
Abstract
Background and Aims:
Electrical burns are uncommon, but they result in high morbidity and mortality due to severe tissue damage. The purpose of this study is to analyze epidemiological variables of electrical injuries and identify preventable measures through them.
Material and Methods:
We retrospectively analyzed the clinical records of 625 patients admitted to Hangang Sacred Heart Hospital’s Department of Plastic Surgery from January 2005 to December 2011. We divided the patients into two groups: (1) low-voltage injury (under 1000 V) and (2) high-voltage injury (over 1000 V). We reviewed the following variables: age, sex, total burn surface area, injury type and mode, and surgical modalities.
Results and Conclusions:
The mean age of all patients was 33.4 ± 18.2 years. The ratio of males to females was 13.5 in the whole group. The mean total body surface are burned was 14.0% ± 13.8% in total. The majority of electrical burns in the low-tension group and high-tension group occurred in patients under 20 years and in patients aged 40–59 years, respectively. Steel chopstick insertions and high-voltage electrical work/repair were the most common injury modes in the low-tension group and the high-tension group, respectively. Groin and abdominal distant flap surgeries were commonly performed in both groups. It is recommended that these risks be prevented through education and safety measures to reduce the incidence of electrical injuries.
Introduction
Electrical burns are uncommon, but they are often the most devastating of all thermal injuries, usually causing damage of both the skin and deeper structures, which can lead to large areas of necrosis, resulting in increased morbidity and mortality. Electrical injuries have the potential to contain three different components: true electrical injury caused by current flow, arc injury at a flexor part of the human body (e.g. the axilla), and flame injury caused by the ignition of clothing and/or the surrounding environment (1). The severity of tissue damage can usually be classified according to the electrical intensity (high vs low voltage), type of current (direct or indirect), amount of electricity, injured part of the body, contact time, difference of resistance, and concomitant secondary injury (2).
At the time of electric shock, the human body acts as a conductor. Electric energy changes to thermal energy, and muscle and bone can be damaged in addition to the skin and soft tissue. Typical high-tension electrical injuries are generally well demarcated, full thickness, and leathery on palpation. Severe damage to an extremity often results in amputation or other handicaps, and digital amputations are seen in lower-tension electrical injuries as well. Electrical burn injuries account for 3%–5% of all thermal burn patients (3, 4). However, they show variable clinical manifestations from small superficial-thickness burns to massively destroyed underlying structures. The authors retrospectively analyzed electrical burn cases and evaluated epidemiological variables, presence of amputation, and reconstructive surgery modality. The aim of this study is to analyze specific aspects of electrical injuries and to identify preventable measures through the parameters mentioned above.
Material and Methods
Patient Selection and Medical Review
From January 2005 to December 2011, a retrospective analysis of clinical records was performed for 625 patients admitted to the Department of Plastic Surgery at Hangang Sacred Heart Hospital. Upon arrival, all patients with electrical injuries were assigned to one of two groups according to electrical intensity. Variables analyzed were as follows: age, sex, total burn surface area (TBSA), injury mode, and whether amputation or reconstructive surgery was performed. In Korea, all domestic electrical power is 110 V or 220 V, and industrial electrical power is over 1000 V (e.g. 3300 V, 6600 V, 22,000 V, 66,000 V, 154,000 V, 220,000 V, etc.). We assumed there were differences between domestic and industrial injuries, so we divided the patients into two groups (with the low-tension group including patients injured with less than 1000 V and the high-tension group including patients injured with over 1000 V) to compare clinical manifestation. We reviewed the frequency of amputations and classified them as minor or major. Minor amputations were performed at the digit level, while major amputations were performed above the ankle or wrist. We also surveyed the variety and frequency of reconstructive flap surgery. This study was approved by the Ethical Committee of Hangang Sacred Heart Hospital, and informed consent was obtained from all participants.
