
Abstract
Aims:
To assess outcome in patients with locally advanced rectal cancer undergoing multivisceral resection.
Methods:
Retrospective study of 30 consecutive patients (mean age 67.8 years) with primary locally advanced rectal cancer undergoing en bloc multivisceral resection of the organs involved with curative intent between 1998 and 2010. Overall survival, local and distal recurrence, and disease-free survival were analyzed by the Kaplan–Meier method. Risk factors for clinical outcome were obtained using a Cox multivariate model.
Results:
Postoperative complications occurred in 76.7% of patients and the in-hospital mortality rate was 10%. The median follow-up was 28.8 months. A total of 19 patients died at follow-up. Of the 11 patients who were alive, 7 were free of disease. In the multivariate analysis, lymph node involvement, stage II, and lymph vascular invasion were significantly associated with survival, and stage III showed a strong trend towards significance. Suture dehiscence (peritonitis and intra-abdominal abscess) showed a significant trend towards a higher local recurrence. Lymph vascular invasion was associated with a higher distant recurrence.
Conclusion:
Lymph node involvement was associated with worse survival, whereas stage II and absence of lymph vascular invasion were associated with a better survival. Lymph vascular invasion was associated with a higher distant recurrence.
Keywords
Introduction
The incidence of locally advanced rectal carcinoma ranges between 5% and 20% (1–6). Total mesorectal excision and the protocolized use of neoadjuvant and adjuvant radiation therapy and chemotherapy (4, 6) have been essential to reduce the local recurrence rate and to increase survival in patients with locally advanced rectal tumors. Recent guidelines of the National Cancer Institute (7) and the American Society of Colon and Rectal Surgeon (8) emphasize that appropriate surgical management of these locally advanced colorectal cancers should include multivisceral resection, in which the cancer and adherent structures are removed en bloc. These clinical guidelines are based on studies showing that 40%–84% of adhesions to neighboring structures are due to tumor invasion, with the remaining adhesions being inflammatory in nature. However, neither preoperative nor intraoperative assessments are adequate to distinguish between these two types of adhesions. Despite these recommendations, the majority of patients did not receive a multivisceral resection, probably in relation to surgeon- and/or patient-related factors (3).
Different studies have reported the results of multivisceral resection for locally advanced colorectal cancer (3, 5, 7, 9–12), but few clinical studies have focused solely on locally advanced rectal cancer, possibly because of the lower number of cases and the difficulty of recruiting large case series (1, 2, 4, 6, 8, 13, 14). Therefore, this study was undertaken to analyze the outcome of multivisceral resection in patients exclusively affected by primary rectal carcinoma infiltrating adjacent structures and to identify predictors of recurrence and survival.
Method
We conducted a retrospective review of all consecutive patients with primary locally advanced rectal cancer infiltrating adjacent organs undergoing multivisceral resection at the Colorectal Surgery Unit of the Department of Surgery of Hospital Universitari Vall d’Hebron in Barcelona, Spain, between November 1998 and September 2010. Inclusion criteria were as follows: histological confirmation of adenocarcinoma, tumor location within 15 cm from the anal verge, and potentially curative en bloc resection of the tumor and involving structures. Exclusion criteria were multivisceral resection for local recurrence and/or preoperative detection of metastasis. All patients were operated on via the open method.
The medical history and pathology reports were reviewed by two of the authors (M.J.M. and E.E.). For each patient, the following data were included in the database: demographics; family history of cancer; clinical presentation; laboratory data (hematocrit, leukocyte count, liver function tests, carcinoembryonic antigen (CEA) and cancer antigen (CA) 19.9); diagnostic studies (colonoscopy/rectoscopy, virtual colonoscopy); locoregional assessment (magnetic resonance imaging (MRI), transrectal endoscopic ultrasound) and extension study (abdominal computed tomography (CT), abdominal ultrasound); American Society of Anesthesiologists Physical Status (ASA) classification; surgical procedure and perioperative data (intraoperative findings, need of intraoperative or postoperative blood transfusion, intraoperative complications); histopathological data, including the histologic type, radicality of the surgical procedure (R0: no residual tumor, R1: microscopic residual tumor ≤ 1 mm, R2: macroscopic residual tumor); number of lymph nodes excised, number of lymph nodes affected and grade (G1: well differentiated, G2: moderately differentiated, G3: poorly differentiated); neoadjuvant and adjuvant treatment; postoperative morbidity (major complications were defined as those that required prolonged hospital stay (>2 weeks) and/or that required surgical reintervention, other complications were defined as minor (15)); anastomotic dehiscence defined as peritonitis secondary to anastomotic failure; hospital mortality (death within 30 days after surgery); survival; and locoregional and systemic recurrence. Tumors were classified by the American Joint Committee on Cancer and International Union against Cancer stage classification.
Oncological treatment was indicated by the oncologist in charge. Details of oncological treatment were recorded, differentiating neoadjuvant (chemotherapy and/or radiation therapy) treatment from adjuvant treatment. Radiation therapy usually included mean total doses of 50 Gy, although some patients received short cycles as neoadjuvant therapy. Chemotherapy regimens usually included 5-fluorouracil, leucovorin, oxaliplatin, and irinotecan. In most patients, oncological treatment was indicated by the Committee of Colorectal Cancer of our hospital according to radiological criteria (suspicion of involvement of the mesorectal fascia, lymph node involvement, or invasion of adjacent structures) for neoadjuvant treatment and histopathological criteria (R1 resections, stages III and IV, and high-risk stage II tumors (perforation, venous/lymphatic invasion, mucinous component >50%)) for adjuvant treatment.
Date of operation was defined as the start of follow-up. Survival was calculated to date of death attributable to the disease or for any cause or to date at the end of follow-up period (September 2010). Local recurrence was defined as the presence of histologically or radiologically proven tumor in the original tumor bed or surrounding structures. Distant recurrence was defined as the presence of histologically or radiologically proven tumor in the parenchyma of any organ and peritoneal carcinomatosis. Disease-free survival was defined as the period between the date of operation and the date at which progression of disease was documented.
