
Abstract
Background and Aims:
Despite several potential complications of elastic intramedullary nailing, it is currently the treatment of choice for femoral diaphyseal fractures in school-aged children. This study aimed to critically evaluate the complications of titanium elastic nailing in pediatric femoral shaft fractures.
Material and Methods:
This study evaluated patients with a diaphyseal femoral fracture treated with titanium elastic nailing (TEN) in Tampere University Hospital in Finland. The study group included 32 children with a mean age of 9 years during a 5-year period, from 1 January 2003 to 31 December 2007. Data were collected from medical records and x-rays. Mean follow-up time was 42 months.
Results:
Of 32 patients, 9 (28%) reported a postoperative complication. Complications were associated with nail prominence in five (16%) patients and instability in four (12%) patients. In patients with nail prominence, the titanium elastic nailing–nail ends were unbent and 10–35 mm outside the cortex of the distal femur. The nail prominence caused pain and delayed knee mobilization until the nail was removed after a mean time of 4 months. In patients with fracture instability, the mean titanium elastic nailing–nail/medullary canal diameter ratio was 46% and periosteal callus formation was 5.4 mm at the first control. In those with stable fractures, the values were 66% and 9.2 mm, respectively.
Conclusions:
Based on this study, two types of pitfalls in a small volume center were found. Titanium elastic nail ends were left unbent and too long. We recommend palpating the nail ends to exclude nail prominence and to verify free movement of the knee after nail cutting and bending. Fracture instability was caused by inserting titanium elastic nailing–nails that were too narrow. To avoid this complication, careful preoperative planning to select the proper-size titanium elastic nailing–nails and intraoperative testing of fracture stability under continuous fluoroscopy after the operation is advised.
Introduction
Although femoral fractures in children account for only 2% of all orthopedic injuries, they have a significant impact on both the patients and their families, and the utilization of trauma resources as these fractures almost always lead to hospitalization (1–3). During the past 20 years, titanium elastic nailing (TEN) has become the most widely used treatment for diaphyseal femoral fractures in school-aged children over 6 years of age (4–6). The advantages of TEN include its minimal invasiveness and the ability for direct mobilization to maintain joint movement and muscle tone as well as normal circulation (7–10). Hospitalization is usually short term and reduces the treatment cost compared to traditional treatments for traction and spica cast (11, 12). In addition, psychological recovery is accelerated by early resumption of functional activity, allowing for a rapid return to school and ordinary family life (11–14). Despite the various advantages of TEN, however, complication rates of up to 60% have been reported, due mostly to incorrect operative techniques and poor patient selection (15–22). The most common reported complication is soft-tissue irritation at the TEN entry side (15–22). Nail prominence can lead to more serious complications such as skin breakdown; superficial or deep infection, such as osteomyelitis; early implant removal; and risk of re-fracture (5, 8, 9, 11, 20). Other common complications include the inability to achieve a stabile reduction or loss of reduction that can lead to delayed fracture union (up to 16% of reported complications), angular malunion, or uncommon rotational malunion (17, 22). In the present study, we critically assessed the complications and pitfalls associated with femoral diaphyseal fractures treated with TEN in a limited pediatric cohort in which the incidence of fractures suitable for TEN is quite low.