Treatment Strategy
Patients with low-voltage (110–220 V) injuries usually show similar clinical aspects to those with small thermal injuries, without transmission to the deeper structures in the defined local area. Therefore, they were admitted to the general ward directly, and they did not need to be admitted to the emergency unit for further evaluation. Patients with high-voltage injuries show not only variable degrees of cutaneous burns at the entry, exit, and hidden/deeper structures but also serious cardiac derangements. Therefore, they were admitted to the burn intensive care unit (BICU) to monitor cardiac changes and hidden injuries, such as muscle necrosis, after injury. Initial management included fluid resuscitation, electrocardiogram, and cardiac monitoring during the first 24 h. Peripheral circulation was evaluated using Doppler sonography to diagnose compartment syndrome. If any compromises were found, escharotomy or fasciotomy was performed immediately. Urine analysis was evaluated for myoglobinuria. Aggressive fluid resuscitation was performed in the presence of myoglobinuria to maintain urine output at 2 ml/kg/h. If fluid resuscitation was not adequate, 12.5 g of mannitol was administered in addition to resuscitation fluid. Urinary alkalinization was also performed by adding sodium bicarbonate to the intravenous solution. All necrotic wounds were removed by early excision to minimize the risk of infection. After these treatments, deep dermal thickness and full thickness wounds were covered using simple surgical procedures such as skin grafts or artificial dermis. If there were any exposed structures (e.g. bones, tendons, cartilage, nerves), appropriate flap surgeries were undertaken as follows: (1) local and distant flaps in small defects and (2) free flaps for wide and complex defects.
Statistical Analysis
All continuous variables were presented as means ± standard deviation (SD), and the frequencies of categorical variables were presented as percentages. Continuous variables were analyzed with the independent t-test when there was normal distribution. Categorical variables were analyzed with the chi-square test. P values less than 0.05 were considered statistically significant.
Results
Age, Sex, TBSA, and Distribution
The mean age of all patients was 33.4 ± 18.2 years (range = 2–72 years). The mean age was older in the high-tension group (42.3 ± 12.1 years) than the low-tension group (12.1 ± 11.5 years). The ratio of males to females was 13.5 in the whole group. The majority of all electrical burns occurred in patients aged 40–59 years; however, the majority of electrical burns in the low-tension group occurred in patients under 20 years of age, and the majority of electrical burns in the high-tension group occurred in patients aged 40–59 years.
The mean TBSA was 14.0% ± 13.8% in all patients. The mean TBSA was greater in the high-tension group (19.0% ± 13.6%) than the low-tension group (2.1% ± 2.6%). The number of TBSA patients in both groups decreased as the TBSA increased. The proportion in which the burned area was less than 20% was higher in the low-tension group. Table 1 shows the details of age, sex, TBSA, and distribution.
Age and sex distribution and TBSA and TBSA distribution of electrical injured patients.
