
Abstract
Background and Aims:
Retrosternal goiter may cause symptoms of airway obstruction and dysphagia, but often it is asymptomatic and is increasingly detected incidentally with imaging investigations. Consensus has been reached that sternotomy is not necessary in most cases, as a collar incision normally suffices. Yet, surgery for retrosternal goiter is associated with more complications than cervical goiter. There is controversy over whether patients with asymptomatic retrosternal goiter should be operated. Proponents argue that retrosternal goiter may be a risk for thyroid cancer and may progress to later cause symptoms, although clear evidence is missing.
Patients and Methods:
Between 1984 and 2012, 132 patients underwent surgery for benign retrosternal goiter. Preoperatively, the benign nature was clinically apparent and confirmed by fine needle cytology in most cases.
Results:
Sternotomy was required in only 4 of the 132 operations. Three patients died in the postoperative period. The risk of morbidity and mortality was 16.7% in 60 patients with compression symptoms and 13.9% in 72 patients without compression symptoms (P = 0.808). Histology revealed no case of unsuspected cancer.
Conclusion:
Surgery for retrosternal goiters involves a higher risk for complications than do cervical goiters, and the risk does not differ between patients with and without symptoms. This, and the fact that no patient in this study had unsuspected cancer, calls into question the rationale for surgery in patients with asymptomatic retrosternal goiter without suspected cancer.
Keywords
Introduction
Retrosternal extension of goiters is not uncommon—in iodine-deficient areas it has been reported to occur in as many as 25% when screening persons over 70 years of age with no evident thyroid disease (1). Accordingly, all surgeons treating thyroid disorders will be faced with the particular problems associated with retrosternal goiter, both preoperatively when deciding the proper indications for surgery and at the operating table when removing the intrathoracic goiter with a minimum of morbidity. Despite the high prevalence, there is some controversy as to which patients with retrosternal goiter should be subject to surgery. A majority of endocrine surgeons seem to argue that virtually all intrathoracic thyroids should be removed (2–9); a few others contend that only patients with symptoms or suspected cancer need an operation (10). By contrast, agreement has been reached that sternotomy is not to be recommended routinely as a collar incision is sufficient in most situations (11). This article reports the results of 132 consecutive operations for intrathoracic goiter at a district hospital during a 30-year period when wide indications for surgery were applied. The results call into question that all asymptomatic patients with intrathoracic goiter really should be recommended surgery.
Patients and Method
All 1022 patients operated between 1984 and 31st August 2013 for thyroid diseases at the Department of Surgery at Highland Hospital in Eksjö, Sweden, were recorded prospectively. This study cohort comprised 132 patients (92 women and 40 men) with a benign retrosternal goiter, defined at the operation as >50% of thyroid volume situated below the thoracic inlet. Median age was 63 years (range 16−88 years). Toxic nodular goiter was present in 22 patients (16.7%), whereas the remaining 110 patients (83.3%) had a nontoxic nodular goiter or thyroid adenoma. Eight of the 132 patients had undergone previous thyroid surgery, 6 of them on the same side as the current operation, that is, “true” redo-surgery. A total of 18 patients with preoperatively verified thyroid cancer extending retrosternally were excluded from the study.
Preoperative Investigation
The histological diagnosis was reached preoperatively with fine needle aspiration cytology in a majority of the 132 patients. Before 2002, the retrosternal nature of the goiter could be suspected with clinical examination and/or plain chest X-ray, but only a few computed tomography (CT) investigations were performed. From 2002 onward, the majority of patients had their goiter characterized preoperatively with CT.
Surgical Procedures
All operations were performed by one single surgeon (Johannes Järhult), using a standard collar incision. Supplementary sternotomy was carried out only when it proved necessary during the operation. The recurrent laryngeal nerves were not searched for routinely, but were nonetheless frequently identified at the last 1–2 cm before their entrance into the larynx.
Definition of Complications
Pre- or postoperative laryngoscopy was not carried out routinely, but only when clinically indicated. Reasons for preoperative vocal cord examination were either previous thyroid surgery or the patient’s own concerns about the voice. Postoperative laryngoscopy was performed after suspected injury to the nerve during surgery or when the patient expressed misgivings about the voice after surgery, even if the responsible surgeon perceived the voice to be normal (12). A palsy of the recurrent laryngeal nerve was considered as permanent if it persisted for 1 year after surgery. Permanent hypoparathyroidism was defined as requirement of vitamin D and/or calcium supplementation to maintain normocalcaemia 6 months postoperatively.