Statistical Analysis
Continuous variables are expressed as mean and standard deviation (SD) and categorical variables as frequencies and percentages. The chi-square (χ2) test was used for the comparison of categorical variables. Overall survival and disease-free survival were analyzed with the Kaplan–Meier method. Differences were assessed with the log-rank test. Variables related to survival were analyzed using a Cox multivariate model in which only statistically significant variables in the log-rank test were considered. Statistical significance was set at p < 0.05.
Results
During the study period, a total of 741 patients with rectal cancer were operated on, 30 (4%) of which received multivisceral resection for locally advanced primary rectal cancer. There were 12 men and 18 women with a mean (SD) age of 67.8 (12.6) years. The follow-up was complete in 100% of patients, with a median of 28.8 months. Clinical and diagnostic data are shown in Table 1. The most frequent clinical findings were positive digital rectal examination (66.7%), rectal bleeding (60%), weight loss, asthenia and anorexia (53.3%), and change of bowel habits (50%). Fiberoptic colonoscopy and abdominopelvic CT were the most common diagnostic procedures (CT showed a sensitivity of 80% in the diagnosis of locally advanced tumors).
Clinical and diagnostic features of 30 patients with locally advanced primary rectal cancer undergoing multivisceral resection.
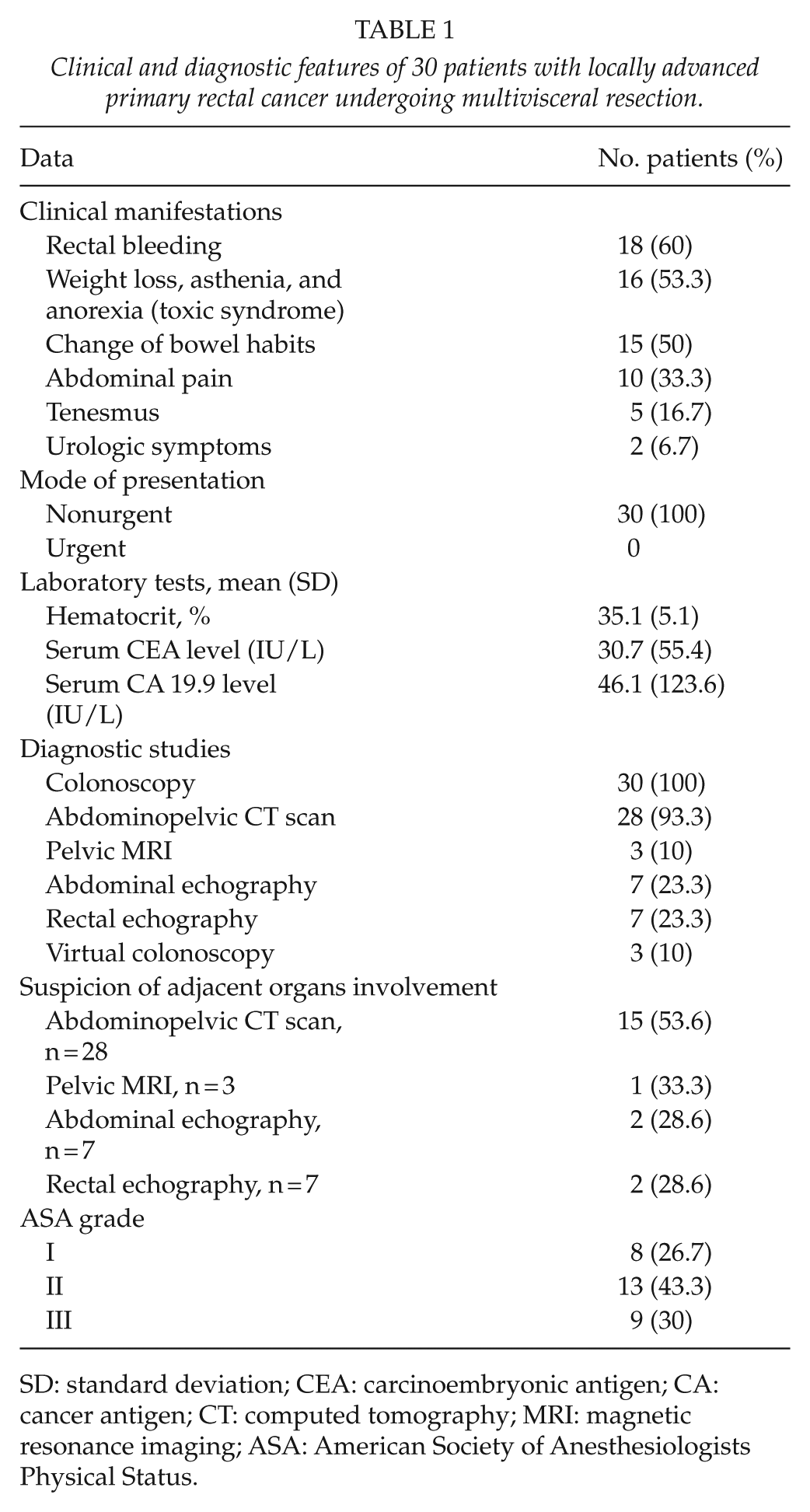
SD: standard deviation; CEA: carcinoembryonic antigen; CA: cancer antigen; CT: computed tomography; MRI: magnetic resonance imaging; ASA: American Society of Anesthesiologists Physical Status.