Material and Methods
The study covered all children and adolescents younger than 18 years with a diaphyseal femoral fracture treated at Tampere University Hospital in Finland during a 5-year period from 1 January 2003 to 31 December 2007. Data were collected by applying a main diagnosis of diaphyseal femoral fracture (S72.3) and two operation codes (NFJ60, NFJ64) from the electronic hospital registry. Information obtained from patient files included patient age, sex, weight, injury mechanism, and fracture type. Fractures were classified according to the Orthopaedic Trauma Association and Gustilo-Andersson classifications. The surgical technique for fixation and complications were recorded from pre- and postoperative x-rays and patient records. Fracture stability/instability was evaluated by comparing fracture position changes between intraoperative x-rays and postoperative x-rays. Cases where the position of the fracture was changed were considered as instable and a cast was applied. The TEN-nail/medullary canal diameter (ND/MD) ratio was evaluated. Duration and time of day of the surgery (day/night) as well as experience of the surgeon (resident/senior) were collected from the patient’s surgical record. The surgeon was considered senior after 10 years clinical experience. The periosteal or secondary callus formation was measured from the follow-up x-rays at the first postoperative clinical visit (4–6 weeks after the initial operation) before gradual limb weight-bearing permission was granted. Physical exercises were forbidden for 3 months. Nail tip prominence was recorded as the maximum transverse distance measured from the side of the femur to the distal tip of the nail on the anterior–posterior or lateral radiographs. The distance of the TENs were measured directly after the initial operation and at the first control (mean of 4 weeks after operation). Patients were followed up from 15 to 57 months (mean 42 months), and the follow-up included radiological and clinical evaluation. Functional outcome was assessed clinically by comparing the operated side to the uninjured side.