Follow-Up
The patients were followed until 31 August 2013, at which time 34 patients had died. Median follow-up time was 116 months (5 days−328 months).
Ethical Considerations
The study was approved by the Regional Ethical Review Board at Linköping University, Sweden.
Statistics
Fisher’s exact test was used to test differences in proportions.
Results
In this study, 83 patients had retrosternal goiter on the left side, 35 on the right side, and 14 on both sides. Subjective respiratory problems were the predominating symptom upon presentation in 37 patients (28.0%) (Table 1). A total of 57 patients (43.2%) had no complaints at all referable to the goiter, 25 of whom had not even noticed any swelling.
Main presenting symptom a in 132 patients with retrosternal goiter.
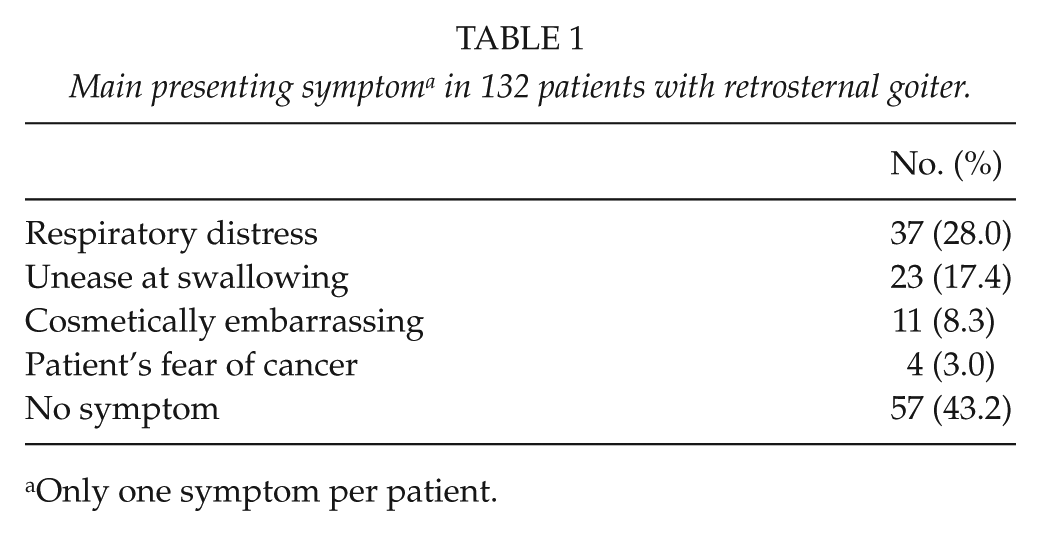
Only one symptom per patient.
Table 2, listing the performed operations, shows that sternotomy was necessary only for four patients (3.0%). Median weight of the specimen was 136 (28−511) g. All specimens were sent for histopathological analysis; nodular goiter was found in 114 patients, whereas 18 patients had various benign thyroid adenomas. Importantly, no case of unsuspected thyroid carcinoma was detected.
Procedures performed in 132 patients with retrosternal goiter.