A total of 10 patients received neoadjuvant radiochemotherapy and 6 patients received radiation therapy only. In the remaining 14 patients, neoadjuvant radiation therapy was not administered because of history of radiotherapy for another malignancy or morbidity-associated contraindications. Postoperative adjuvant treatment was indicated in 15 patients (50%), 5 of which have been treated with neoadjuvant radiochemotherapy and 4 neoadjuvant radiotherapy. Two patients (6.7%) received adjuvant chemotherapy and radiation therapy without any previous treatment.
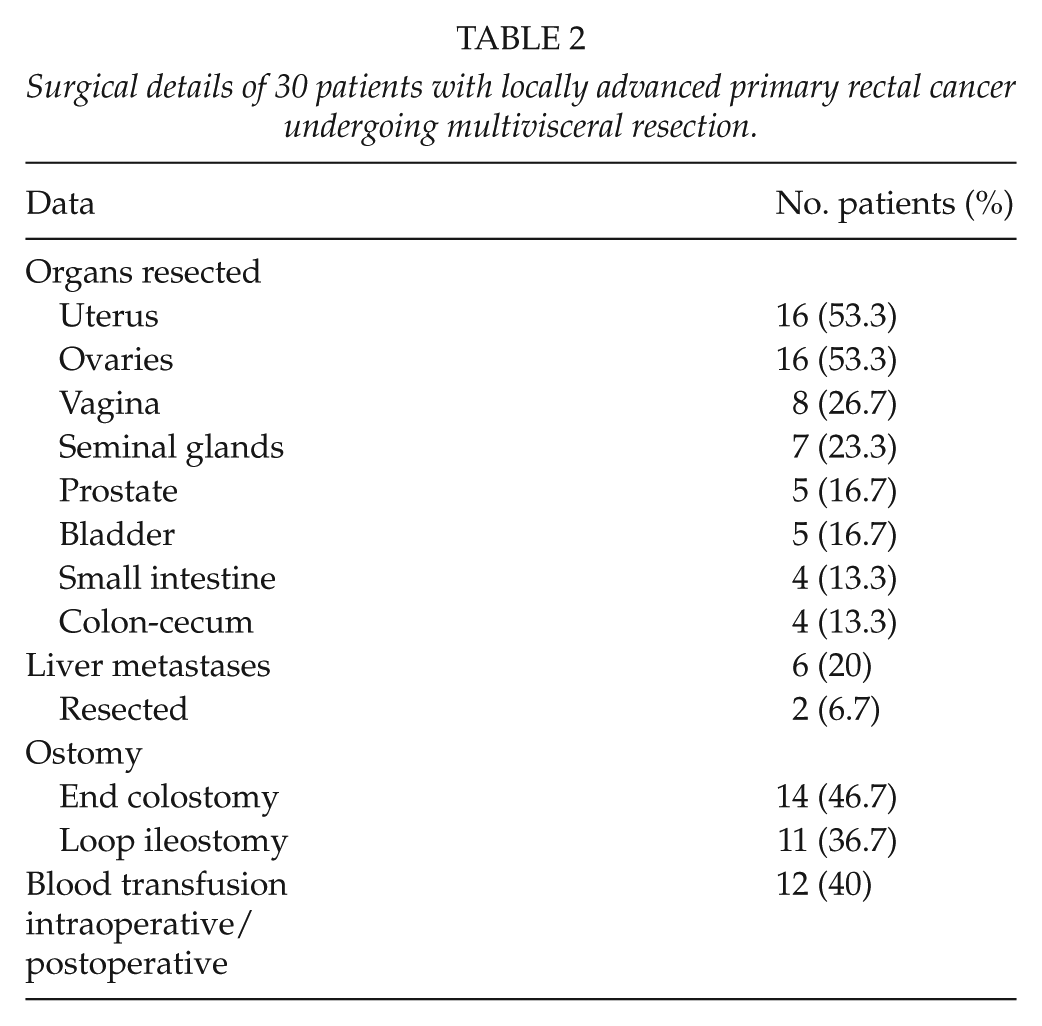
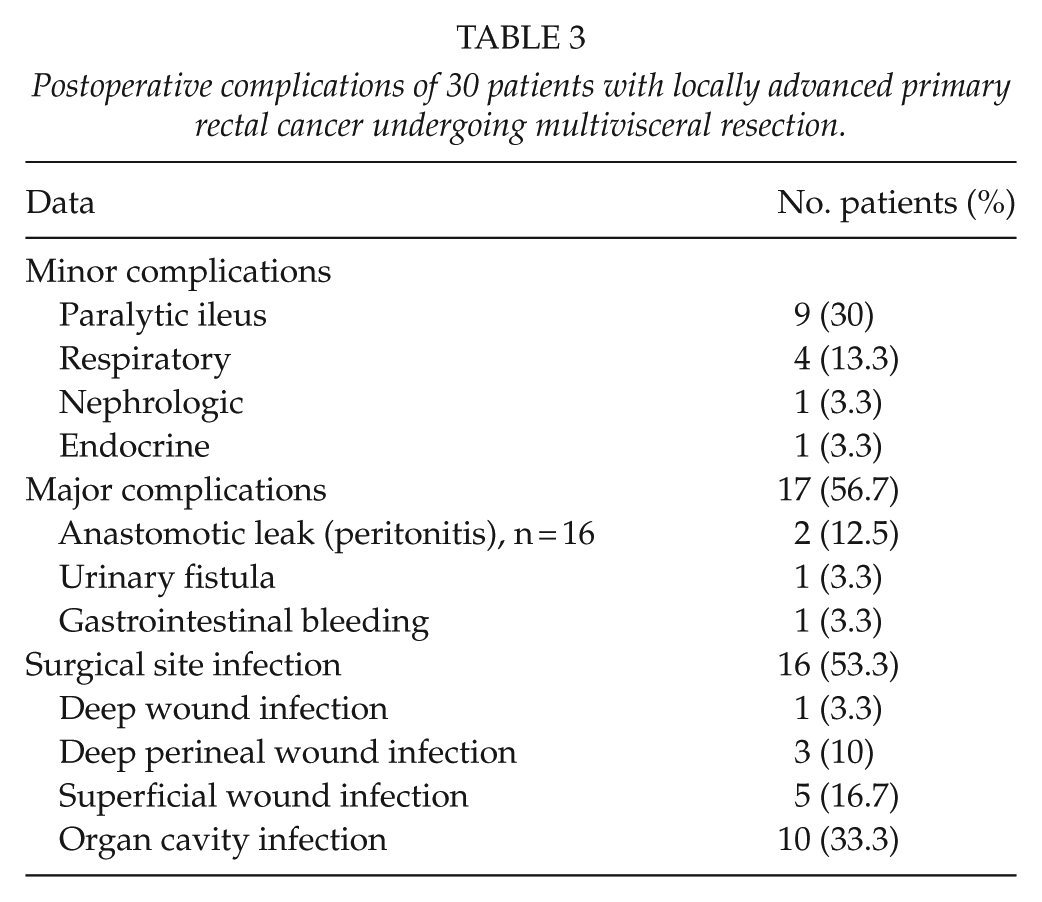
The organs most frequently resected en bloc with the primary rectal tumor were the uterus and the ovaries followed by the prostate and the bladder. End colostomy was performed in 14 cases, and loop ileostomy in 11. Liver metastases were found in 6 patients (20%), with a synchronous resection of the hepatic mass in 2 cases. Intraoperatively, surgical resection was classified as curative resection (R0) in 30 patients (100%) and histopathologic examination showed tumor infiltration of the margins (R1) in 8 patients. Of these, 12 patients (40%) required intraoperative blood transfusion. Postoperative complications occurred in 23 patients (76.7%), with major complications in 17. The hospital mortality was 10% (n = 3). Causes of death were respiratory failure in two patients and septic shock secondary to intra-abdominal abscess in one. Details of the surgical procedure and perioperative data are shown in Tables 2 and 3.
Surgical details of 30 patients with locally advanced primary rectal cancer undergoing multivisceral resection.
Postoperative complications of 30 patients with locally advanced primary rectal cancer undergoing multivisceral resection.
The histopathological diagnosis was conventional adenocarcinoma in 24 patients (80%). R0 resection was achieved in 22 patients (73.3%). The tumor spread to adjacent organs in 20 patients (66.7%); it was staged as pT4b. The most frequent tumor-node-metastasis (TNM) stage was III (11 patients, 36.7%). Histopathological features and stage are shown in Table 4.
Histopathological features and stage in 30 patients with locally advanced rectal cancer undergoing multivisceral resection.
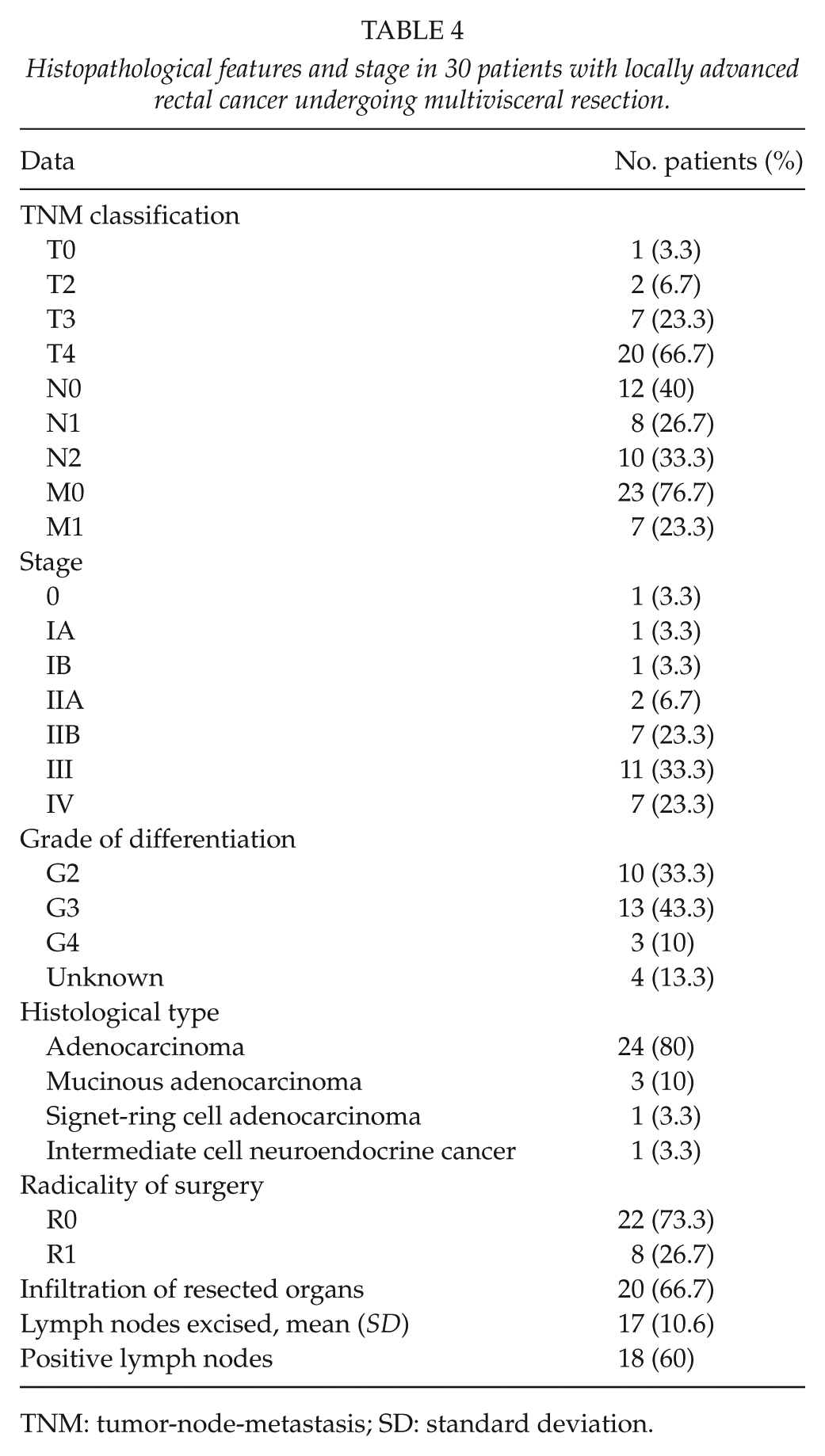
TNM: tumor-node-metastasis; SD: standard deviation.
