
Abstract
Background and Aims:
Atrial fibrillation is a common arrhythmia after cardiac surgery. It increases morbidity, length of hospital stay, and costs of operative treatment. Beta-blockers, sotalol, amiodarone, corticosteroids, and biatrial pacing have been shown to be efficient in the prevention of postoperative atrial fibrillation. The aim of this study was to find out how widely different prophylactic strategies for postoperative atrial fibrillation are used in Scandinavian countries.
Material and Methods:
An online link for a questionnaire was emailed to (214) cardiac surgeons in Finland, Sweden, Norway, Denmark, and Estonia to assess the use of prophylactic methods for postoperative atrial fibrillation.
Results:
A total of 97 surgeons responded to the survey. Oral beta-blockers were routinely used for atrial fibrillation prophylaxis by 62% of responders. The main reasons for nonuse of beta-blockers were that responders were unconvinced of the evidence of benefit or they preferred some alternative prophylaxis. Intravenous beta-blockers were used frequently by 6% of responders. Amiodarone was used for prophylaxis by 18% of responders. Nonusers were unconvinced of its efficacy, were afraid of its complications, or found its use too cumbersome. Other prophylactic atrial fibrillation strategies that were used are as follows: sotalol by 2%, magnesium by 17%, corticosteroids by 1%, and atrial pacing by 11% of respondents.
Conclusions:
There is still widely varying implementation of strategies for atrial fibrillation prophylaxis among Scandinavian cardiac surgeons. Lack of confidence in the efficacy of these approaches is the main rationale for nonimplementation.
Introduction
Atrial fibrillation (AF) is the most common arrhythmia to occur after cardiac surgery. In general, in studies involving large numbers of patients, the reported incidence is around 30% (1–4). These results vary depending on the definition of AF used and the type of postoperative monitoring employed to detect it.
AF after cardiac surgery is associated not only with increased morbidity and mortality but also with additional treatment and thus increased perioperative cost (1, 5–8). As postoperative AF has been shown to be an independent predictor for postoperative stroke (9–11), long-term morbidity is also a key consequence of this complication.
Numerous studies have assessed the value of prophylactic strategies for postoperative AF. The efficacy of beta-blockers (12, 13), sotalol (12, 13), amiodarone (12–14), magnesium (15, 16), corticosteroids (17, 18), and biatrial pacing (12, 13) has been shown in many well-conducted randomized controlled trials (RCTs). Furthermore, meta-analyses addressing this question have shown that the preventive strategies of postoperative AF reduce the risk of stroke and the length of hospital stay (12, 13, 19). On this basis, current guidelines recommend the use of prophylactic medication, especially beta-blockers, for the prevention of AF after cardiac surgery (20, 21).
A recent online survey was reported about the use of prophylactic strategies for postoperative AF among Canadian cardiac surgeons. Less than 60% of surgeons used beta-blockers routinely for the prevention of postoperative AF. They concluded that the use of AF prophylaxis remained less than expected (22). The aim of this study was to assess how widely different prophylactic strategies are used in the prevention of AF after cardiac surgery in Scandinavian countries.
Material and Methods
An electronic questionnaire was developed to assess the use of different preventive methods of postoperative AF after cardiac surgery among adult cardiac surgeons in Scandinavian countries. The questionnaire consisted of 37 questions concerning current prophylaxis of the postoperative AF (type and frequency) and demographics. Rationale for use or nonuse for each of the strategies was also requested.
The questionnaire was sent to cardiac surgeons working in Finland, Sweden, Norway, Denmark, and Estonia. The surgeons were identified from the Cardiothoracic Surgery Network (CTS Net) and personal contacts. The survey was sent by email as an online link using Webropol (Webropol Oy, Helsinki). Altogether, 438 emails were sent to 214 surgeons because nonresponders were sent several emails. Of the 214 surgeons, 39 were congenital cardiac surgeons or were not performing cardiac surgery. Out of the remaining 175 surgeons, 97 (55.4%) completed the questionnaire comprising the final study population.
