osteosyntheses using conventional plates only (3). Our series with a study period from 2000 to 2010 included both conventional and locking plates. The amount of these relatively rare fractures in the current study is small, and we did not find it necessary to perform subgroup analyses separately for conventional and locking plates. Locking plates have for several years been in routine use for the treatment of Rorabeck type I and II fractures at our institution.
In the current study, fracture union was determined by medical records of the follow-up appointments. As we mention in the “Materials and methods” section, any cases of radiological non-union, plate failure, or continuing pain leading to re-fixation were classified as non-union. Thus, a pain-free result with an intact plate and satisfactory ossification indicated by either callus-formation or disappearing of the fracture line was classified as union of the fracture.
In our experience, radiological fracture union can in some cases be difficult to evaluate, especially in very distal or complex fractures and in cases of partial union. When this is the case, clinical outcome and pain-levels give some information of the state of the fracture. In some cases where radiological union had already been declared, this was later proven wrong when increasing pain eventually led to the failure of the plate. Due to these issues a precise time to union was not measurable for many of the study patients and we cannot thus provide a mean union time.
The infection rate of 10% in our study is higher than published previously. This may be linked to the slower healing rate and surgical complications associated with very elderly patients. The mean age of the patients in the current study is 10 years higher than that of similar publications from previous decades. Another possible explanation is in infection classification, which is an area that seems quite heterogeneous. We considered only clinically diagnosed surgical site infections requiring some form of intervention an infection complication. We point out that other studies have even considered, for instance, a post-operative urinary tract infection an infection complication (12). The systematic review by Herrera et al. reported an overall infection rate of 3%, but the review only took into account deep infections resulting in surgical debridement. Infections leading to non-union were counted as non-union (3). These both may underestimate infection rates.
The revision surgery rates for the laminofixation group and the re-arthroplasty group in our study were 23% and 31%, respectively, which are higher than those in previous studies overall. The older age of our patients along with probably more osteoporotic bone and poorer medical condition may in part explain this difference.
The reasoning behind selection of treatment method or possible bone grafting could not be provided in our study. This selection is based on several individual features of the patient, the fracture pattern and the clinical instinct of the surgeon. These variables are not classifiable in any feasible way. The treatment method cannot be dictated by fracture typing only, which is especially clear in the case of very distal fractures. The advantages of faster mobilization after re-arthroplasty are also indisputable when compared to internal fixation techniques. Prolonged immobilization of an elderly patient puts future walking capability at risk, not to mention the other known complications associated with immobilization.
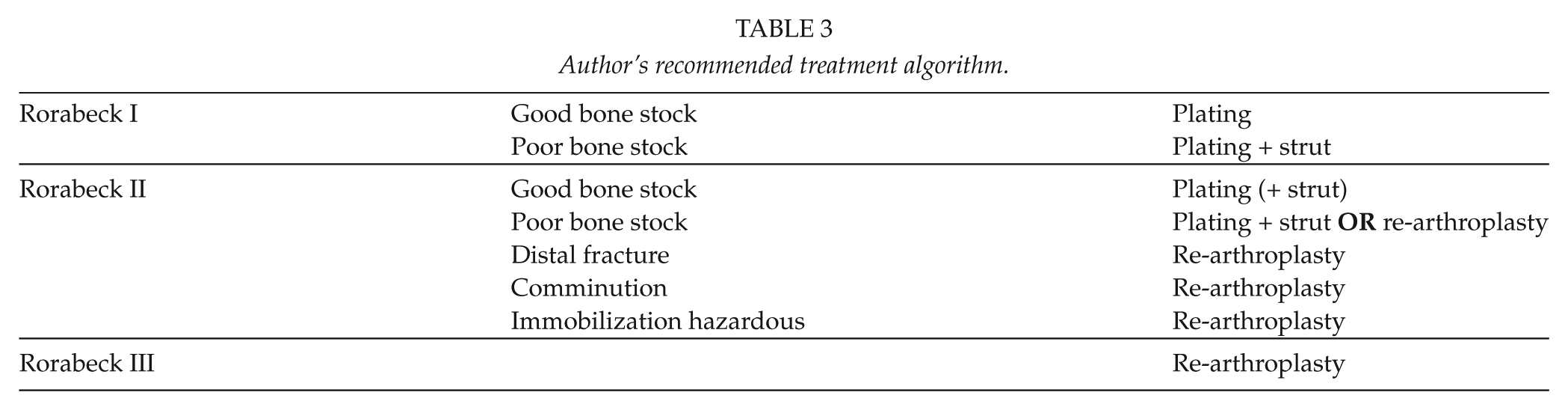
It has been suggested that in very distal PSFs, the bone stock of the distal femur is not always adequate for internal fixation (13). Although internal fixation by plating with possible bone grafting is an alternative for treatment in these cases, our routine has been to consider revision TKA in very distal fractures and in cases of poor bone quality or comminution (9). If the fracture line is on the level of the anterior proximal part of the femoral component, there is seldom enough bone in the distal femoral fracture fragment to enable laminofixation. This is the most common reason to choose revision instead of laminofixation in Rorabeck II fractures. Complex comminution of the femoral bone is not that common in these low-energy fractures. A recently published study compared the use of revision TKA at the time of fracture to revision TKA after failed open reduction and internal fixation. The results showed fewer future operations in the group treated by revision TKA at the time of fracture. Revision TKA was recommended for osteopenic patients or those with greater non-union risk (14). See Table 3 for the author’s recommended treatment algorithm.