At the end of follow-up, 11 patients (36.7%) were alive. As shown in Fig. 1, of the 11 patients who were alive, 7 were free of disease and 4 had recurrence of rectal cancer (local recurrence 2, distant recurrence 2). In the subgroup of 20 patients with pT4b disease, 12 patients died (mortality rate 60%), and of the 8 survivors, local recurrence was documented in 2 and distant recurrence in 2 (Fig. 2). Of the 19 patients (63.3%) who died, cancer was the cause of death in 12 (63.1%) patients, 10 patients (83.3%) had pT4b in the histological study and 4 (30%) were found to be stage IV at surgery. After excluding patients who died in the postoperative period and patients with unresectable intraoperative metastasis, local recurrence was documented in 37% (10/27) patients and distant recurrence in 34.8% (8/23). The outcome of patients at follow-up is shown in Figs 1 and 2.
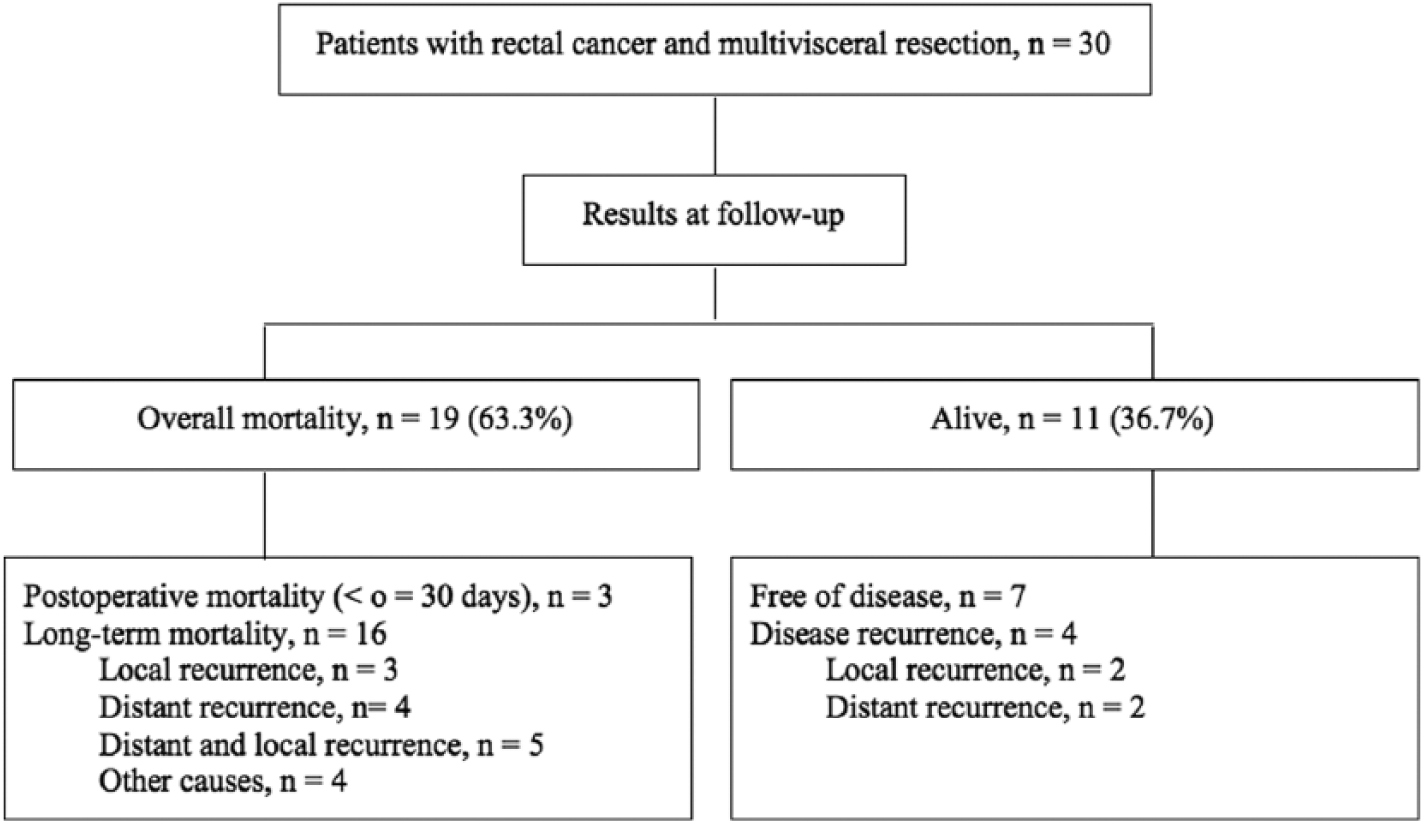
Follow-up results in 30 patients with locally advanced rectal cancer treated with multivisceral resection.