Results
The geographical distribution of the responders was as follows: Of the 97 responders, 37 were from Finland, 29 from Sweden, 16 from Norway, 13 from Denmark, and 2 from Estonia. In all, 26% of them had worked as cardiac surgeons for less than 10 years, 44% for 10–20 years, and 30% for more than 20 years. A great majority of the surgeons (91%) worked at a university hospital. Overall, 48% of the responders reported that their institution had formal guidelines for the prevention of postoperative AF.
Most commonly, oral beta-blockers (62%) were used for AF prophylaxis (Fig. 1). The reasons for not using oral beta-blockers postoperatively were unconvincing evidence of the benefits of beta-blockers (47%) or preference for some alternative therapy (32%) (Table 1). Only 6% of the responders used intravenous beta-blockers frequently for AF prophylaxis (Fig. 1). The main reasons for nonuse of intravenous beta-blockers were lack of confidence in the evidence (32%) and/or perception that their administration was cumbersome and time-consuming (20.5%), also alternative therapy was preferred (41%) (Table 1). The main perceived complications were bradycardia, hypotension, and low output syndrome.
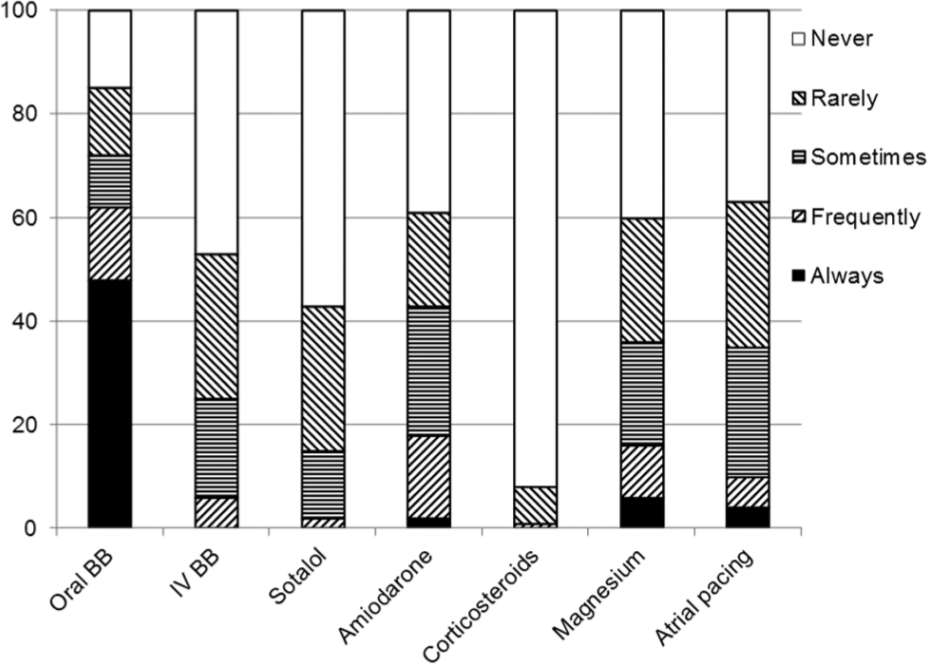
The use of different strategies for the prevention of postoperative atrial fibrillation among cardiac surgeons in Nordic countries.
Reasons for nonuse of different strategies for the prevention of postoperative atrial fibrillation among cardiac surgeons in Nordic countries (numbers in percentages, more than one alternative available).
