
Abstract
Background and Aims:
The aim of this study was to compare the feasibility and early postoperative outcomes between patients undergoing double-barreled wet colostomy and patients undergoing terminal colostomy and ileal conduit for simultaneous urinary and fecal diversion.
Material and Methods:
Between 1995 and 2012, we had 181 patients in whom it was necessary to make simultaneous urinary and fecal diversion. This is a retrospective study and patients were divided into two groups, depending on the technique applied for the fecal and urinary diversion. The first group consisted of patients undergoing ileal conduit and terminal colostomy and the second group consisted of patients undergoing double-barreled wet colostomy.
Results:
Ileal conduit and terminal colostomy was performed in 77 (43%) cases, while wet colostomy was performed in 104 (57%) cases. Median length of stay was shorter for double-barreled wet colostomy (13.1 vs 18.1, p < 0.0001). Median operating times for urinary and fecal diversion were shorter for double-barreled wet colostomy (32 vs 64 min, p < 0.0001). The morbidity was lower for double-barreled wet colostomy (11.5% vs 23.4%, p = 0.0432), retrospectively. The mortality was 3.8% for double-barreled wet colostomy and 10.3% for ileal conduit and terminal colostomy group (p = 0.1282).
Conclusions:
Double-barreled wet colostomy is a safe, fast, and simple alternative to traditional ileal conduit and terminal colostomy diversion. The technique is relatively easy to learn, and it reduces the time for urinary and fecal diversion, length of stay, and morbidity rate.
Introduction
In patients who had undergone total pelvic exenteration, have had complications related to radiation therapy (usually after radiotherapy for cervical cancer), and in patients with inoperable pelvic tumors, it is necessary to make fecal and urinary diversion (1). Fecal diversion does not offer much choice, as either colostomy or ileostomy (when colostomy is not possible) is performed. In contrast, there are several types of urinary diversion: incontinent (including ileal conduit (IC) wet colostomy) and continent (Indiana pouch, Kouch pouch, Florida pouch, Miami pouch) (2).
Reconstructive phase (urinary diversion, filling of the pelvic dead space, and, in female patients, reconstruction of the vagina) is the very important step in pelvic exenterative surgery and significantly contributes to increased surgical morbidity and mortality (3). Alexander Brunschwig (4), the pioneer of exenterative and pelvic surgery, performed the original wet colostomy in 1948, with implantation of ureters proximally to fecal output so that the stool and urine mixed before exiting. This type of ostomy was accompanied by numerous complications, including ascending pyelonephritis (major complication), electrolyte dysbalance, and unpleasant odor, which led to its abandonment from surgical practice (5).
In 1950, Bricker constructed the IC considered to be an excellent solution at the time (still often used today) and a major step forward in exenterative pelvic surgery (6). The reasons against performing this procedure are the need to perform two stomas, prolonged surgical procedure, and the performance of anastomosis with an increased risk of dehiscence in previously irradiated intestines and in malnourished patients.
In 1989, MF Carter (7) was the first to describe three patients in whom a common urinary and fecal diversion was necessary and where double-barreled wet colostomy (DBWC) was performed. This was followed by a report of 11 additional patients in 1994 (8). The procedure involves performing bipolar colostomy, with the section and sutured closure of the distal end of the colon at about 10–15 cm distal to the stoma, and implantation of ureters into the formed colon conduit. After the intervention, a urine reservoir, which is formed distal to the stoma, empties out freely without fecal contact. The advantages of this new method include existence of one stoma instead of two, avoidance of the anastomosis in over-irradiated bowel, shortening operating room (OR) time, and a better quality of life.
This study was retrospective and included a comparison of two surgical techniques used to perform fecal and urinary diversion, namely, DBWC and IC with terminal colostomy (IC + TC). Objective of this study is to show that the DBWC is safe, technically feasible, cheaper, and faster alternative to IC + TC method.
Materials and Methods
After Institutional Ethical Review Board approval, the nature of the procedure for fecal and urinary diversion was explained to all candidates in detail, as well as the necessity to create two stomas (IC + TC group), as a standard procedure. Since 2003, alternative solution was offered, to create just one stoma (DBWC group), and most patients accepted it. The reported data include patient demographic information such as gender, age, tumor type, and previous radiation therapy. Surgical course and early postsurgical outcomes were recorded for each patient (general complications, urinary and fecal diversion–related complications, late complications, OR time for urinary and fecal diversion, and hospital length of stay (LOS)). In addition, the results of long-term postsurgical monitoring were recorded.