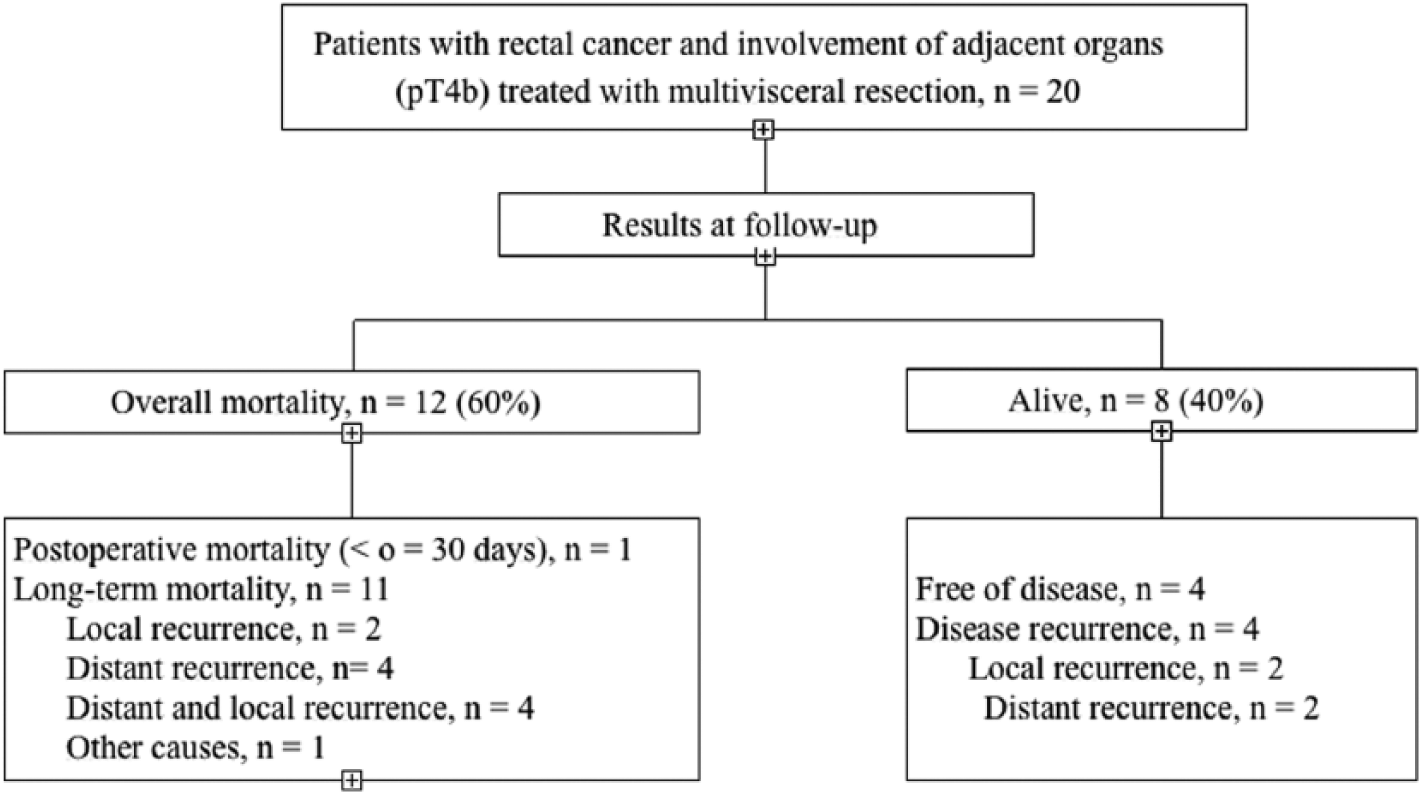
Follow-up results in 20 patients with locally advanced rectal cancer pT4 treated with multivisceral resection.
In the univariate analysis, age, endoscopic distance to the anal verge, CEA level, number of positive lymph nodes, and stages III and IV were significantly associated with a lower probability of survival, whereas pelvic exenteration, bladder resection, prostatectomy, absence of venous and lymph node invasion, and stage II were significantly associated with a higher probability of survival. Peritonitis and wound dehiscence showed a trend towards significance (p = 0.055) in the univariate analysis. In the multivariate analysis, nodal involvement was independent predictor of poor survival, whereas stage II and absence of lymphatic vascular invasion were significantly associated with a better outcome. Stage III had a significant trend as a predictor of poor survival with p = 0.050 (Table 5). As shown in Fig. 3, lymph node involvement was significantly associated with worse survival.
Result of multivariate analysis. Prognostic factors associated with survival in 30 patients with locally advanced rectal cancer undergoing multivisceral resection.