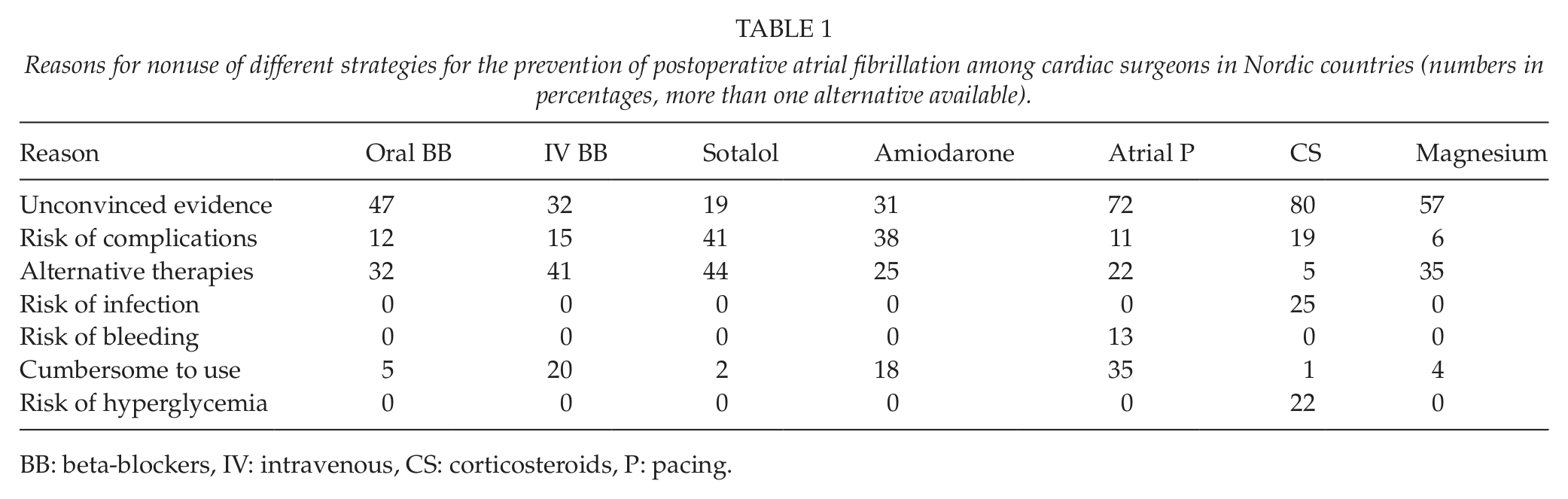
BB: beta-blockers, IV: intravenous, CS: corticosteroids, P: pacing.
Sotalol was reported to be used never or only rarely by 85% of responders (Fig. 1). The reasons for nonuse were as follows: fear of increased risk of complication (41%), unconvincing evidence of benefits (19.5%), and use of preferred alternative therapy (44%) (Table 1).
Amiodarone was used for AF prophylaxis always or frequently by 18% of responders (Fig. 1). Those who were reported to use amiodarone never or only rarely for AF prevention cited unconvincing evidence (31%), fear of complications (38%), cumbersome strategy (18%), or preferred alternative therapy (25%) (Table 1) as reasons for nonuse. Many surgeons answered that they use amiodarone for the treatment of AF but not for its prophylaxis.
Magnesium was used always or frequently for AF prophylaxis by 17% of the responders (Fig. 1). The most common reasons for nonuse of magnesium were unconvincing evidence of benefits (57%) or some alternative therapy (35%) (Table 1).
A majority (92%) of the responders had never used corticosteroids for AF prophylaxis (Fig. 1). More than half (54%) of them considered corticosteroids safe to be used as a part of cardiac surgery. Unconvincing evidence of benefits (80%), fear of increased risk of wound infections (25%), and fear of increased risk of hyperglycemia (22%) were the most common reasons for nonuse of this strategy (Table 1).
Only 11% of the respondents used atrial pacing for AF prophylaxis (always or frequently) (Fig. 1). The most common pacing site was left atria, and biatrial pacing was used only by 3% of surgeons. Those who never or rarely used atrial pacing reported lack of convincing evidence of benefits (72%) or were afraid of increased risk of arrhythmias (11.5%) or risk of bleeding (13%) (Table 1).
