
Abstract
Elemental mercury impaction in the appendix can cause subsequent local and systemic complications. We present a case of a teenage boy who ingested approximately 10 mL of elemental mercury, resulting in residual mercury sequestration in the appendix after conservative management. We performed laparoscopic appendectomy to remove the residual mercury. The patient made a complete clinical recovery without adverse events related to mercury poisoning over the 6-month follow-up. We highlight the advantages of laparoscopic appendectomy, abdominal computed tomography (CT), negative pressure operating rooms, and surgeon protection to improve surgical success rates. This case report adds to the literature on the management of elemental mercury impaction in the appendix and provides valuable insights for clinical decision-making.
Keywords
Introduction
Mercury is a toxic heavy metal that is widely distributed in nature and exists in various forms, including elemental mercury, inorganic salts, and organic compounds. Although exposure to mercury can be toxic, elemental mercury is rarely absorbed after acute ingestion, and is considered non-toxic and excretable within a few days. 1 However, residual mercury in the body is harmful. In particular, elemental mercury that remains in the appendix can cause appendicitis and subsequent local complications.1–3 Inorganic or organic compounds transformed from elemental mercury could result in chronic toxic effects, such as toxic nephropathy or neurotoxicity, that can persist for decades.4–6 Therefore, residual elemental mercury in the body requires immediate attention, even after active conservative treatments.
Traditionally, residual elemental mercury in the appendix has been removed surgically, such as endoscopically or with prophylactic appendectomy. However, these surgeries carry the risk of mercury leakage into the abdominal cavity. 1 Additionally, the surgical team must have extensive experience, and few reports describe the surgical procedure for mercury sequestration in the appendix.3,7 Here, we report a case of elemental mercury sequestration in the appendix that was successfully managed using laparoscopic appendectomy. We describe the operative techniques, which may help improve the surgical success rate.
Case report
A teenage boy presented to our outpatient department after ingesting an estimated 10 mL of mercury and barium sulfate. He was taken to a local emergency department within 2 hours of ingestion. On admission, his initial vital signs were unremarkable; none of the following were present: elevated heart rate, elevated respiratory rate, elevated blood pressure, elevated body temperature, nausea, abdominal pain, or diarrhea. He was treated with conservative management, namely gastrointestinal decompression, laxatives, and gastric lavage, with care to avoid inhalation of mercury and subsequent toxicity.2,8 These treatments resulted in the discharge of most of the mercury from his body. After this treatment, he showed no apparent abdominal pain, nausea, vomiting, dizziness, or limb numbness. However, abdominal computed tomography (CT) revealed a high-density shadow in the appendix (Figure 1a), indicating possible residual mercury sequestration. He was then transferred to our hospital for further treatment. Examination on admission revealed the following: body temperature: 36.6°C, pulse: 88 beats per minute, respiratory rate: 20 breaths per minute, and blood pressure: 138/82 mmHg, with no particular discomfort. Blood tests revealed the following: alanine aminotransferase concentration: 76 U/L and aspartate transaminase concentration: 109 U/L. Blood routine and coagulation test results were within normal limits, and electrocardiography and chest CT findings were normal. Because the mercury had been retained in the patient’s body for 24 days, the residual mercury sequestration in the appendix was difficult to excrete.

Abdominal radiographs showing the comparison of residual mercury in the appendix before (a) and after (b) the surgery.
With the patient’s and his family’s consent, we performed laparoscopic appendectomy to remove the residual mercury in the appendix (Figure 1b). Intraoperatively, we established pneumoperitoneum during laparoscopy and found that the distal appendix was significantly thickened and filled with blood and edema. To prevent mercury flowing back into the intestine, we clamped the appendix with separation forceps 1 cm from the root of the appendix followed by double-locking Hem-o-Lok clips (WD-JZ 4L; Wedu, Zhejing, China), to close to the root of the appendix. We then treated the mesenteric appendix and clipped the distal end of the appendix with a Hem-o-Loc clip (Wedu) to avoid mercury flow into the abdominal cavity. Importantly, before removing the appendix, we applied suction to retrieve the severed part, with continuous negative pressure to prevent mercury outflow. We successfully removed the appendix, and routine operation continued. There was no mercury outflow. Postoperatively, we dissected the appendix in water. The mercury scattered in the water and was collected and sealed before further processing (Figure 2). In this case, we took strict measures to prevent the inhalation of toxic mercury vapor.