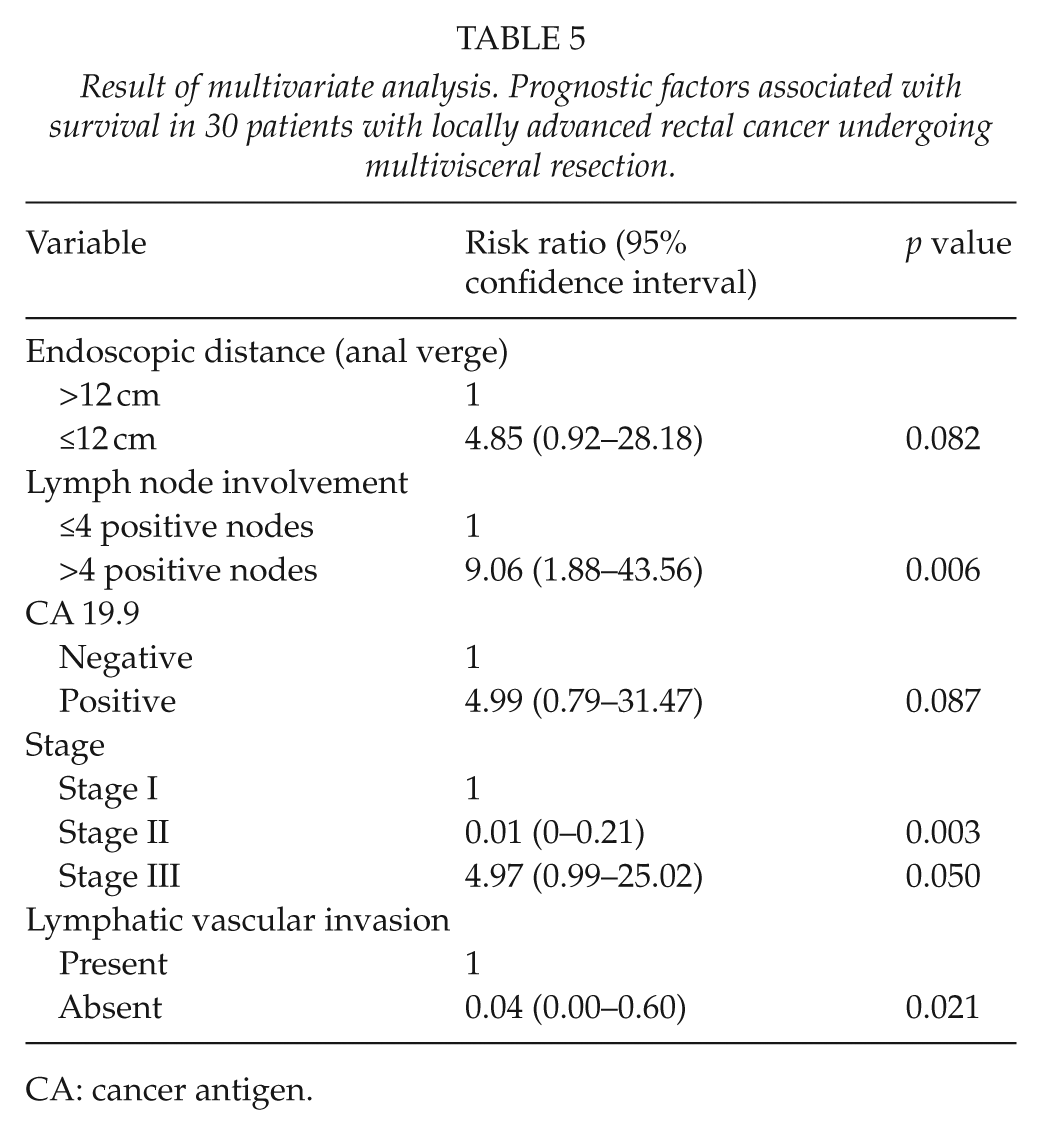
CA: cancer antigen.
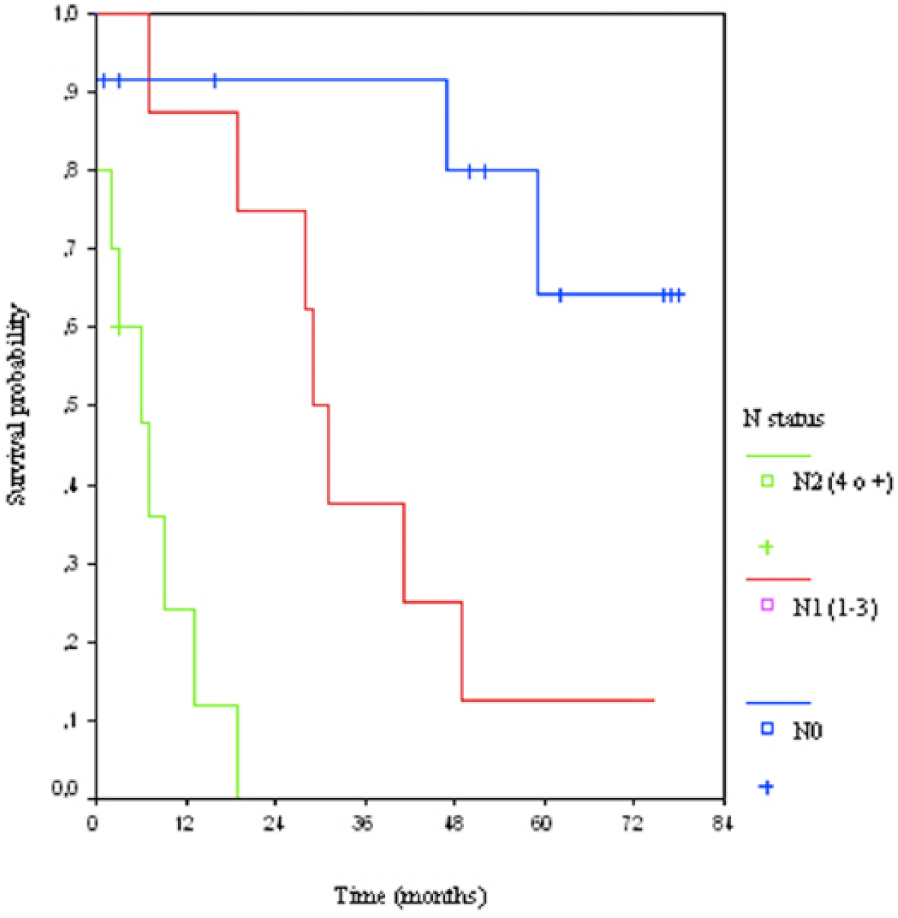
Actuarial curve for survival depending nodal involvement.
The mean disease-free survival until local recurrence was 23.3 (6.1) months, and the mean disease-free survival until distant recurrence was 16.0 (12.8) months. No statistically significant variables associated with the probability of disease-free interval either until local relapse or distant recurrence were found in the multivariate analysis, although there was a relationship between lymphatic vascular invasion and distant recurrence in the Kaplan–Meier analysis, with a log-rank of 4,126 and p = 0.042. Differences between R0 and R1 resection groups in the overall survival (closed to 5 years vs close to 3 years) (log-rank = 0.519, p = 0.471) and disease-free survival (78 months vs 62 months) (log-rank = 0.398, p = 0.533) were not observed.