Author’s recommended treatment algorithm.
There are only a few studies focusing on the use of re-arthroplasty in the treatment of periprosthetic distal femoral fractures. Cases of re-arthroplasty have often been excluded from studies that concentrate on internal fixation. Mortazavi et al. (12) reported of 20 patients treated by re-arthroplasty with a hinged prosthesis. There were 10 post-operative complications, and five of the patients required additional surgery. The high complication rate was asserted with the high age and medical co-morbidities of the patients. The 31% re-operation rate in our study is comparable to that reported by Mortazavi et al. Although patellar dislocation is a devastating complication after re-arthroplasty, the most common and feared complication is infection. Re-arthroplasty is often considered a more invasive procedure with larger exposure and longer operative time compared to internal fixation techniques. In our study, we found no difference in infection rates between the treatment groups even though operation duration was, indeed, longer.
The success of the use of strut grafts in association with plating in the treatment of periprosthetic distal femoral fractures is interesting. Strut grafts have been seen as an option in fractures associated with poor bone quality (9). Haddad et al. suggested that cortical onlay strut allografts act as biological bone plates and serve both a mechanical and a biological function. The authors reported a higher rate of fracture union, satisfactory alignment, and an increase in proximal and diaphyseal femoral bone stock (15). Our results of using strut grafts successfully in distal periprosthetic fractures give support to earlier findings of using strut grafts in proximal femoral fractures. The use of onlay strut grafts in the treatment of periprosthetic distal femoral fractures has, to our knowledge, not been reported earlier.
Our study has limitations. It is retrospective, focusing on different treatment options for a diverse range of fracture patterns, and the number of cases is limited. Furthermore, the reasoning behind the selection of the method of treatment cannot be provided. Radiological evaluation or functional knee scores are not available because of the study design that did not make it possible to arrange systematic outpatient visits to evaluate them.
However, our results may well represent standard outcome in a Northern European clinic. It is in these kinds of clinics, or smaller, where most of these fractures are treated. In general, during the study period, the Turku University Hospital may have been considered as a non-specialized clinic compared to specialized high volume orthopedic units like Mayo Clinic in Rochester, Minnesota (who also publish a lot of papers). In Finland, these fractures are treated mainly in university clinics and in the largest central hospitals. In the Hospital District of Southwest Finland, these fractures are nowadays centralized to Turku University Hospital. For example, the supracondylar femoral fractures of the Satakunta Central Hospital region are sent to us. In the Finnish scale, the experience of treatment of these fractures in our clinic is nowadays high. With this article, we want to underline the importance of these fractures: their increasing incidence and that they are often very difficult to treat. The total number of published European PSFs is only several hundreds. If only well-arranged studies from high volume centers are published, the complication and revision surgery rates may be misrepresented. The purpose of our study was not to provide recommendations or new guidelines for treatment but to describe and assess treatment outcome in a typical Northern European clinic.
These patients are generally very old, have multiple co-morbidities, and many of them die shortly after such a devastating trauma. Interestingly, knowing the fact that major surgery is a great risk for extended hospitalization for these patients, we noted that almost three quarters of our patients were eventually able to return to their preceding state of living. Our results show that operative treatment, whether plating or re-arthroplasty, generally delivers satisfactory results regardless of the reported complications.
Footnotes
Acknowledgements
The authors thank M. Seppänen, J. Mokka, M. Junnila, and T. Vahlberg.
Declaration of Conflicting Interests
None.
Funding
This study was supported by the Orion-Farmos Research Foundation and Turku University Research Grant (EVO).