Statistical analysis was performed using the SPSS 17.0 statistics package. Chi-square test, Fisher’s exact test, and student t-test were applied to compare the groups.
Wet colostomy—surgical technique
Wet colostomy requires mobilization of the left colon and splenic flexure. After the large bowel mobilization, bilateral identification and mobilization of the ureters should be performed, with a distal section below the promontorium. Sigmoid colon is then sectioned and its ends closed using the gastrointestinal anastomosis (GIA) stapler. The resection line is then reinforced using interrupted polygalactin 3/0 sutures to prevent distal stump leakage. In patients with TC, the colostomy is first mobilized, followed by performing the wet colostomy.
Ureters are implanted into the colonic pouch at antimesenteric tenia of the distal stump and sutured with interrupted polygalactin sutures (refluxing anastomosis) 4/0 sutures (Fig. 1) To avoid complications such as hyperchloremic and hypocalcemic acidosis, it is important to make a short distal reservoir (10 to 15 cm) which, when associated with mass colonic contraction movements, tends to decrease stasis and residual urine.
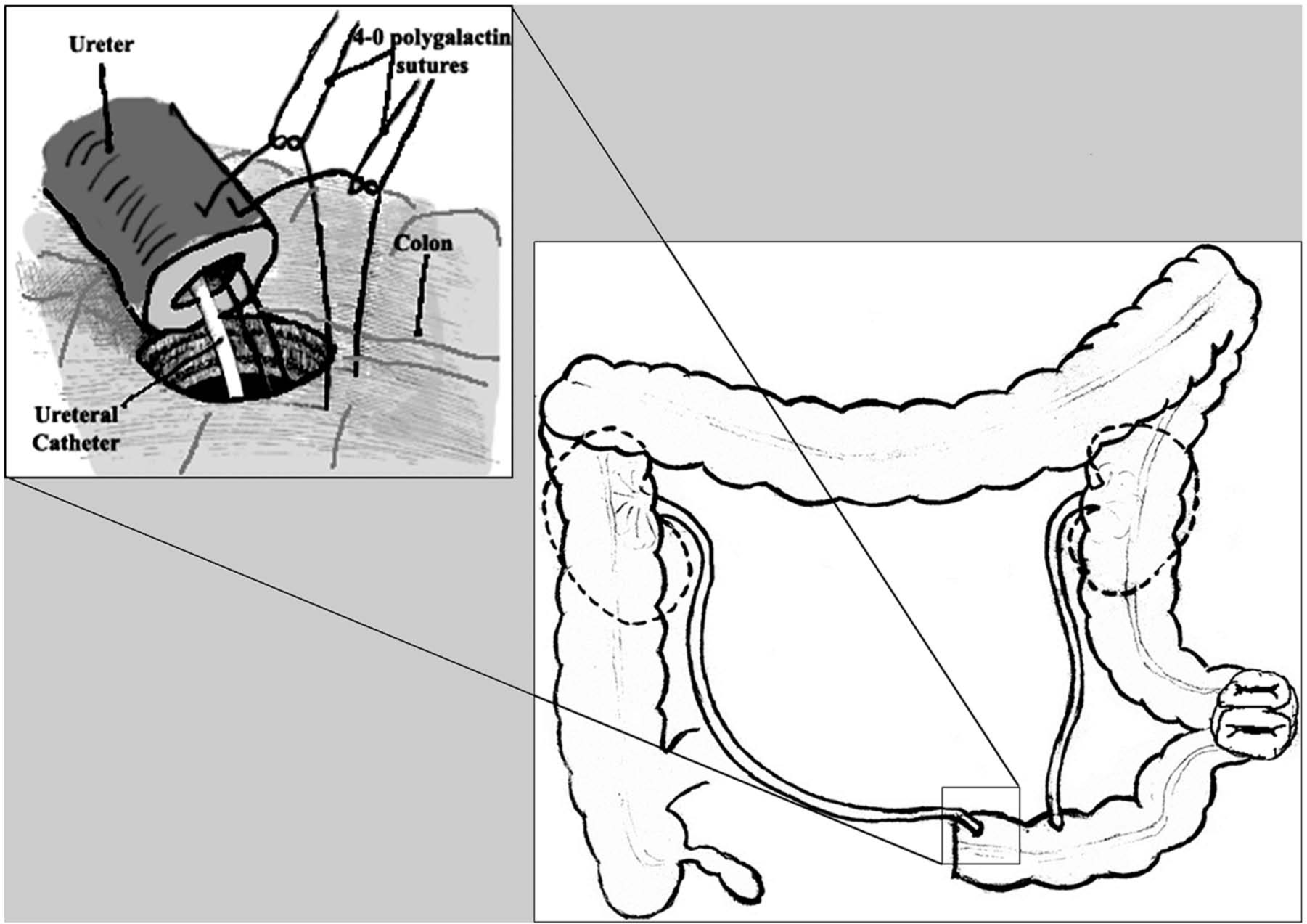
Wet colostomy and uretero-colonic refluxing anastomosis.