A total of 102 patients with a diaphyseal femoral fracture younger than 18 years were treated in pediatric unit in Tampere University Hospital during the 5-year study period. Patients older than 16 years were treated with stable intramedullary nailing or plating, and patients younger than 5 years of age were treated with a spica cast. A total of 32 patients (mean = 6.4 fractures per year) suitable for TEN were included in the study. Of these, 22 (70%) were boys and 10 (30%) girls. The mean age of both boys and girls was 9 years. Injuries were mainly related to high-energy accidents such as motor vehicle or snowboard accidents (21, 66%) or playground injuries (9, 28%), such as falling to ground from monkey bars in healthy children. Only two injuries (6%) occurred following very low-energy activities, such as stretching or walking: one in a patient with neuromuscular disease and another with a simple underlying diaphyseal femoral cyst.
Results
Of 32 fractures, 23 (72%) were united without any problems, and 9 (28%) fractures were associated with skin irritation or fracture instability. All fractures were considered united at the 12-week control and patients were allowed to start free mobilization at that time. Two same-size TENs were inserted in all fractures except in two patients who required insertion of three TENs. Most operations were performed by a senior orthopedic surgeon (25, 78%).
Complications were mainly related to the ND/MD ratio, that is, fracture instability and prominence of the TEN at the entry site causing skin irritation and delayed mobilization (Table 1). There was no association between the fracture type and occurrence of complication (Table 2). Two patient fractures were classified as Gustilo-Andersson grade I and II; these fractures united without complications.
Differences between two study groups: patients without postoperative complications and those with postoperative complications.
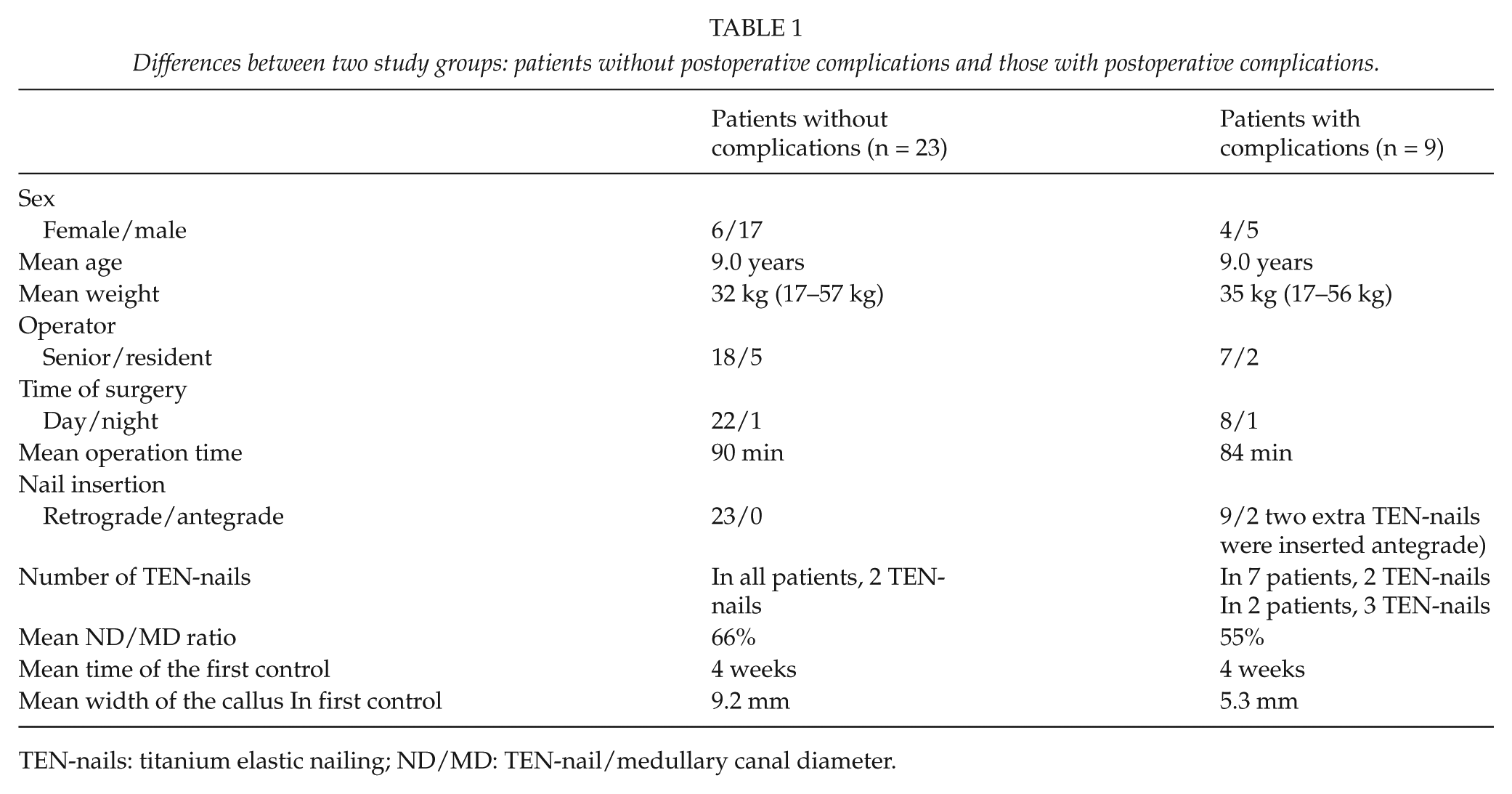
TEN-nails: titanium elastic nailing; ND/MD: TEN-nail/medullary canal diameter.
Fractures divided according to the OTA classification and three study groups: patients without postoperative complications and those with postoperative nail prominence or fracture instability.