Other methods described by respondents for prevention of the AF were as follows: pericardial fenestration to left pleura, slow dehydration to preoperative weight, careful control of plasma electrolytes and hemoglobin, avoidance of cardiopulmonary bypass (off-pump coronary artery bypass grafting (OPCAB)), and proper cardioplegia with fast surgery.
Discussion
Among Nordic surgeons, oral beta-blockers were employed most commonly (62%) in the prevention of the postoperative AF. The use of oral beta-blockers turned out to be lower than we expected. The most common argument for nonuse of beta-blockers was “not convincing evidence of benefits.” This is of surprise, in light of the fact that the beneficial effects of beta-blockers in AF prophylaxis have been well documented in several RCTs and meta-analyses (12, 13), and guidelines recommend the prophylactic use of beta-blockers in all cases unless they are contraindicated (20, 21).
Intravenous beta-blockers are only rarely used for AF prophylaxis despite recent supportive evidence in the clinical literature. A prospective RCT demonstrated that intravenous metoprolol is more effective than oral metoprolol in AF prophylaxis (23). Similarly, another prospective RCT reported that the efficacy of intravenous metoprolol was comparable to intravenous amiodarone in AF prophylaxis (24). Despite this, only 6% of responders used (always or frequently) intravenous beta-blockers for AF prophylaxis.
Sotalol, a beta-blocker with class III properties, was used for AF prophylaxis only rarely (15%), mainly due to fear of side effects. Although sotalol has been shown to be effective in AF prevention (12, 13), it is reasonable to avoid its use because of its potential proarrhythmic effects (13).
It is of interest that amiodarone was reported to be used (almost always or frequently) by 18% of responders. This is a surprisingly high percentage, considering that according to recent guidelines amiodarone should not be used routinely but it should be reserved only for patients in whom beta-blocker therapy fails or is contraindicated (21).
Corticosteroids were used only rarely for AF prophylaxis. Only 1% of the responders used corticosteroids as routine practice for AF prevention. The most common reason for nonuse of corticosteroids was lack of evidence of benefits. Another reason for nonuse of corticosteroids was fear of side effects. In a recent study, corticosteroid treatment reduced the incidence of postoperative AF by 38% (18). The efficacy of corticosteroids has also been shown in another recent study (17) as well as in a meta-analysis (18). These studies reported no serious adverse effects related to corticosteroid use.
Magnesium was used for AF prophylaxis routinely by only 17% of responders. The main reason for nonuse was lack of evidence. Although the efficacy of magnesium in the prevention of AF has been documented (15, 16), there are still some open questions such as the optimum dose as well as its benefit when used with concomitant beta-blockers.
Only 11% of responders used atrial pacing for AF prophylaxis. The right atrium was the most commonly used pacing site, whereas biatrial pacing was used only rarely. This is somewhat unexpected in light of the evidence from RCTs and meta-analyses, which have shown that biatrial pacing is very effective in AF prevention (13).
The use of prophylactic strategies for postoperative AF after cardiac surgery has been studied previously among Canadian cardiac surgeons. It is of interest that in Canada, the use of beta-blockers, amiodarone, or corticosteroids for AF prevention was almost identical to the results of our study (22). In addition, the reasons for nonuse of prophylactic strategies were almost identical to our study.
One obvious limitation of our study is that it was performed only by cardiac surgeons. In several cardiac centers, postoperative care is provided by cardiologists or cardiac anesthesiologists, and thus it would be of significant interest to repeat this questionnaire among this population of health-care providers. Another limitation of our study is that only 55.4% of the surgeons responded to the survey. However, the percentage of responders is high enough for the results to be generalized (25).
In summary, this survey has demonstrated that there remains wide variability in the therapeutic approaches to AF prophylaxis among Scandinavian cardiac surgeons. This finding supports the need for definitive trials with convincing numbers of patients to resolve this pressing question. The similarity of the findings across two continents implies that there would be international interest in this research directive.