It is necessary to establish adequate urine output during surgery and postoperatively—verification of uretero-colonic anastomosis continuous flow to prevent ureteral stent clogging. Two ureteral catheters (RÜSCH® Standard Cylindrical Straight tip, 1 eye ureter catheter) are placed through the anastomosis into the ureters for a duration of 4 weeks. Colonic reservoir should be additionally fixed to the retroperitoneal promontorium (9).
Results
Between 1995 and 2012, a total of 181 (104 with DBWC and 77 with IC + TC) patients underwent surgery, requiring urinary and fecal diversion. In our study, the most common indications for urinary and fecal diversion in IC + TC group were 21 (27%) recurrent rectal adenocarcinoma, 20 (26%) primary rectal adenocarcinoma, 10 (13%) for palliation, and 3 (4%) after postradiation damage. In DBWC group, the most common indications for urinary and fecal diversion in IC + TC group were recurrent cervical cancer 23 (22%), primary rectal adenocarcinoma 18 (17%), 12 (12%) for palliation, 17 (16%) and after postradiation damage (Table 1).
Indications for urinary and fecal diversion.
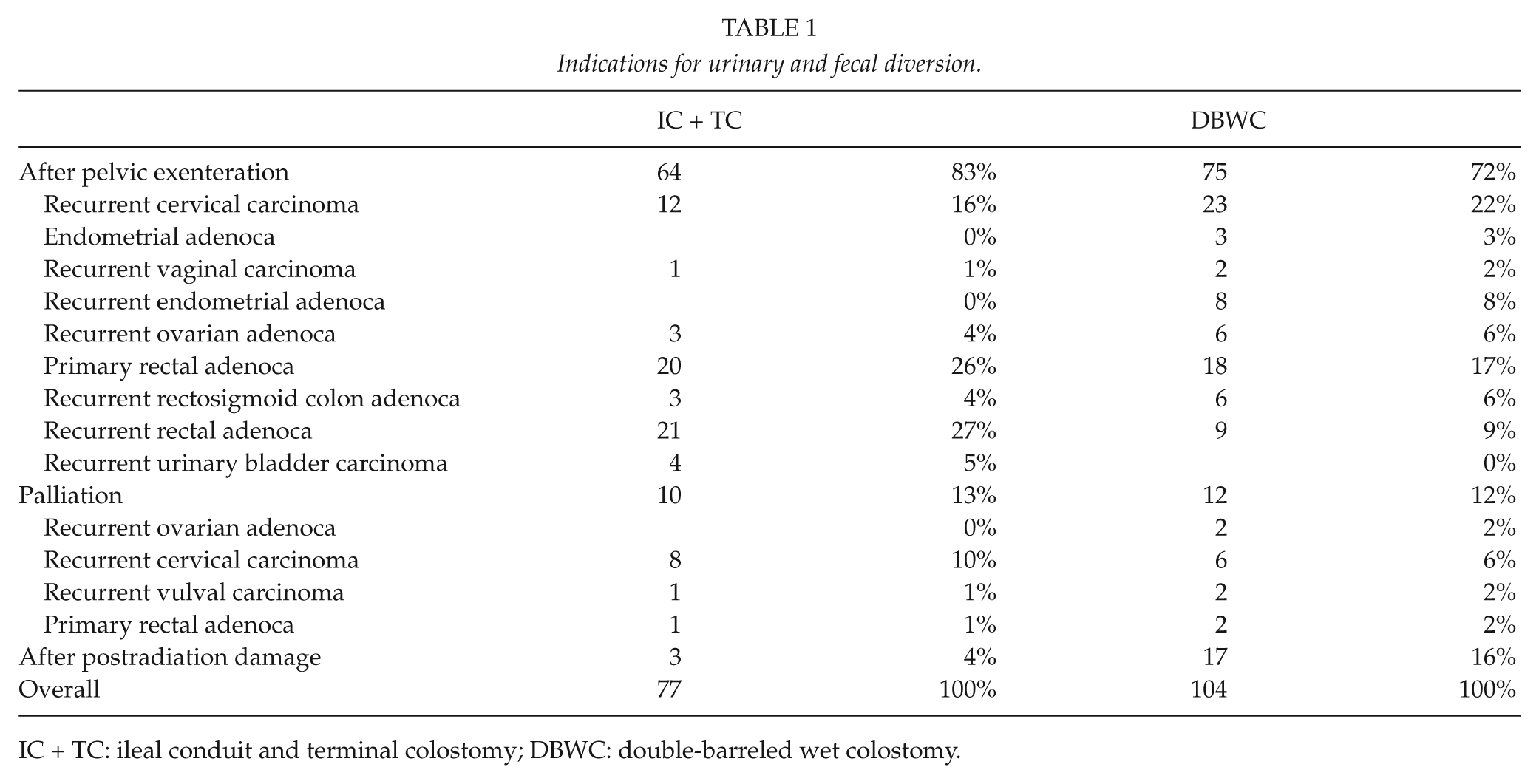
IC + TC: ileal conduit and terminal colostomy; DBWC: double-barreled wet colostomy.
