
Abstract
Background:
Treatment of open fractures continues to be a challenge for orthopedic and trauma surgeons, and early treatment recommendations, which persist in the literature for decades, often do not have supporting data.
Methods:
This is a critical review of the literature surrounding controversies in the initial management of open fractures. It also focuses on the utility of negative pressure dressings in the care of associated complex wounds. Studies were selected based on their relevance to the treatment of open fractures.
Results:
A total of 40 studies were included. The following topics were critically discussed: timing of initial debridement, antibiotic coverage, utility of obtaining cultures, and timing of wound closure.
Conclusion:
The majority of open fractures require urgent, not emergent, irrigation and debridement. Antibiotics are essential in preventing infection in open fractures. Timely wound closure after all necrotic tissue has been debrided decreases complications in open fractures. Finally, negative pressure wound therapy has dramatically changed the care of associated complex wounds.
Introduction
Open fractures are one of the most challenging injuries in trauma care. Compared to closed fractures, they have a significantly higher risk of infection, nonunion, wound healing complications, and often require multiple surgeries for definitive care. In addition, these fractures, in association with soft tissue destruction, may trigger and fuel systemic inflammation. Consequently, a multidisciplinary approach including teams of orthopedic, trauma, and plastic surgeons is commonly required to address the needs of patients with open fractures.
The most debated controversies with regard to the initial management of open fractures include timing of initial operative debridement, choice of antibiotic, and time to wound coverage. The purpose of this review is to critically evaluate the current literature on these controversies.
Classification
To better understand the controversies surrounding the management of open fractures, it is important to recognize their most commonly used categorization scale, the Gustilo–Anderson Classification (1). This classification system, which was corroborated by other investigators (2), correlates with the risk of infection and nonunion and therefore provides the platform for treatment guidelines.
The Gustilo–Anderson Classification divides fractures into three types in an ascending order of severity. It is based on the mechanism of injury, soft tissue damage, length of skin laceration, fracture pattern, and degree of contamination. According to this classification, in Type I fractures, the wound is less than 1 cm in length and clean (Fig. 1), whereas in Type II, the wound is greater than 1 cm and has minimal soft tissue damage and intact periosteum (Fig. 2). These wounds can be primarily closed either immediately or delayed. Type III fractures include those injuries with significant periosteal stripping, segmental fractures, extensive soft tissue wounds, vascular injury requiring repair, or high-velocity gunshot wounds (Fig. 3). After the recognition that Type III fractures carries varying degrees of prognosis and outcome, this type of open fracture was subdivided into three different categories (3). Type IIIA injuries are those with adequate soft tissue coverage of the bone that does not require a rotational or free flap, as well as fractures with high-energy mechanisms and significant soft tissue damage irrespective of wound size. In Type IIIB fractures, there is inadequate soft tissue coverage of the bone and massive contamination, necessitating flap coverage (Fig. 4). Type IIIC injuries are those with vascular disruption requiring repair (Fig. 5). Type IIIB and IIIC fractures have higher rates of infection and amputation compared to Type IIIA injuries. In addition, all Type III open fractures have a higher incidence of gram-negative infection, and the addition of aminoglycosides is commonly used for these fracture types (1, 3). Nevertheless, it should be noted that there are no data supporting that the addition of gram-negative coverage decreases the infection rate.

Type I open fracture.

Type II open fracture.

Type III open fracture.
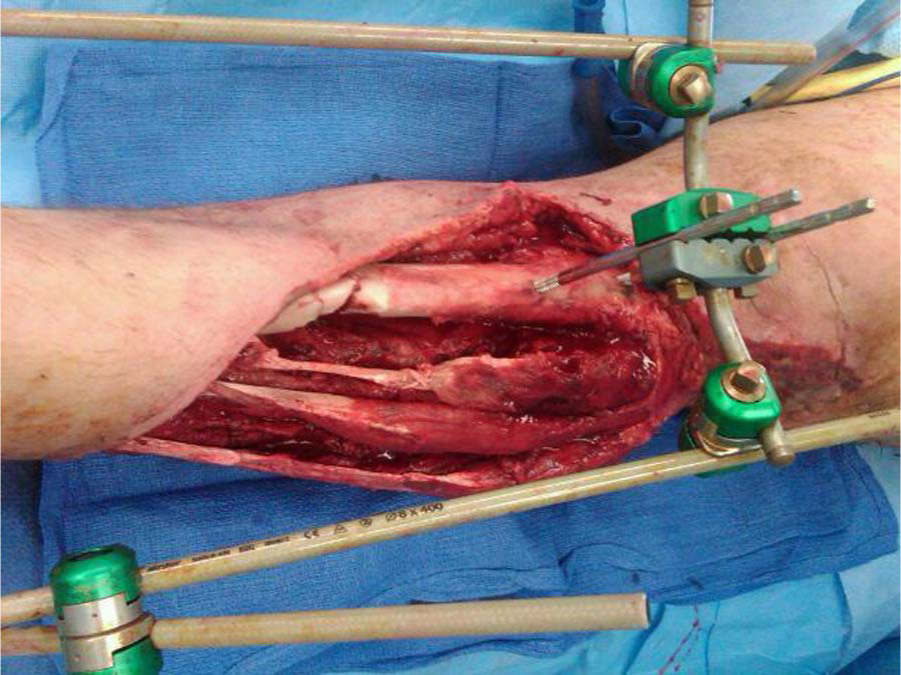
Type IIIB open tibia fracture requiring rotational/free flap.