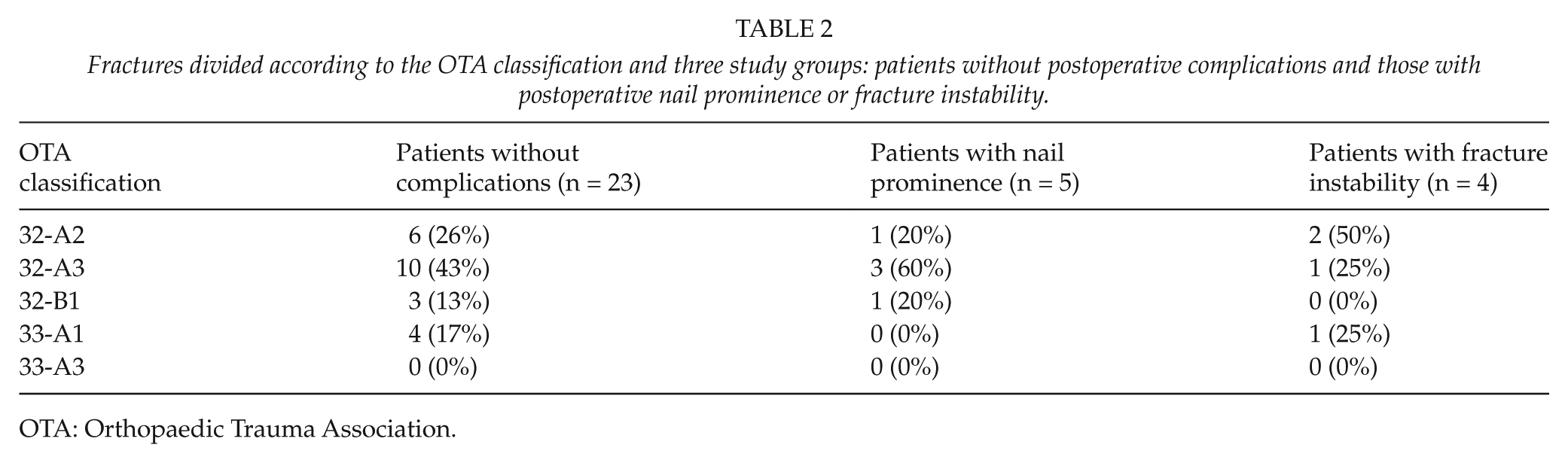
OTA: Orthopaedic Trauma Association.
Patients with postoperative complications included five patients (16%) with pain or skin irritation at the TEN entry side in the distal femur. In three of five patients, two same-size TENs were inserted retrogradely, while in the other two patients, three TENs were inserted; two same-size TENs inserted retrogradely and a third 1.5-mm TEN inserted anterogradely. The complication was observed immediately after the operation or at the first control but did not lead to skin breakdown or reoperation during the follow-up. This complication was strongly associated with nail ends that remained extended at the entry site without being bent toward the side of femur (Fig. 1). All TENs causing pain or skin irritation extended mean 17 mm (10–35 mm) from the cortex and were left unbent toward the skin. In all patients, pain and skin irritation delayed knee motion and overall mobilization until the TEN removal (mean = 4 months compared with 6 months in patients with instability problem and 9 months in patients without complications). A senior pediatric orthopedic surgeon operated on four of the five patients.

An 8-year-old girl with nail prominence causing pain and skin irritation.
In four patients (12%), the fractures were considered unstable after the primary operation (Fig. 2). Fracture was considered unstable if the fracture position was changed between intra- and postoperative x-rays and ND/MD ratio was below 80% at the same time. The differences between groups were considered to be only minor, except for in the ND/MD ratio and periosteal callus formation (Table 3). The ND/MD ratio varied from 36% to 56% (mean 46%) and was lower in those with unstable fractures than in the other groups. All four patients were immobilized with an over-the-knee cast and/or wheelchair at least until the first control (3–5 weeks). A senior pediatric orthopedic surgeon operated on three of the four patients.

A 10-year-old boy with postoperative fracture instability.
Differences between patients without postoperative complications and those with postoperative nail prominence or fracture instability.