In the DBWC group, 45/104 patients received full dose pelvic radiation, without brachytherapy or intraoperative radiation, and in the IC + TC group, 12/77 patients received full radiotherapy without brachytherapy or intraoperative radiation.
IC and TC were performed in 77 (43%) cases, while wet colostomy was performed in 104 (57%) cases. Median age was 54.5 (23–77) years in DBWC group and 55.4 (24–78) years in IC + TC group (p = 0.5924). There were 27 males and 77 females in the DBWC group and 35 males and 42 females in the IC + TC group (p = 0.0073). The DBWC group had more patients who received radiotherapy (45/104) than in the IC + TC group (12/77) (p = 0.0001).
Median LOS was shorter for DBWC (13.1 vs 18.1, p < 0.0001). Median operating times for urinary and fecal diversion (only for diversion, not for whole operation) were shorter for DBWC (32 vs 64 min, p < 0.0001).
The morbidity was lower for DBWC than in IC + TC group (12/104 (11.5%) vs 18/7723 (4%), p = 0.0432), retrospectively. The two groups were similar in terms of urinary and fecal diversion–related morbidity and late complications. Patients (in both groups) with general complications like postoperative prolonged intestinal paresis, central venous catheter infection, thrombocytopenia and anemia, pulmonary embolism, wound infection/dehiscence, and deep vein thrombosis were treated conservatively. Patients with pyelonephritis were treated conservatively, and patients with urinary leaks were managed with percutaneous nephrostomy (PCN) tubes. All patients (in both groups) with enteric fistula required reoperation. One patient in the DBWC group and two patients in the IC + TC group had stenosis of the uretero-colonic anastomosis, which was resolved by catheterization. In the patient who had conduit necrosis, 2 months after surgery, we performed resection of the large bowel with new wet colostomy.
Mortality was 3.8% for DBWC and 10.3% for IC + TC group (p = 0.1282). In the DBWC group, one patient died due to conduit necrosis, one due to enteric fistula, one due to pulmonary embolism, and one due to deep vein thrombosis. In the IC + TC group, five patients died due to enteric fistula, two due to urinary leaks, and one due to pyelonephritis (Table 2).
Demographic characteristics and outcomes.