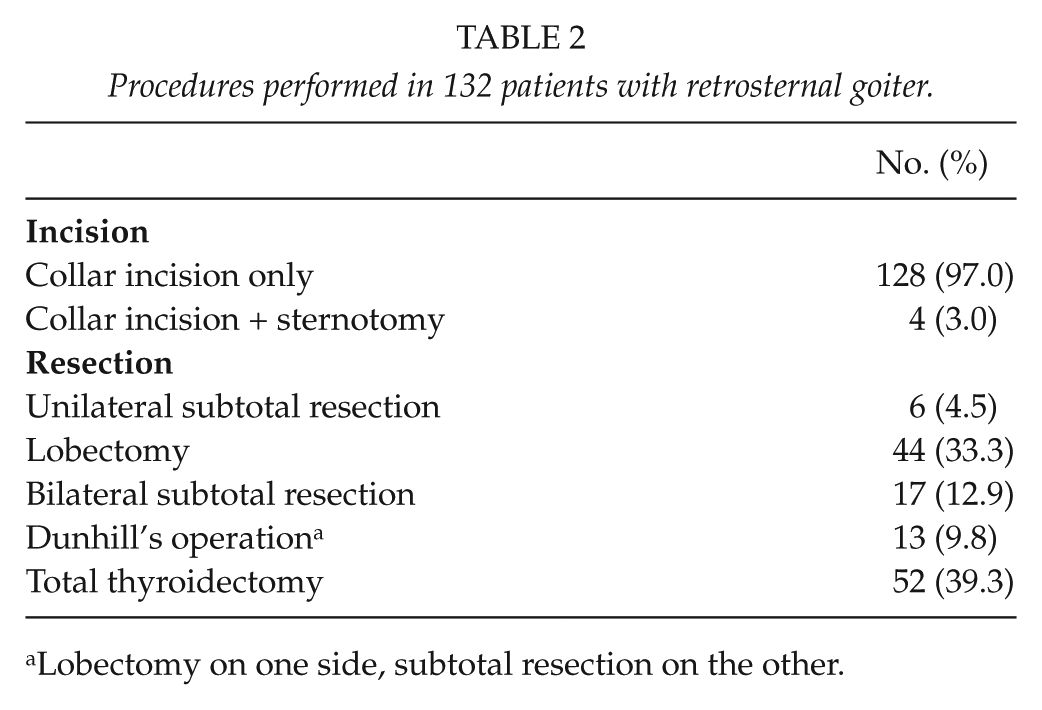
Lobectomy on one side, subtotal resection on the other.
Table 3 shows postoperative complications and mortality. Three old (all over 80 years) and multimorbid patients died in the immediate postoperative period due to pneumonia (n = 1) and circulatory failure (n = 2). No patient in this series suffered tracheomalacia or required tracheostomy after surgery. The risk of morbidity and mortality did not significantly differ between patients with compression symptoms (respiratory distress or unease at swallowing) (16.7%) and patients without compression symptoms (cosmetically embarrassing, patient’s fear of cancer or no symptoms) (13.9%) (P = 0.808). One of the six patients with previous ipsilateral thyroid surgery suffered a permanent recurrent laryngeal nerve palsy, and there were no other complications or mortality in this group.
Postoperative complications in 132 patients with surgery for retrosternal goiter.
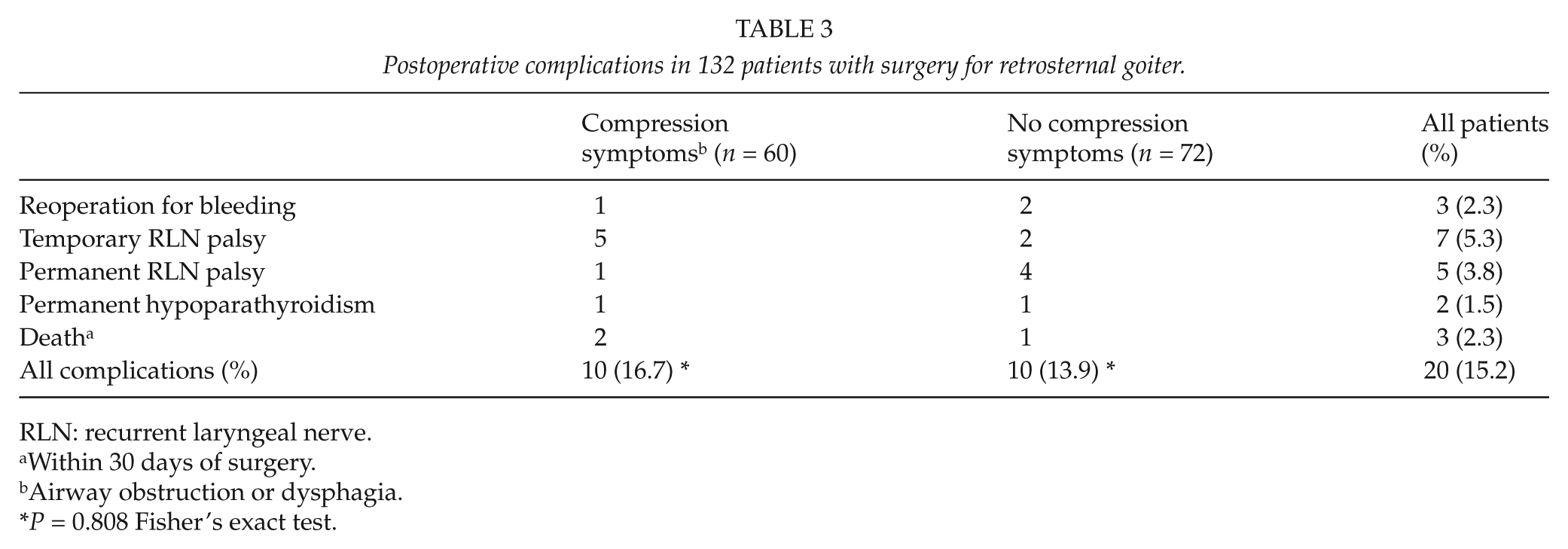
RLN: recurrent laryngeal nerve.