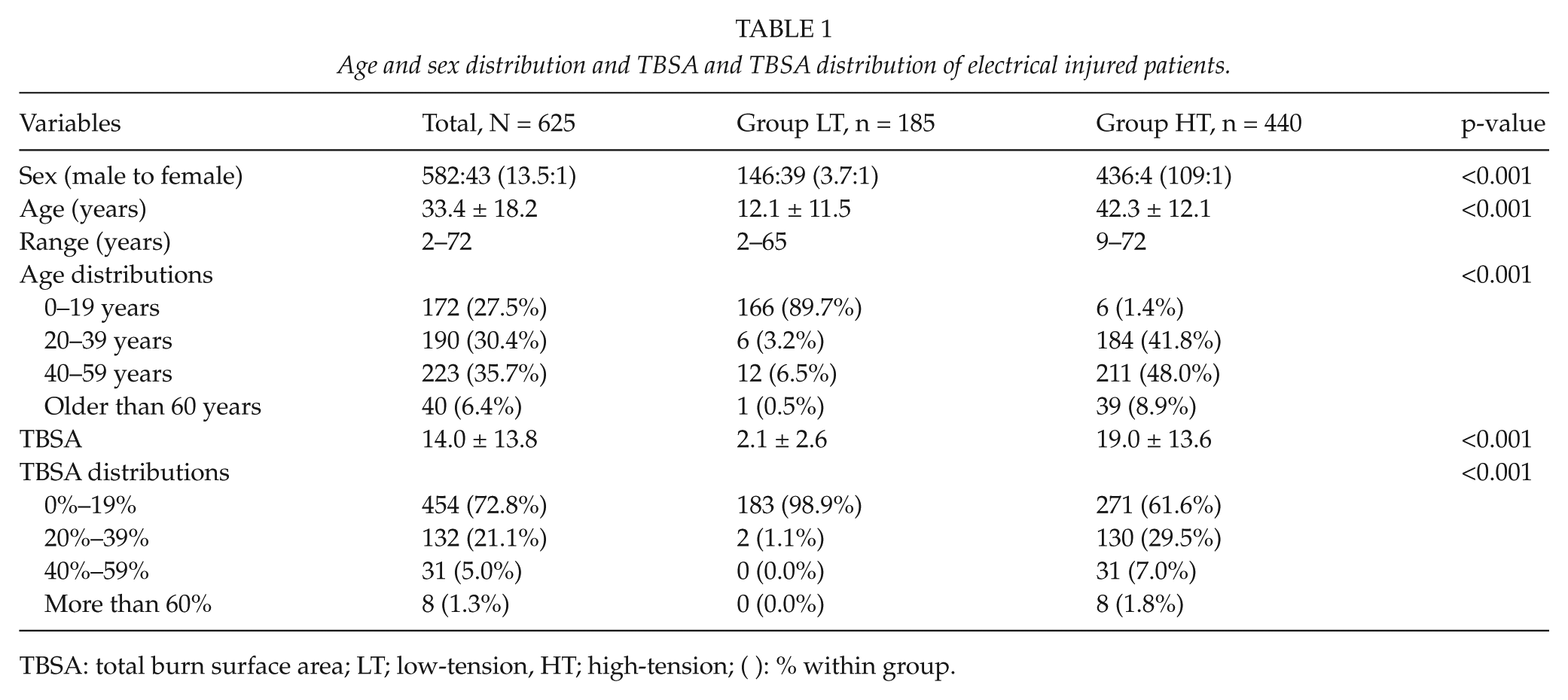
TBSA: total burn surface area; LT; low-tension, HT; high-tension; ( ): % within group.
Type and Mode of Electrical Injury
Thermal injuries with contact-type electrical burns were observed in 351 cases (56.2%) of all electrical burn patients, and this figure was significantly higher in the low-tension group, but the proportion of true electrical- and arc-type electrical burns was significantly higher in the high-tension group.
The most common mode in the whole group was electric work/repair. Inserting steel chopsticks into wall sockets caused 158 of 185 electrical burns (85.4%) in the low-tension group. Electric work/repair was the most common cause in the high-tension group. Table 2 shows the details of the type and mode of electrical injury.
Type and mode of electrical injury.