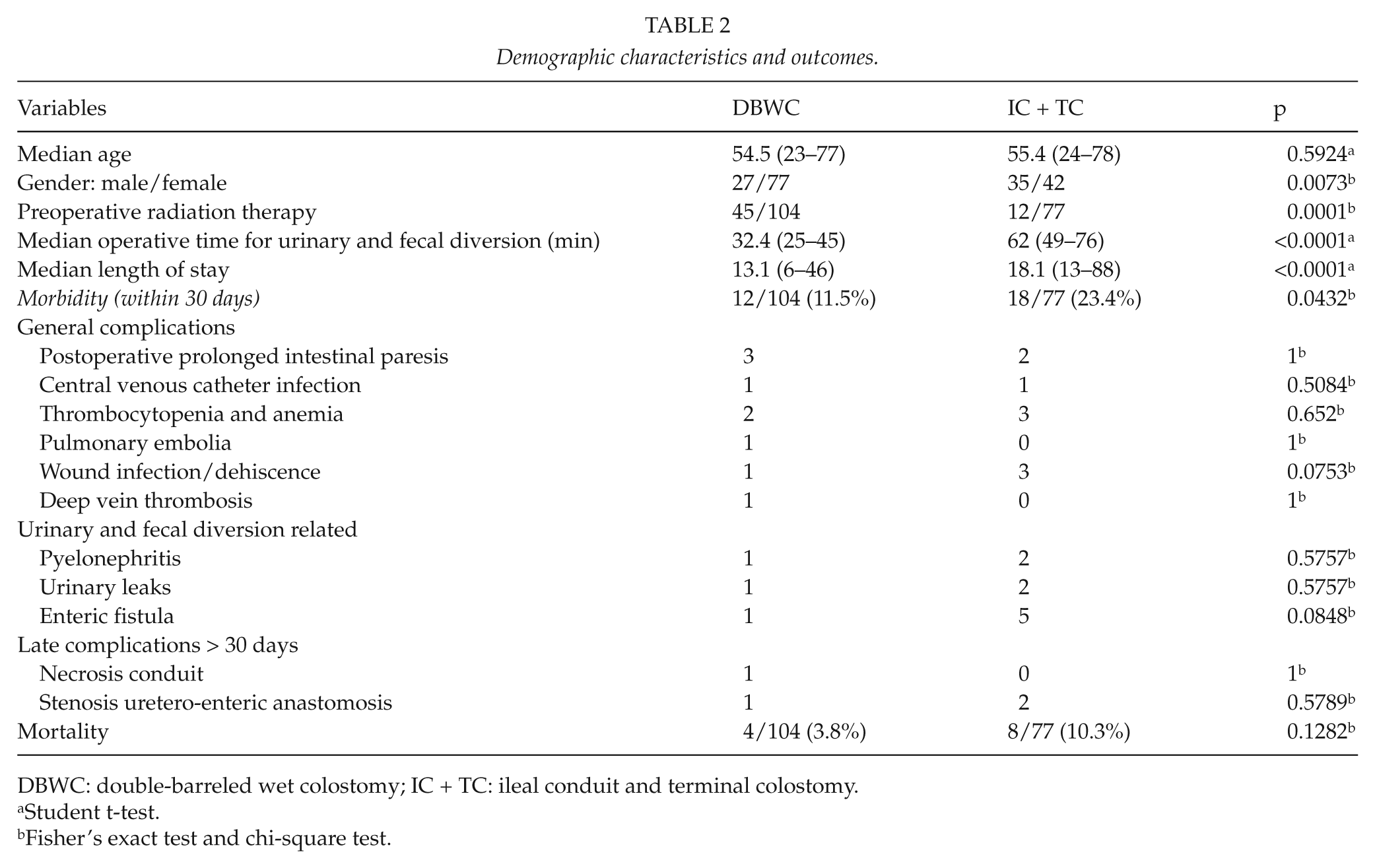
DBWC: double-barreled wet colostomy; IC + TC: ileal conduit and terminal colostomy.
Student t-test.
Fisher’s exact test and chi-square test.
For the first 2 years, patient follow-up visit was performed every 3 months, every 6 months for the next 2 years, and just once a year afterward. During site visits, results of abdominal ultrasound, urea, creatinine, and calcium were obtained. Results showed no changes in electrolyte status.
Discussion
The most common indications for performing fecal and urinary diversion are cervical cancer (about 70%, usually relapse after radiation therapy) and primary and advanced recurrent rectal carcinoma (about 10%, where preoperative radiotherapy is the standard of care), and thus the intestines used for the diversion are commonly irradiated and very often over-irradiated (10).
Review of the literature revealed two studies that compared these two methods, but only after pelvic exenteration (11, 12). In contrast, our study investigated fecal and urinary diversion after total pelvic exenteration, in palliation of inoperable pelvic tumors, and in resolving enterovesicovaginal fistulae following radiation therapy. Our study is limited because of its retrospective nature, group diversity, especially by cause.
The first reason to favor the DBWC is faster performance, because in patients with IC and TC, it is necessary to establish a TC followed by resection of a portion of terminal ileum, formation of urostomy, and enteral anastomosis. Median operating times in our study for urinary and fecal diversion (only for diversion, not for whole operation) were shorter for DBWC (32 vs 64 min, p < 0.0001).