Within 30 days of surgery.
Airway obstruction or dysphagia.
P = 0.808 Fisher’s exact test.
At follow-up, most patients (95%) with preoperative respiratory problems were completely relieved; the two remaining patients both had markedly improved symptoms.
Discussion
Results of surgery for retrosternal goiter are difficult to assess owing to the various definitions of the condition. When Ríos et al. (13) applied eight different definitions in a material of multinodular goiter treated with thyroidectomy, the frequency of intrathoracic goiter varied between 2.8% and 48%. Still, the results presented in this study are in keeping with those reported in the systematic review presented by White et al. (11). Thus, most authors find that retrosternal goiters as a rule can be managed via a standard collar incision and that the frequency of injury to the recurrent laryngeal nerve is higher than after surgery of goiters confined to the neck (8, 11, 14). The mortality rate in this study was 2.3% in comparison to none in 809 cervical goiter patients treated in our institution during the same period of time (P = 0.003) (Järhult, unpublished results). Mortality in connection with surgery for retrosternal goiter is rarely discussed in the literature. As an exception, Pieracci and Fahey (8) found a significantly higher risk of postoperative mortality in patients with substernal compared to cervical goiter among 33,390 thyroidectomy patients.
Patients with symptomatic retrosternal goiter should generally be recommended surgery, and the effect of surgery on respiratory symptoms was excellent in this study. It is less clear how asymptomatic patients should be managed. Several authorities advocate wide indications for surgical removal of intrathoracic goiters, including notable British endocrine surgeons Hardy, Bliss, and Lennard (9), who claimed that “thyroidectomy should be performed in all patients with retrosternal goitre who do not have medical co-morbidity excluding them from surgery.” Their recommendation was based on the suppositions that patients with retrosternal goiters are at increased risk for thyroid cancer and later severe respiratory problems. It is also feared that untreated substernal goiters may hinder endotracheal intubation during later anesthesia for whichever purpose. However, neither of these indications seem to have much scientific support. In their systematic review, White et al. (11) did not find any substantial data to show that the incidence of cancer is higher in substernal than in cervical goiters. Likewise, there was no case of unsuspected malignancy among our 132 patients with preoperatively diagnosed benign goiter. All cases of intrathoracic thyroid cancer were identified preoperatively by clinical examination and verified by preoperative cytology. The frequency of failed intubation in patients with substernal goiters seems to be low (15, 16), and the notion that most retrosternal goiters will progress and eventually cause severe respiratory distress has not been studied as far as we are aware of. Neither has it been shown that patients with asymptomatic retrosternal goiter do better with surgery than without. A randomized trial comparing expectancy with surgery in these patients would therefore be of great interest, not least in view of the increasing number of incidental retrosternal goiters found by imaging modalities for conditions unrelated to thyroid diseases. It should be noted that the radiological appearance of retrosternal goiter correlates poorly with both subjective experience and objectively recorded diagnosis of upper airway obstruction (17).
Further reason to question surgery in asymptomatic patients is the present finding that postoperative morbidity and mortality does not significantly differ from that of patients with symptoms. It should here be pointed out that the presence of symptoms might even have motivated higher operative risks in a few patients with relative contraindications.
An alternative treatment to reduce the volume of a large intrathoracic goiter is to use radioiodine, which has been reported to diminish the goiter volume by 30% (18). However, the effect is unpredictable and there are certain problems associated with the method (19).
In conclusion, our data indicate that morbidity and mortality rates are substantial after surgery for retrosternal goiter, particularly in old age. Since the natural history of asymptomatic retrosternal goiter is unknown, surgery in these patients seems not to be mandatory.
Footnotes
Declaration of Conflicting Interests
None.
Funding
The study was supported by grants from Futurum—the Academy for Healthcare, County Council, Jönköping, Sweden.