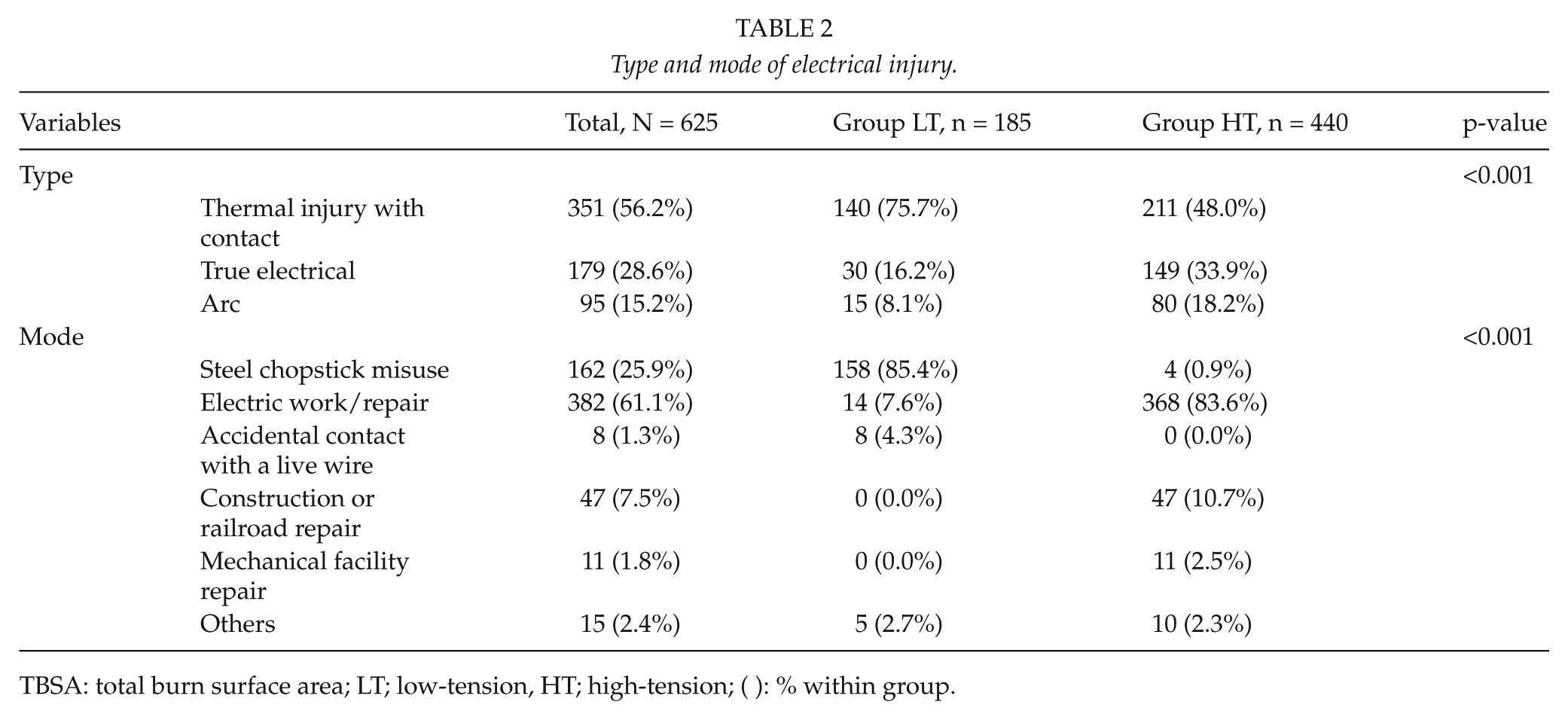
TBSA: total burn surface area; LT; low-tension, HT; high-tension; ( ): % within group.
Amputations
In the low-tension group, 29 of 185 patients (15.6%) underwent an amputation: 24 patients (13.0%) were classified as minor, and 5 patients (2.7%) were classified as major. A total of 38 minor amputations were performed on 24 patients. The right hands were affected in 21 cases, the left hands in 10 cases, the left feet in 5 cases, and the right feet in 2 cases. A total of five major amputations were performed on five patients. In the high-tension group, 329 of 440 patients (74.7%) underwent an amputation. Among them, 222 patients (50.5%) were minor, 89 patients (20.2%) were major, and 18 patients (4.1%) underwent both minor and major amputations. A total of 332 minor amputations were performed on 222 patients. The right hands were affected in 107 cases, the left hands in 83 cases, the left feet in 76 cases, and the right feet in 66 cases. A total of 89 major amputations were performed.