This type of surgery can be safely performed on non-irradiated intestine because the splenic flexure is always mobilized, and the colon prep is cut and sutured closed between descending and sigmoid colon, an area which is very rarely irradiated. In contrast, with the IC, there is no choice but to resect the terminal ileum and create the IC from this part of intestine. Although, according to recent data, survival of female patients with cervical carcinoma is significantly prolonged, incidence of late gastrointestinal (GI) complications is increased. Rectum is an organ with greatest chance of being over-irradiated, causing proctitis in 5%−11% female patients (13), while complications with sigmoid colon are much more rare (0.6%−6.4%) (14, 15). Radiation complications with descending colon, used for forming of DBWC, are described as very rare. In the DBWC group, there were more patients who received radiotherapy (45/104) than in the IC + TC group (12/77) (p = 0.0001). In the DBWC group, we have fewer complications than in the IC + TC group (p = 0.0432). In our study, we found that enteral fistula occurred in one patient in DBWC group and in five patients in the IC + TC group, which is in accordance with Backes et al.’s (12) study (they found enteral fistula only in two patients in the IC + TC group). Chokshi et al. (11) found that enteral fistula occurred in 13 patients in DBWC group and in 1 patient in IC + TC group.
Patients who are candidates for this type of surgery are almost always very exhausted and cachectic (enterovesicovaginal fistulae complicated by chronic pelvic infections, difficulty in defecation due to the tumor mass, obstructive nephropathy, and so on), and thus benefit from less invasive surgery (16).
Quality of life is important when considering existence of two stomas instead of one. After all, Carter’s idea for the modified wet colostomy came after a patient, who had undergone abdominoperineal resection by Miles, refused the second stoma. None of the patients in our study accepted two stomas if they were offered an alternative of one stoma. Patients use ileostomy bags with air filter, and urine draining of full bag is done by simple opening of the clamp. When it is full of feces, the bag is replaced.
There is a significant financial impact due to the reduction in OR time for urinary and fecal diversion, postsurgical recovery time, and costs related to stoma bags and disks, as one set is used compared to two required in TC and IC.
The reasons against performing DBWC, outlined by some authors, include the possibility of urinary infection, the potential for stenosis during long-term monitoring, and the possibility of colon cancer at the part of colon containing the pouch (described in one case, but the de novo occurrence could not be excluded) (17).
We made non-reflux anastomosis even if there is an assumption that this type of anastomoses are predicted to create stenosis. Studer et al. (18) showed that stenosis was found in 13.5% of patients with anti-reflux uretero-ileal anastomosis and only in 3% of patients with non-anti-reflux anastomosis. Pantuck et al. (19), after 41 months of follow-up, found presence of uretero-ileal anastomosis in 13% of patients with anti-reflux anastomosis and only 1.7% with usual end-to-side non-anti-reflux anastomosis.
Many urologists believe that unnecessary additional mobilization of the left ureter (while forming of IC) and the setting above mesenteric sigmoid colon can lead to ischemic anastomotic structures of uretero-enteric anastomosis that may be resistant to endoscopic or open repair of anastomosis (20, 21). Some clinical studies have shown a higher percentage of uretero-enteric stenosis on the left side compared to the right side, and also a smaller percentage of successful interventions while dealing with stenosis of the left side (22, 23). In our study, we had two ureteral stenosis to the left side in the IC + TC group, while in the DBWC group we had one stenosis of the uretero-enteric anastomosis on the right side (1/104, 0.9%), which is consistent with clinical studies of Guimaraes et al. (1), who showed the existence of one uretero-colonic anastomosis, and also studies by Golda et al. (24), which also had one stenosis of uretero-colonic anastomosis. In accordance with the results of other clinical studies (8, 25, 26) we did not diagnose the existence of hydro-electrolyte disorders.
Few clinical studies have evaluated this approach (DBWC) and there is lack of long-term monitoring data (1, 26). Urologists generally agree that this type of urinary diversion is appropriate in critically ill patients with short life expectancy, as late outcomes are uncertain (17).
In conclusion, DBWC is a safe, fast, and simple alternative to traditional IC and TC diversion. It reduces the time for urinary and fecal diversion, LOS mortality, and morbidity rate. DBWC is associated with good late outcomes, as the functional results are similar with IC + TC, and there is no statistically significant difference in the rate of stenosis of the uretero-intestinal anastomosis, obstructive nephropathy, and the formation of calculi in the conduit.
Footnotes
Declaration of Conflicting Interests
All the authors hereby declare that they have no conflicts of interest to disclose.
Funding
This study was supported by the grant from the Serbian Ministry of Science (Project No. 41033).