Discussion
Multivisceral resection in patients with locally advanced rectal cancer is a complex surgical procedure associated with an increase in morbidity (1, 9, 11, 13). Clinical guidelines and results of different studies published in the literature indicate that when complete excision is feasible, the surgical approach in these patients is multivisceral because despite a higher morbidity, it has been shown to increase long-term survival (1–4, 7, 8).
The incidence of multivisceral resection for locally advanced rectal cancer of 4.1% (30 patients) in our series is similar to that reported by others (1–6). Histopathologically, adhesions to surrounding structures were due to tumor invasion in 66.7% of the cases. As the nature of adhesions cannot be established intraoperatively, en bloc resection of affected adjacent organs is the only way of obtaining R0 resections. None of the clinical, laboratory, or imaging data were significantly associated with survival. However, CT scan showed 80% sensitivity to detect locally advanced tumors and was the most frequent study performed in our patients (93.3%). Pelvic MRI, which is currently the technique of choice for the local assessment of rectal cancer, was included in the diagnostic protocol of rectal tumors in recent years; this is the reason why the rate is low in this historical series.
Operative morbidity and mortality after en bloc multivisceral resection for locally advanced rectal cancer varies between 21% and 61% and between 3% and 10%, respectively, which is higher than after standard resection (10, 16, 17). The overall morbidity rate was 76.7%, with a percentage of major complications of 56.7% and surgical site-related complications of 53.3%. The hospital mortality rate of 10% is within the ranges reported in other studies. The incidence of anastomotic dehiscence after low anterior resection for rectal cancer ranges between 1% and 13% (18, 19) and in our series occurred in only two patients (12.5%). None of these factors was associated with a lower survival.
A multidisciplinary approach with neoadjuvant radiochemotherapy together with multivisceral resection (3, 8) has demonstrated to increase survival with an acceptable mortality. The effect of neoadjuvant chemotherapy and radiation therapy (QT-RT) on perioperative and postoperative morbidity is unclear. In different studies, neoadjuvant QT-RT does not appear to increase postoperative morbidity (20). In the experience of Valenti et al. (21), postoperative complications are associated with the preoperative clinical status of the patient and duration of surgery but not with neoadjuvant treatment. Kerr et al. (22) concluded that to postpone surgery 8 weeks after neoadjuvant reduces morbidity without compromising prognostic factors. These authors also showed that reduction of postoperative inflammatory response associated with neoadjuvant QT-RT appears to be related to an increase in the susceptibility of local complications (23). In the study of the German Rectal Cancer Group (24), toxicity gastrointestinal indexes were similar between patients undergoing neoadjuvant treatment and patients undergoing adjuvant therapy (28.8% vs 31.7%). Sacral or pelvic fractures are late complications in patients treated with radiotherapy of the pelvis. Late toxicity in relation to neoadjuvant therapy, such as changes in the bowel habits, urinary alterations, fecal incontinence, or actinic rectitis, has been reported (16). In our study, a direct relationship between neoadjuvant QT-RT and postoperative complications was not found.
Five-year survival after a curative resection (R0) varies from 35% to 71% (1–4, 6, 14). The overall survival in our series was 36.7%, but considering the 12 patients with R0 resection in the subset of 20 patients staged a pT4b, the survival at the end of follow-up was 41.7% (5/12), which is consistent with data reported in the literature, although the percentage of patients with lymph node involvement (60%) in our study was higher than that documented in many of the aforementioned studies (2–4, 6, 9, 10, 14, 25). Lymph node involvement has been one of the factors more frequently related to poorer survival in several studies (1, 2, 4, 6). In our study, in the multivariate analysis, lymph node involvement was significantly associated with a worse survival (as shown in Fig. 3), whereas absence of lymphatic vascular invasion and stage II were predictor of a favorable outcome. Stage III showed a strong trend towards significance in the survival study.
Local recurrence is an important variable in the follow-up of rectal cancer patients after surgical treatment. The percentages of local relapse range between 3% and 35% (26, 27). Total mesorectal excision and neoadjuvant treatment decreased local recurrence (28). In the study of Harris et al. (2), local recurrence was predicted by metastatic disease and nodal disease. In the experience of Larsen et al. (6), N-stage, CEA response, and pelvic wall resection were relevant factors for local recurrence. Moreover, despite a better control of locoregional recurrence, patients with locally advanced rectal cancer showed a higher incidence of distant metastases (up to 50%–60% of the cases) (4, 14). In a systematic review and meta-analysis (29), anastomotic leakage had a negative prognostic impact on local recurrence after restorative resection of rectal cancer, although no association between anastomotic leakage and distant recurrence was found. However, the relationship between anastomotic failure and outcome is controversial (30). Our results regarding local recurrence (37%) and distant recurrence (34.8%) are similar to those reported in the literature. Lymphatic vascular invasion showed a significant association with distant relapse. In the multivariate analysis, no significant factors were associated with local or distant recurrence, although wound dehiscence and peritonitis showed a trend towards significance as risk factors for local recurrence, probably due to the small sample population.
In summary, in this study, multivisceral resection showed a perioperative mortality of 10%, a high morbidity (76.7%), and a long-term survival of 36.7%, which in our opinion justify the risks of multivisceral resection in patients with locally advanced rectal cancer. Factors associated with a better survival were stage II and absence of vascular invasion, whereas lymph node involvement was associated with a poor survival. Lymph vascular invasion was associated with a higher distant recurrence. However, the high complication rate of multivisceral resection for locally advanced rectal cancer supports the need of centralizing this kind of surgery to high volume centers.
Footnotes
Acknowledgements
The authors thank Marta Pulido, MD, for editing the manuscript and for editorial assistance.
Declaration of Conflicting Interests
M.J. Mañas and other co-authors have no conflict of interest.
Funding
M.J. Mañas and other co-authors have no financial support.