Reconstructive Surgery
In the low-tension group, 67 flap surgeries were performed in 33 out of 185 patients (17.8%). In terms of distant flap surgery, groin flap surgery and abdominal flap surgery were performed in 32 cases and 20 cases, respectively. Free flap surgery (e.g. on the latissimus dorsi and radial forearm) was performed in five cases, and local flap surgery (e.g. on the posterior interosseous, cross-finger, or local transposition flap) was performed on nine cases. In the high-tension group, 644 surgeries were performed on 329 out of 440 patients (74.8%). Distant flap surgery, including groin flaps and abdominal flaps, was performed on 197 cases and 95 cases, respectively. Free flap surgery—such as on the latissimus dorsi, anterolateral thigh, or radial forearm—was performed on 84, 56, and 33 cases, respectively. Local flap surgery—such as on the posterior interosseous, cross-finger, local transposition, or reverse sural flap—was performed on 24, 26, 50, and 31 cases, respectively. Table 3 shows the details of the reconstructive procedures.
Reconstructive procedures (n = cases).
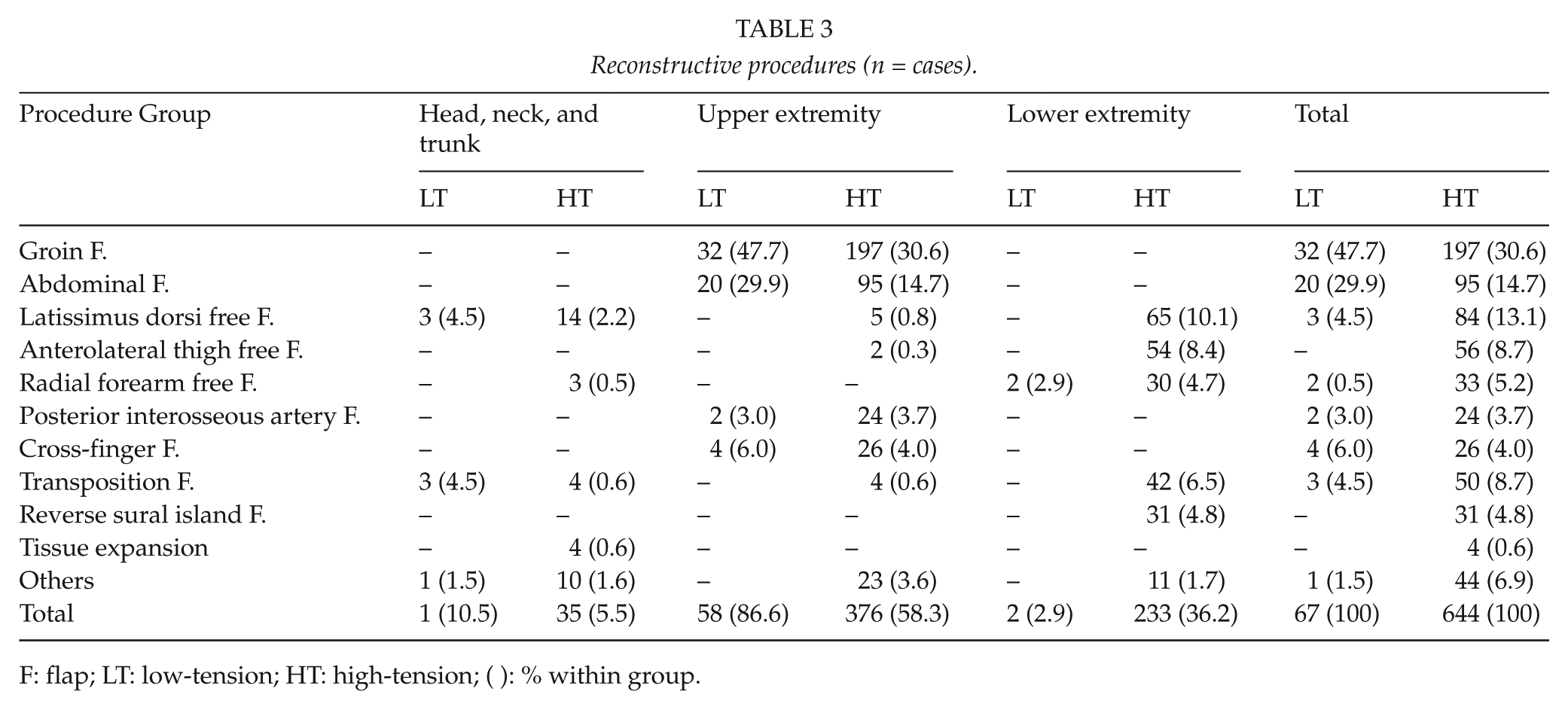
F: flap; LT: low-tension; HT: high-tension; ( ): % within group.