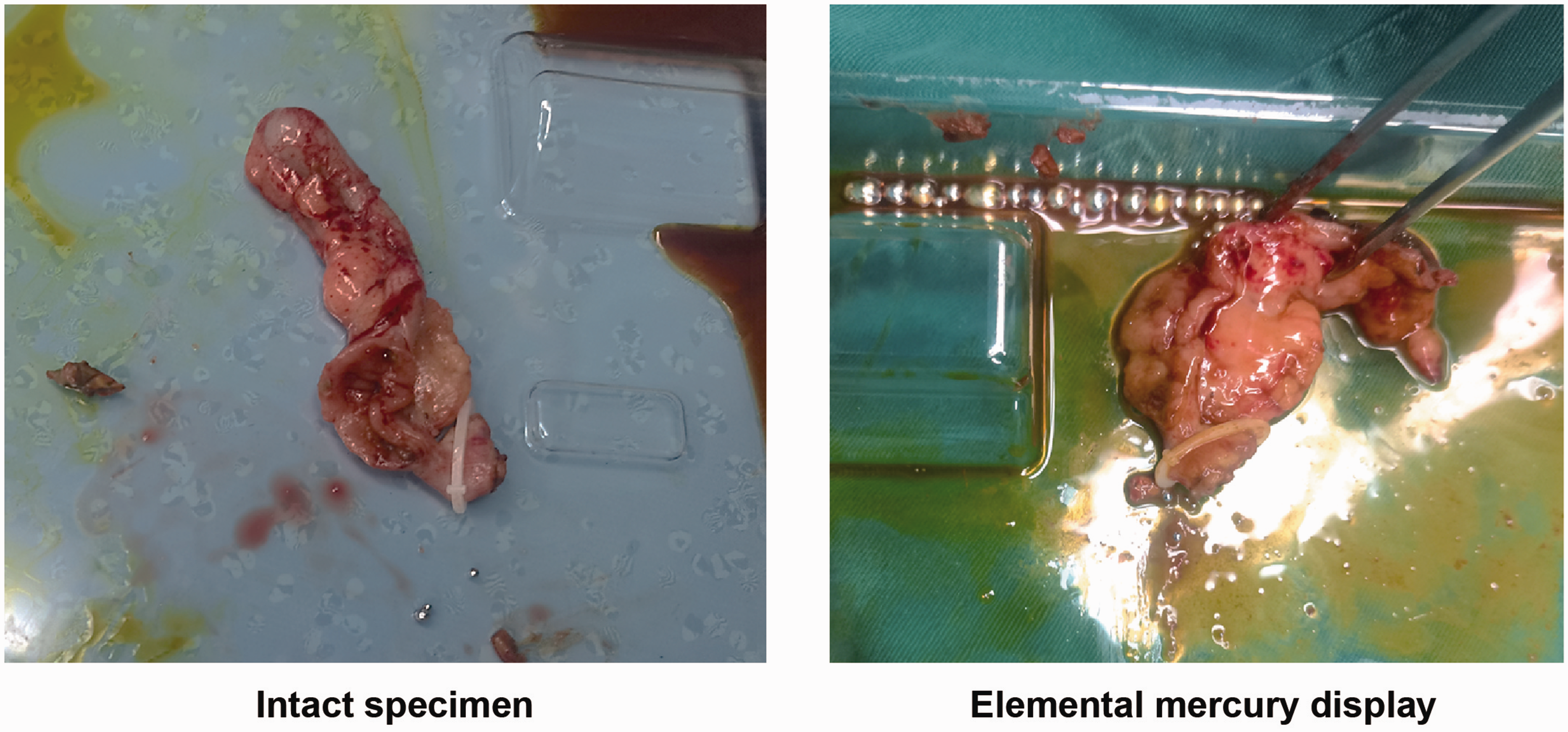
The appendix specimen after laparoscopic appendectomy.
The operation was successful, and the patient’s postoperative recovery was uneventful. After 4 days of postoperative observation, he showed no symptoms of discomfort. He made a complete clinical recovery and showed no adverse effects related to mercury poisoning over a 6-month follow-up.