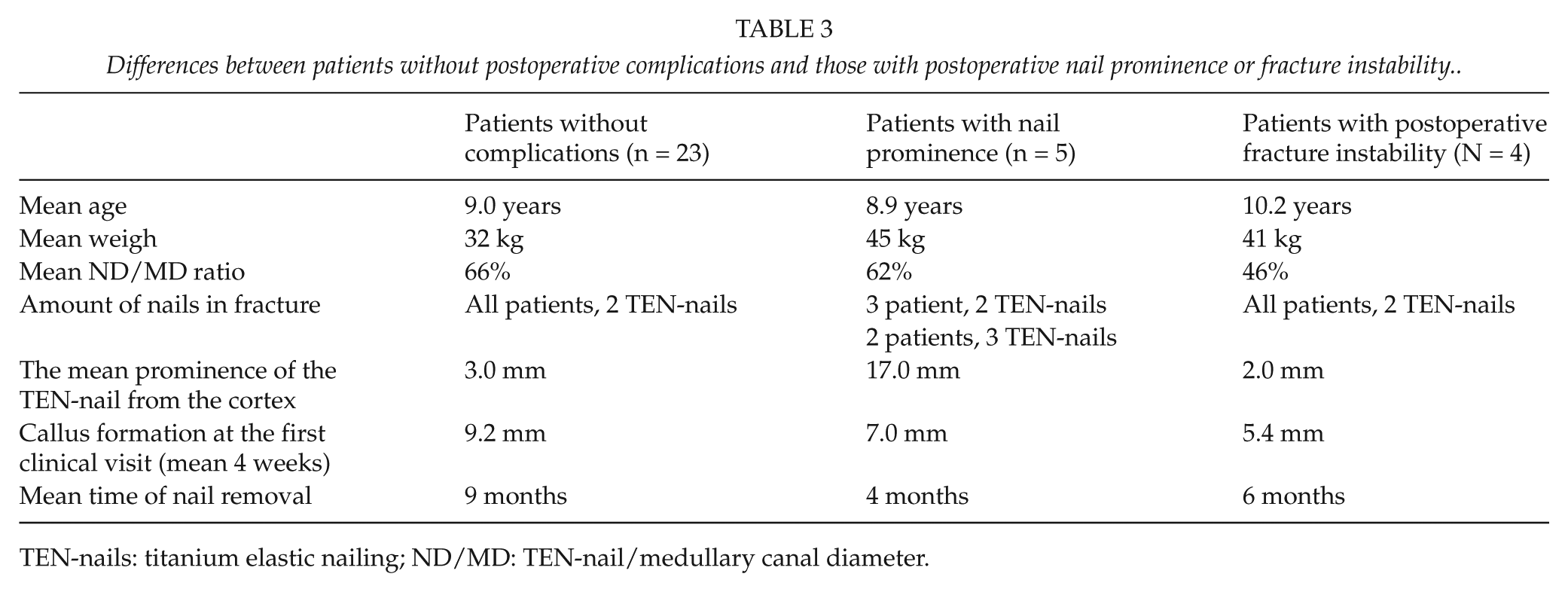
TEN-nails: titanium elastic nailing; ND/MD: TEN-nail/medullary canal diameter.
Two of the four patients were previously healthy, one patient had a neuromuscular disease, and the other’s fracture was caused by a simple cyst (cyst diameter was as wide as the intramedullary width of femur) in the diaphyseal femur.
The patient with neuromuscular disease required reoperation because a TEN-nail slid out from the intramedullary canal soon (2 weeks) after the primary operation. The ND/MD ratio was 46%. A same-size TEN-nail was reinserted and trimmed, but it slid out again, producing a skin prominence. The TEN was finally removed after 2 months. There was no problem with the other TEN-nail, which was removed 10 months after the primary operation.
The patient with a fracture caused by the simple cyst was immobilized immediately after the primary operation. The ND/MD ratio in this patient was 55%. Despite over-the-knee cast immobilization for 7 weeks after the primary operation, a 12° varus deformity developed and was noticed at the 3-month control, when total bone union was recorded. A corrective osteotomy was performed 6 months after the primary fracture operation. There were no further complications associated with the primary fracture or corrective osteotomy.
In this study, there were no complications associated with the removal of the TEN-nails.
Discussion
The principal aim of this study was to critically analyze postoperative complications associated with diaphyseal femoral fractures treated with TEN in a limited pediatric cohort in which the incidence of femoral diaphyseal fractures suitable for TEN is quite low. The complication rate was 28%, and the two main complications were nail prominence caused by long unbent distal TEN ends at the insertion side and fracture instability after surgery, resulting from the application of TENs that were too thin.