In 63 (94.0%) out of 67 cases and 602 (93.5)out of 644 cases did not need further operations after reconstruction in the low- and high-tension groups, respectively. And, split-thickness skin graft (STSG) was performed in two cases and 34 cases, and a different flap surgery was performed in two cases and eight cases due to a failed previous flap surgery in the low- and high-tension groups, respectively. STSGs were performed to cover small defect of previous operations and appropriate other flap surgeries were undertaken if there were still remained any exposed structures (e.g. bones, tendons, cartilage, nerves).
The following figures show the outcomes of the reconstructive procedures. Fig. 1 shows the anterolateral thigh free flap of the right foot of a 47-year-old man with a high-tension electrical injury. Fig. 2 shows the latissimus dorsi muscle free flap of the right ankle and foot of a 53-year-old man with a high-tension electrical injury. Fig. 3 shows the groin flap of the ulnar hand and posterior interosseous artery flap of the wrist of a 42-year-old man with a high-tension electrical injury.

Intraoperative image showing the right foot of a 47-year-old man with a high-tension electrical injury. (A) The tendon, ligament, and joint of the metatarsal area were exposed and (B) 6 months after anterolateral thigh free flap (B).
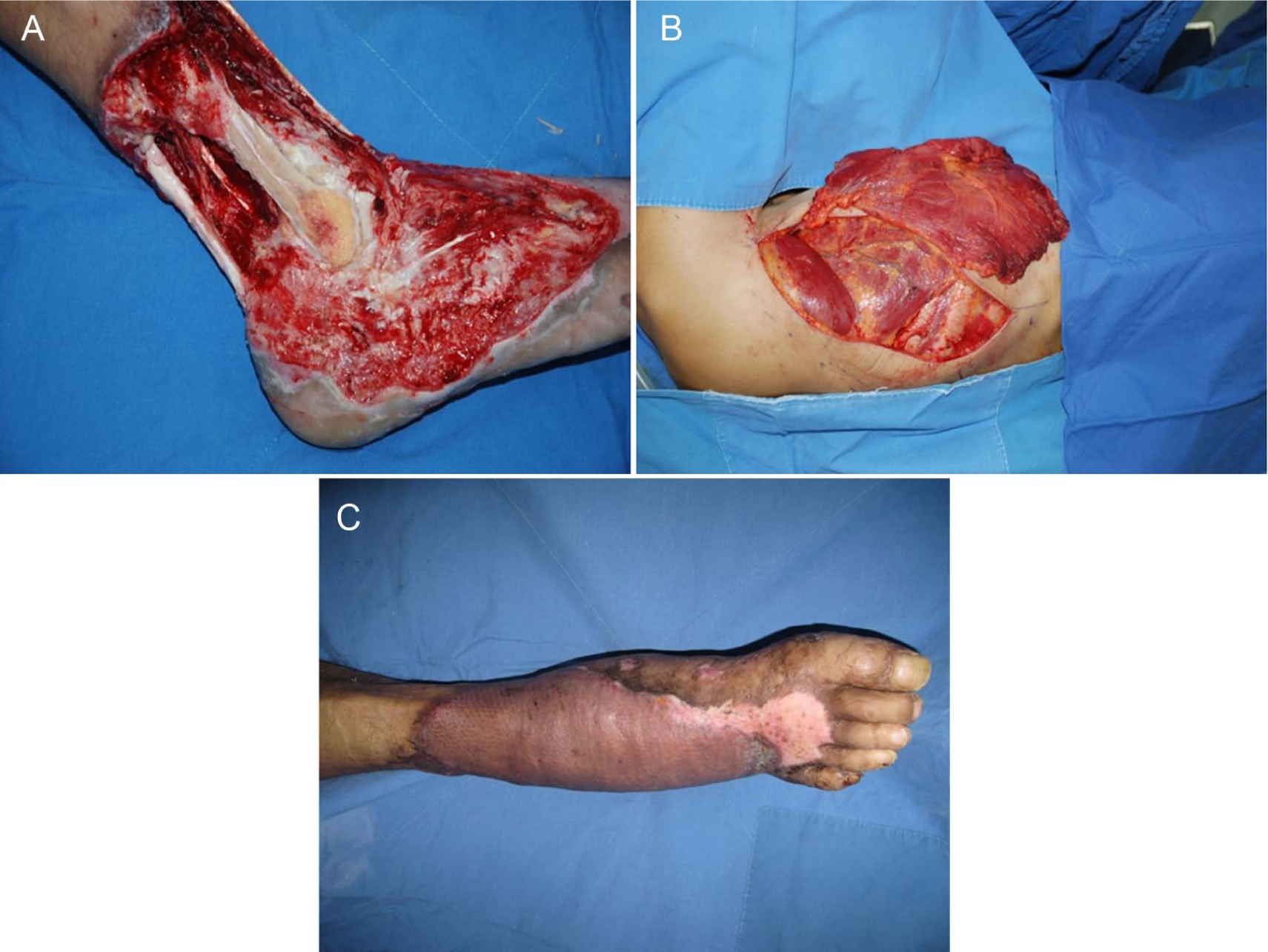
Intraoperative image showing the right ankle and foot of a 53-year-old man with a high-tension electrical injury. (A) The tendon, ligament, and joint of the ankle area were exposed; (B) image of latissimus dorsi muscle flap harvesting; and (C) 1 month after operation.