Type IIIC open femur fracture with vascular injury.
Finally, the type of open fracture may not be determined until after final debridement. For example, it is possible that an open fracture with a 1-cm skin laceration, initially classified as Type I, may actually be a Type II or III after debridement of all contaminated or nonviable soft tissues.
Antibiotic Coverage in Open Fractures
What is Agreed Upon?
There is strong evidence for using systemic antibiotics in the treatment of open fractures. This has been first established by the landmark study by Patzakis et al. (4). In this prospective randomized controlled trial, 330 open fractures were randomized to either receive a first-generation cephalosporin, penicillin and streptomycin or a placebo. The duration of antibiotic varied from 10 to 14 days depending on whether internal fixation was used. There was a significant difference in infection rates between the cephalosporin (2%) and penicillin/streptomycin (10%) or placebo (14%) groups. The efficacy of antibiotics was also established by another study, which reviewed over 1100 open fractures (5). Interestingly, the authors of that study, overwhelmed by the demonstrated protective effect of antibiotics, suggested that future placebo-controlled studies are “not warranted.”
What is Controversial?
In contrast to the use of first-generation cephalosporins, the administration of aminoglycosides for more complex open fractures (Type III) is controversial. In his original paper describing Type III open fractures, Gustilo reported that 77% of bacteria isolated from infections were gram-negative organisms. Therefore, he concluded that adding an aminoglycoside or using a third-generation cephalosporin for gram-negative coverage is indicated in Type III open fractures (3), a dogma which has propagated throughout the literature. However, as Gustilo did not study whether the addition of an aminoglycoside actually decreases the rate of infection in Type III fractures, his recommendation to add gram-negative coverage is not valid.
In a follow-up retrospective study, Patzakis et al. (6) reported that the addition of aminoglycosides to cephalosporin decreased infection rate compared to cephalosporin alone (13% vs. 5%). However, this study has several flaws, which cast doubt on the validity of its findings. For example, the duration of antibiotics as well as wound closure management (i.e. primary closure vs. leaving the wound open) varied among the groups.
More recently, Patzakis et al. (7) tested the hypothesis that a single agent, ciprofloxacin, could be used in Type III fractures. To that end, they prospectively compared the use of ciprofloxacin to a regimen of cephalosporin plus gentamicin in 200 open fractures. Although patients in the ciprofloxacin group were over 4 times likely to develop infection in Type III fractures, this was not statistically significant, probably due to the small study group in the Type III fractures (26 patients in each group). Since both groups received gram-negative coverage, one cannot conclude that adding gram-negative coverage is necessary.
Thus, the addition of aminoglycosides for Type III fractures is not currently supported in the literature. This notion is supported by recent Consensus Guidelines issued by a military evidence-based medicine (EBM) review, also endorsed by Infectious Disease Society of America (IDSA) and the Surgical Infection Society (SIS) (8, 9). In contrast, despite the lack of evidence supporting the use of gram-negative coverage in Type III open fractures, the Eastern Association for the Surgery of Trauma (EAST) recommends it (10). Consequently, the lack of a uniformed guidelines leads to variability of care, as evidenced by a recent study showing that aminoglycosides are ultimately used at the discretion of the surgeon (9).
The use of penicillin has been advocated in heavily contaminated or farm wounds to prevent clostridium infection and is recommended by the East Practice Management Work Group (10). However, no hard data exist to support this recommendation (9), and Gustilo and Anderson (1) reported no cases of gas gangrene infection in their original study of over 1000 patients.
The duration of antibiotic therapy in open fractures has also been the subject of much debate. In a retrospective study evaluating open fracture-related infections, there were no infections in patients receiving antibiotics for 24 h, whereas fractures treated with longer duration of antibiotics (>3 days) had a statistically significant higher infection rate. However, this observations could be attributed to the type of open fracture, that is, worse injuries, which are more prone to infection, received a longer duration of antibiotics (2).