Based on the literature, elastic titanium nailing is currently the most popular operative method of fixation of femoral diaphyseal fractures in children, despite reported complication rates of up to 60% (4, 6, 9, 16). In our study, the low complication rate of 28% may be partly explained by the experience of the surgeon. On the other hand, complications concerning the TEN technique also occurred in patients operated on by experienced senior orthopedic surgeons. Predictors of complications and or outcome have been reported in several large studies from centers treating considerable numbers of patients per year (18, 20, 22). The most common complication associated with TEN is pain or skin irritation at the nail insertion site caused by a prominent nail end (19, 20). In our study, nail prominence was the most reported complication causing pain and delayed knee mobilization. Patients with nail irritation were in average heavier and older than the other patients, so it is possible that the amount of subcutis was considered by an operating surgeon to be sufficient enough to cover unbend nail. Additionally, inconvenience and delayed mobilization nail prominence can lead to more severe complications like deep infection or osteomyelitis after skin breakdown and early implant removal with the risk of re-fracture (15, 19). To prevent these complications, it is recommended that the nail ends be trimmed to 1–2 cm from the cortex and unbent nails ends should be applied close to the supracondylar flare at approximately the level of the physis (15, 20, 21). Technical modifications to standardize the cut point of the nail or to improve the nails by precurving the tip and shaft could also solve some of the nail prominence problems (23, 24). After skin closure, the nail ends under the skin should be palpated while moving the knee to exclude a disturbing nail prominence (21).
In our study, fracture instability was recognized in four patients immediately after the primary operation. In these patients periosteal callus formation was reduced (5.4 mm compared to 9.2 mm in patients without complications) at the first control. Based on animal studies performed by Claes et al. (25) and Aro and Chao (26), periosteal (or secondary) callus formation occurs faster with transverse stable fractures and is delayed in unstable fractures with wide fracture gaps. Instability, leading to a loss of reduction and malunion, is associated with the use of mismatched nail size as well as patients heavier than 49 kg and older than 10 years (17, 18, 21, 27). In the present study, neither patient weight nor age exceeded previous recommendations (17, 18, 21, 27). According to Flynn and Schwend (5), to prevent fracture instability, the ND/MD ratio of the narrowest diameter of the medullary canal should be up to 80% and both TEN-nails should be of the same diameter. Knee immobilization for up to 2 months with a hip–knee–ankle–foot orthosis or cast is advisable after fracture instability (9). In our study, patients with fracture instability were immobilized with an over-the-knee cast and/or wheelchair. Despite immobilization, one patient with over-the-knee cast developed varus deformation. Flynn et al. (9) recommend knee immobilization for up to 2 months with a hip–knee–ankle–foot orthosis or cast after fracture instability. Based on our study, we recommend to focus on to preventing instability, instead of postoperative casting, by selecting wide-enough TENs and testing the fracture stability under fluoroscopy after insertion of the TEN-nails.
In our study, all TENs were removed without complications. Routine removal of TEN-nails is controversial; a clear recommendation does not exist, although the removal complication rates are reported as high as 34% (22, 28, 29). Most authors still recommend nail removal within 1 year after the operation to prevent difficulties in future orthopedic procedures, nail irritation or prominence problems, and so on (9). In our study, most of the problems arise from TEN irritation. These problems could have been avoided by inserting the TEN-nails into the intramedullary canal and left unremoved as rigid intramedullary nails. Giving recommendations on the subject is, however, difficult because future risks of unremoved TEN are not known due to lack of long-term follow-up studies.
Based on this study, the pitfalls of TEN-nailing in pediatric surgery unit in which the incidence of femoral diaphyseal fractures suitable for TEN is low are associated with implant application and selection of proper-size TENs. To avoid these complications, we recommend first measuring the width of the intramedullary canal preoperatively and then choosing two wide-enough, same-size TENs. After positioning the chosen TENs, fracture stability should be verified under continuous fluoroscopy and free knee movement without nail prominence confirmed.
Footnotes
Declaration of Conflicting Interests
None declared.