Intraoperative image showing the left wrist and hand of a 42-year-old man with a high-tension electrical injury. (A) The tendons and nerves of the wrist and ulnar hand were exposed, (B) post-operative image 3 days after groin flap on ulnar hand and posterior interosseous artery flap on wrist; and (C) 3 months after operation.
Discussion
This study attempted to show epidemiological and clinical differences between low- and high-voltage electrical injuries. Based on the reports of other authors (5 –8), low-tension injuries comprise 72.8%–76.3% of all electrical injuries. However, our study showed that low-voltage burns accounted for 29.6% of injuries and predominantly involved patients under 19 years of age. On the other hand, high-voltage burns accounted for 70.4% of all electrical injuries and were observed in patients of working age (i.e. 20–50 years of age). These age patterns are similar to those found in Luz’s study in Brazil, and it is a common feature in developing countries (9). Our study showed that the male proportion was higher in the high-tension group (99.1%) than in the low-tension group (78.9%), since the high-tension group was primarily composed of males in the working age bracket and the low-tension group was composed of young children, many of whom were female, on the other hand. In Korea, steel chopsticks are typically used in daily life; thus, many patients under 20 years of age were included in the low-voltage injury group. In the high-tension group, many patients were injured while performing electrical work/repair, a result similar to that found in another study (9).