This case report was approved by the Ethics Committee of Dongzhimen Hospital (approval no. 2023DZMEC-006-01). The patient provide written informed consent for publication of this report. The reporting of this study conforms to the CARE guidelines. 9
Discussion
The toxic effects of mercury are slow in onset but severe. Mercury may impair organs or subcellular structure function. Mercury collects in various organs by changing the tertiary and quaternary structure of proteins, and sulfhydryl and selenium group binding, causing toxicity and abnormal cell function. 10 Although elemental mercury is rarely absorbed (up to 0.01%) in the gastrointestinal tract, it can easily pass the blood–brain barrier and impair the nervous system.11,12 Furthermore, if acutely-ingested elemental mercury cannot be excreted from the body, the residual mercury can be transformed into organic or inorganic mercury by bacteria or other microorganisms, and in particular, become sequestered in the appendix. 13 Elemental mercury sequestration in the appendix may cause local complications, such as acute appendicitis or perforation, which is considered the third most common sequela of appendicitis. 3 However, in our literature review, we found few studies describing the active management of elemental mercury retained in the appendix.1,8
Notably, in our experience with this case, we found that laparoscopic management of elemental mercury sequestration in the appendix has several advantages over open surgery: 1) Laparoscopic surgery is minimally invasive, which means that it involves smaller incisions and less tissue damage compared with open surgery. This can result in less pain, shorter hospital stay, and faster recovery time for the patient; 2) Laparoscopic surgery provides better visualization of the surgical field, 14 which can help the surgeon identify and remove all of the mercury-contaminated tissue more effectively. This can reduce the risk of leaving mercury behind, which could lead to further complications; and 3) Laparoscopic surgery is associated with a lower risk of infection and other postoperative complications, such as bleeding and hernia formation. 15 This is because the smaller incisions used in laparoscopic surgery result in less tissue trauma and a reduced risk of wound infection. The patient in this case was young, and laparoscopic surgery is associated with better cosmetic outcomes, as the smaller incisions result in less scarring compared with open surgery. 16 On the basis of these findings, we highly recommend laparoscopic appendectomy to remove retained mercury in similar cases. 3
For several reasons, we performed abdominal CT in this case rather than abdominal ultrasonography to identify mercury impaction in the appendix. First, abdominal CT has a larger observation range than that of ultrasonography; therefore, CT provides a more comprehensive view of the abdominal area. 17 This is particularly important in cases where the mercury impaction is not limited to the appendix and may have spread to other areas. Second, with large amounts of intestinal gas, ultrasonography may be unsatisfactory, as gas can interfere with the ultrasound waves and make it difficult to obtain clear images. CT is not affected by intestinal gas and can provide clear images even in the presence of gas. Third, compared with ultrasonography, CT provides a more accurate understanding of the dispersed location of mercury in the appendix, which can help surgeons plan the surgical approach more effectively. CT can also determine whether there is leakage or perforation around the appendix, which is important for determining the appropriate surgical intervention. Overall, compared with ultrasonography, abdominal CT can identify mercury impaction in the appendix; provides a larger observation range, clear images even in the presence of intestinal gas, more accurate understanding of the location and extent of the mercury contamination; and can be used to assess the overall extent of the contamination. CT can also be used to determine whether there is residual mercury in other areas, which is important for assessing the overall extent of the mercury contamination and planning appropriate treatment.
Nevertheless, as surgery is associated with potential complications risks, we describe the points in our successful approach in laparoscopic appendectomy. To achieve a very low rate of complications, we implement the following strict measures:
A negative pressure operating room is necessary in cases where there is a risk of airborne contamination. Mercury vapor can be released during surgical manipulation of the contaminated tissue, and this vapor can pose a risk to the health of the surgical team and others in the operating room. However, while a negative pressure operating room is an effective measure for preventing the spread of airborne contaminants, it can be costly to implement and maintain. The cost-effectiveness of this measure should be considered carefully, given the potential risks and benefits, while ensuring the occupational safety of the surgical personnel. In the case of mercury impaction in the appendix, cautery can be used to minimize the release of mercury vapor by sealing the contaminated tissue and preventing the spread of mercury to other areas of the body. Surgeons must increase protective measures, including the use of protective equipment, such as gloves, masks, and goggles, to prevent direct contact with the contaminated tissue and inhalation of mercury vapor. We use a suction device to retrieve the severed part of the appendix using continuous negative pressure, when the appendix is removed. Additionally and importantly, the removed appendix should be dissected in water to avoid further mercury evaporation in the operation room.
In the case of laparoscopic appendectomy for elemental mercury sequestration, we recommend using a negative pressure operating room to minimize the risk of exposure to mercury vapor. However, the decision to use a negative pressure operating room should be made by a thorough assessment of the risks and benefits of this approach, as well as the specific circumstances of the surgery and the patient’s condition. Moreover, if a negative pressure operating room is not available, we recommend spraying adsorbents or chelating agents to address the mercury vapor in the environment postoperatively. Alternatively, we recommend a sealed bag to remove the specimen and dissecting and inspecting the specimen in a sealed operating box. Hence, the decision to use a negative pressure operating room should be made on a case-by-case basis.
Regarding the management strategy in cases of mercury spillage into the abdomen, this situation can be difficult if not managed properly. First, if mercury accidentally spills into the abdominal cavity, the patient should be placed in the supine or right lateral position, and the spilled mercury should be promptly removed by suction. Second, the patient’s head should be elevated to use gravity to retain the mercury in the right lower abdomen or pelvic area, with the mercury promptly removed by suction. Third, chelating agents can also be used for treatment, followed by lavage and suction.
This case report adds to the literature on the management of elemental mercury impaction in the appendix and provides valuable insights for clinical decision-making.
Footnotes
Author contributions
Guibin Yao was a surgeon in this case and drafted the manuscript. Ping Zhang collected the data. Jianyu Cao was a surgeon in this case, and Xia Hu was the resident physician during the follow-up. Yan Tan drafted and edited the manuscript. Chengli Yao was a surgeon in this case and conceived the study.
Data availability statement
The data used to support the findings of this study are included within the article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Special Project of Health Development and Scientific Research in the Tongzhou District of Beijing [Project no. TFZXPT-20180116] and the Science and Technology Plan of the Tongzhou District of Beijing [Project no. KJ2020CX013].