Dellinger et al. (11) reported a prospective randomized study evaluating the timing of administration of antibiotics and duration. For 240 patients, they found no relationship between the timing or duration of antibiotic treatment to infection. A similar infection rate was noted in patients receiving antibiotics for 24 h or greater than 24 h after admission. Nevertheless, the type of open fracture was related to infection. Most important, when evaluating by fracture type, the duration an antibiotics continued to be insignificant in predicting infection.
Recently, Al-Arabi et al. (12) confirmed these results in a prospective study evaluating timing of delivery of antibiotics. Patients assigned to six different groups based on the timing of their first dose of antibiotic (less than 2, 4, 6, 8, 12 h and greater than 12 h) demonstrated no correlation between timing of antibiotic administration and infection rate (12).
Other authors disputed that timing of delivery of antibiotics correlated with infection rate. Patzakis and Wilkins (13) reported a difference in infection rate in antibiotics delivered in less than 3 h (4.7%) and greater than 3 h (7.4%). However, they did not report whether this was statistically significant, did not control for fracture pattern, and this was a retrospective study on the data originally collected from their prior reports.
Our Practice
Given the above controversies and in line with the SIS guideline for use of antibiotics in open fractures (14), we believe that a first-generation cephalosporin (or clindamycin) should be administered upon arrival to the emergency room. Although there is no consensus on whether 24 h of antibiotics after each debridement prevents infection, it has been our current practice to administer 24 h of antibiotics after each debridement until wound closure or coverage (9).
The Utility of Cultures in Open Wounds
What is Agreed Upon?
Patzakis et al. (7) also evaluated the use of preoperative culture data of the wound. In agreement with other reports (1, 3), they found that less than 20% of initial cultures predicted the infecting organism and suggested that routine preoperative cultures should not be pursued. Indeed, organisms isolated from infected fractures are often not sensitive to the initial antibiotics (15), and many of the infecting organisms in severe open fracture are hospital acquired (16). In contrast, positive cultures at the time of closure did correlate with infection and may have clinical usefulness (15).
What is Controversial?
Although pre-debridement cultures are not recommended, post-debridement cultures may be useful. Positive cultures at the time of closure do not predict the infecting organism but correlate with the development of infection (15). Lenarz et al. (17) retrospectively reviewed their protocol of wound closure of open fractures based on culture data. According to this protocol, routine cultures were obtained after each debridement (n = 340 fractures). If the cultures were positive at 48 h, the patient received a repeat washout and new cultures. Wounds were closed or covered when the culture results from the previous washout were negative. The authors reported a low rate of infection for Type III fractures (6%) compared to historical controls (10%–50%).
Our Practice
We do not routinely take post-debridement cultures in open fractures. However, we perform this routine in delayed (>24 h) or infected injuries.
Timing to Debridement
The most heavily debated topic in the treatment of open fractures is the urgency in which open fractures should be debrided. In their original article, Gustilo and Anderson (1) concluded that “open fractures require emergency treatment …” Nevertheless, this statement is not supported by data and seems to represent his expert opinion only. In fact, emergent treatment is not supported in the current literature, and practice trends have been to perform urgent rather than emergent debridement of open fractures (18). A recent review of treatment of open fractures (19) concluded “neither emergent surgical intervention in the absence of physiologic stability, nor prolonged elective delay is supported by the available literature or otherwise warranted in the management of open fractures.” Furthermore, reviewing recent practice trends, Namdari et al. (18) found that approximately 40% of patients with open tibia fractures received debridement greater than 6 h from presentation and 25% of patients more than 24 h.
What is Agreed Upon?
The most important aspect of managing open fractures is the delivery of systemic antibiotics and performing an adequate debridement of nonviable tissue. As evident by Namdari et al.’s (18) work, many surgeons believe that an open fracture without vascular compromise is not an emergency. Some surgeons continue to treat open fractures immediately upon presentation. Thus, there is no absolute time which is agreed upon by all surgeons, by which open fractures should be debrided.
What is Controversial?
Emergent debridement of open fractures, within 6 h from injury, has propagated throughout the literature and became the standard of care for many years despite poor evidence supporting this practice. However, recent studies in open fracture management suggest that the timing of debridement may be of secondary importance compared with the delivery of antibiotics and aggressive debridement. Also, it seems that debridement should be performed within the first 24 h after injury once the patient has been adequately resuscitated (9).