In electrical burns, tissue injury is the result of a change from electric energy to thermal energy. In terms of resistance, the skin provides intermediate resistance and is an important factor for impeding current flow. Nerve tissue is the least resistant, and together with the vessels, muscles, and mucous membranes, it offers a path of low resistance for electricity (10). Remnants of the current can cause thermal injury to the muscle, fat tissue, and skin as it moves to an exit site (1, 11, 12). The skin at entry and exit areas is usually blackened by the electrical current, which can also damage internal structures, such as tendons, nerves, or vessels. Therefore, although the treatment of burn injury has advanced with time, electrical burn patients still face treatment difficulties, as the visible areas of necrosis represent only a small part of the tissues that are actually damaged (13). The arc from the electric potential difference can quickly damage muscle. The arc is an intense flame composed of ionized particles with a heat of approximately 3000 °C–20,000 C (10). It can jump over 2–3 cm per 1000 V, and the human body can be damaged without direct contact with the live wire. The result is the typical oval-shaped burn wound frequently observed on the wrist, elbow, or axilla (10, 11, 14).
In addition to the direct damage in high-tension electrical injuries, gradual ischemia is also a serious problem. Thrombus formation at the small artery or arteriole, vessel constriction slowing the blood flow, and tissue necrosis can occur (12, 15). These are contributing factors influencing the decision of amputation. Therefore, in our study, amputations were performed frequently in the high-tension group.
One of the best methods to protect the viable tissue in the initial stage of treatment is early decompression with a fasciotomy of the injured compartment (16, 17). If initial management is completed, the surgeon can consider the next stage of reconstruction. Simple surgical procedures, such as skin grafts or artificial dermis, are useful at first, and regional or free flaps are useful if the injury is severe. Reconstruction other than skin grafts is divided into three categories: local flaps, distant flaps, and free flaps. Local and distant flaps are primarily used to correct small defects, such as those in the low-tension group. In the high-tension group, local and distant flaps were primarily used, but free flaps were also used for wide and complex defects. In the high-tension group, groin and abdominal flaps were the most frequently used, but free flaps were needed to reconstruct wide defects in many cases. In our study, free flaps were performed more in the high-tension group. Latissimus dorsi free flaps were the most commonly used, followed by anterolateral thigh free flaps and other types of free flaps. Small defects in the extremities can be reconstructed with local or distant flaps, such as cross-finger flaps or groin flaps. However, free flaps were inevitable in severe and complex defects with deep structure exposure. Moderately sized defects are typically treated with radial forearm flaps or anterolateral thigh free flaps. Latissimus dorsi flaps are primarily used for extensive defects that are greater than the size of one hand. In our study, almost 94% did not need additional surgery, which we thought was quite a good result. Therefore, when performing flap surgery, we must consider many factors, such as the patient’s general condition, donor condition, surgeon’s skill level, flap character, vessel condition, and possibility of early exercise. In critical situations, such as inhalation burns or septic conditions, reconstructive surgical management cannot be started, because life-saving surgical management, such as an allograft, is typically performed beforehand. Therefore, many high-tension electrical injury patients often do not have the chance to receive an operation to recover function of the affected extremity immediately.
The mortality rate of electrical injury varied from 0% to 21.7% in other studies (9, 14, 18, 19). We did not calculate mortality rate, because non-surviving patients were not included in our study group. In our burn center, acute electrical burn patients at a high risk of death usually receive initial treatment in the Department of General Surgery rather than in the Department of Plastic Surgery. Then, when the condition of the patients has improved and the likelihood of morbidity and mortality has declined, they are transferred to the Department of Plastic Surgery for further treatment such as reconstructive surgery. It is a somewhat different procedure compared to other nations.
In summary, almost all defects can be reconstructed by surgical measures, from skin grafts to free flaps, except serious vascular insufficiencies. However, in cases of compromised vascularity, it is meaningless to perform reconstructive procedures, and this results in amputating the injured area. The best management is prevention through educational programs and social meetings emphasizing household electrical safety and training in the use of industrial electrical equipment for the at-risk groups mentioned above. We also proposed the best methods of treatment by providing our experiences, since the effect of treatment of tissue injured by electrical current varies depending on patient condition.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.