The “6-hour rule” likely originated from a study in the 1890s (20) in which garden mold and dust were used as infecting agents in a guinea pig model of open fracture. In this experiment, the early phases of bacterial growth stopped after 6–8 h from injury, and it was more difficult to obtain a clean wound after 6–8 h of being contaminated. In addition, the main studies evaluating the association between timing of initial debridement and complications (i.e. infection) in open fractures are flawed by design. First, these studies compared the complication rate in fractures receiving operative debridement in less than or greater than 6 h from injury only, and no other time points were investigated. Second, because of the retrospective nature and/or inadequate data collection, the types of open fractures in each of these two study groups were unequal (11, 13, 21). This nonmatched distribution skews the results and conclusions of the above studies. For example, if more patients with a Type III open fracture were operated on earlier, the infection rate in the earlier group may have been higher. Conversely, if Type III fractures are debrided later rather than earlier, nonviable muscle may have declared itself and debridement would have been more aggressive. Third, many of the earlier studies were underpowered, and solid conclusions cannot be reached (22, 23).
As described above, the type of open fracture is predictive of infection (11, 24, 25). Thus, it is important to control for fracture patterns when attempting to determine the relationship between timing and infection, and a few studies were designed accordingly. The Lower Extremity Assessment Project (LEAP), originally constructed to assess the differences in outcome of patients with severe lower extremity injuries receiving amputation or limb salvage (26), served as a platform for several retrospective studies, which addressed the timing question. In a well-powered study, Pollak et al. (27) evaluated over 300 lower extremity Type III open fractures and reported a 27% infection rate and no relationship between timing of initial operative debridement and infection. They did find, however, that time from injury to arrival at the definitive trauma center was an independent risk factor for infection. Most recently, Schenker et al. (28) performed a systematic review of over 3500 open fractures and evaluated the relationship between timing of initial operative debridement and infection. The authors collected data from previously reported retrospective studies and controlled these cases for type of open fracture. This analysis did not identify a difference in infection rates between patients with open fractures receiving early (<6 h) or late (>6 h) debridement, and the authors concluded that the “6-hour rule” has little support in the literature.
Our Practice
Based on current data, there are no absolute recommendations regarding the optimal timing of open fracture debridements. However, it does appear that the “6-hour rule” is not valid. Thus, we recommend urgent debridement of open fractures, while the safety of waiting more than 24 h needs to be determined (9).
Timing of Wound Closure/Coverage
The optimal timing for closure of open fracture-associated wounds is debatable. Nevertheless, urgent debridement of open fractures with early soft tissue coverage is universally recommended.
What is Agreed Upon?
Type I and II open fracture wounds can be safely closed after initial thorough debridement, if there is no concern for ongoing muscle necrosis or contamination (29). There is agreement that patients with complicated open fractures be transferred to a specialized trauma center that is staffed with experts in fracture care and wound coverage (30, 31).
What is Controversial?
Controversy is focused on the optimal coverage or closure of Type III open fracture wounds. These wounds usually require a repeat debridement at 48–72 h after initial debridement. Although early wound coverage is recommended, the definition of “early” is vague. Coverage of an open wound associated with fractures should be performed only after all devitalized tissues have been removed. Early studies reporting increased infection rates with delayed coverage are flawed, as no control for injury severity or other risk factors was reported (32, 33). In addition, the groups with later coverage had worse soft tissue injuries, requiring more debridements and thus were inherently at a higher risk of infection.
More recent studies did control for fracture severity. Webb et al. (34) reported over 150 patients from the LEAP study group with Type III open tibia fractures. After controlling for fracture severity, they found that there was no difference in infection rate in those patients receiving early (<3 days) or late (>3 days) wound coverage. Pollak et al. (35) expanded the LEAP subgroup of patients and did not find any difference in infection rate when comparing wound coverage at less than 3, 4–7, or greater than 7 days. They did report, however, a 32% complication rate in those wounds covered at greater than 7 days. More recently, D’Alleyrand et al. (36) reported no difference in wound complications in those covered in less than 7 days, but every day afterward, complication rate increased 15% per day.
Our Practice
We recommend closure within 7 days of wounds associated with open fractures once the soft tissues have stabilized, and all nonviable tissues have been removed (9).
Future Directions: The Use of Negative Pressure Wound Therapy
The use of negative pressure wound therapy (NPWT) has become increasingly popular in the soft tissue management of open fractures. It increases blood flow to the wound bed (37), decreases the wound surface area needed for coverage (38), and has been shown to decrease infection rates in open fracture wound management (39).
In a prospective, randomized study, Stannard et al. (39) examined infection rate in 62 patients with open fractures who received initial soft tissue management with either NPWT or a gauze dressing. They found a significantly decreased infection rate (28% vs. 5.4%; p = 0.02) in favor of the NPWT. More recently, Blum et al. (40) reported similar results (20% infection in the standard dressing group and 8% in the NPWT group). As expected, the open fracture type correlated with infection rate. We routinely use and support NPWT in the initial management of open fractures.
Footnotes
Declaration of Conflicting Interests
The authors do not have any conflict of interest in relation to this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.