
Abstract
Background and Aims:
Although declining, cystic echinococcosis is still a serious public health issue in Greece. This study evaluated the clinical features, management, and short-term outcome of patients with complicated liver echinococcosis.
Material and Methods:
A total of 227 patients who were operated on for 322 echinococcal cysts of the liver were retrospectively evaluated. Patients were divided into those with complicated disease (53.7%) and those with noncomplicated disease (46.3%). Intrabiliary rupture (34.4%), cyst infection (32.7%), and their combination (24.5%) were the most common complications. Demographic characteristics, previous hydatid cyst surgery, cyst multiplicity and location, presenting symptoms and signs, types of complicated disease, operative procedures performed, postoperative complications, and hospital stay were assessed.
Results:
Patient demographics and cyst characteristics demonstrated no significant difference between the two groups. The complicated disease group had significantly more pronounced clinical presentations and higher postoperative morbidity. Choice of surgical procedure depended upon cyst location and surgeon preference. Both conservative and radical procedures were performed, supplemented with additional management of the biliary tree when indicated.
Conclusions:
Complicated liver echinococcosis demonstrates several distinct features that differentiate it from the noncomplicated disease. Frequently severe clinical manifestations, complexity of surgical management, and the increased postoperative complications characterize complicated liver echinococcal disease.
Introduction
Cystic echinococcosis or hydatid disease, a zoonosis caused by the adult or larval stages of the cestode Echinococcus granulosus, is a disease widespread in Greece since ancient times. National surveillance programs implemented during the last decades have contributed to a continuous decline of the parasite’s prevalence in humans. According to official records, the annual incidence of human echinococcosis has decreased from 14.8 per 100,000 inhabitants during the 1967–1971 period to 0.3 per 100,000 in 2003 (1). Nevertheless, echinococcosis is still present in Greece, representing a serious public health problem.
The parasite’s lifecycle is almost exclusively domestic involving dogs as definitive hosts and sheep or (accidentally) humans as intermediate hosts. The adult tapeworm resides in the small bowel of canines and produces eggs that contaminate vegetables with the feces. Humans become infected by eating contaminated vegetables, and the ingested eggs free their larvae in the duodenum. After crossing the intestinal wall, the larvae enter the portal system and reach the liver. Although many of them are destroyed in the liver, those that survive develop into hydatid cysts. Being the first organ of passage, the liver is the most frequently infected (50%–75%), followed by the lungs (20%–25%) and various other organs (15%–20%) via arterial dissemination (2, 3).
Once settled in the liver, larvae develop into cysts, which grow 1 cm in the first 6 months and 2–3 cm per year thereafter (4, 5). The cysts remain asymptomatic for many years, but as they increase in size, symptoms and complications arise. Adjacent structures and organs can be involved with the formation of fistulous tracts. Daughter cysts, which develop inside the primary cysts, can be disseminated into the biliary tree, pleura bronchi, or the peritoneal cavity.
In this study, we retrospectively evaluated patients with both complicated liver echinococcosis (CLE) and noncomplicated liver echinococcosis (NCLE) treated operatively at our department in order to identify possible differences in clinical characteristics, management, or outcome.
Patients and Methods
Patients with hepatic hydatid cysts who were treated surgically between January 1980 and January 2010 were retrospectively evaluated in this study. Preoperative diagnosis was based on history, clinical examination, abdominal ultrasound (US), computerized tomography (CT), and recently, magnetic resonance imaging (MRI) (Figs 1, 2). Liver function tests and blood eosinophils have very low sensitivity and therefore were not routinely used to support the diagnosis. Diagnostic adjuncts including Casoni skin test and liver scintigraphy, initially used during the early phases of the study, were gradually abandoned.
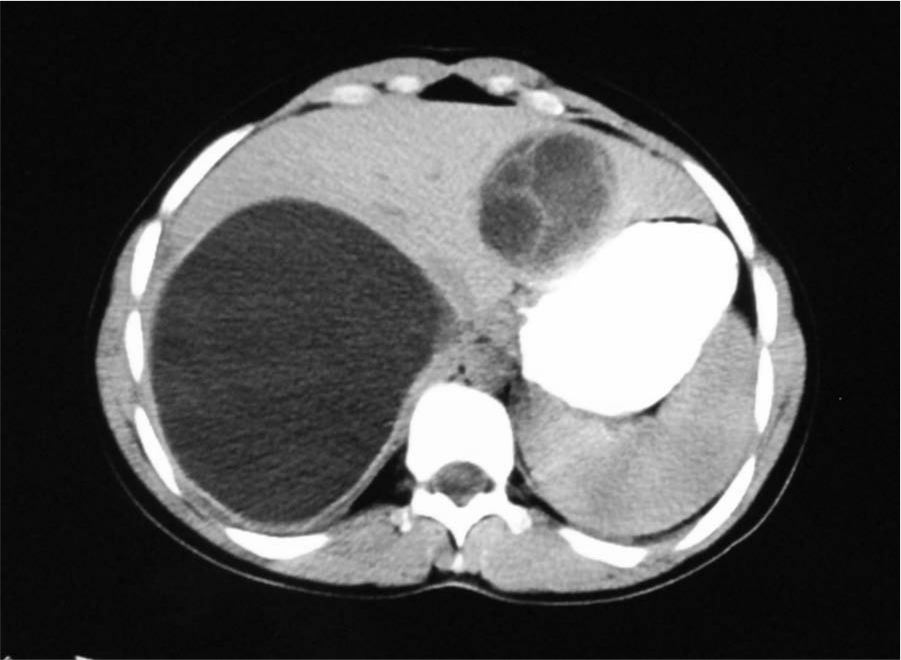
CT of uncomplicated liver hydatid cysts.
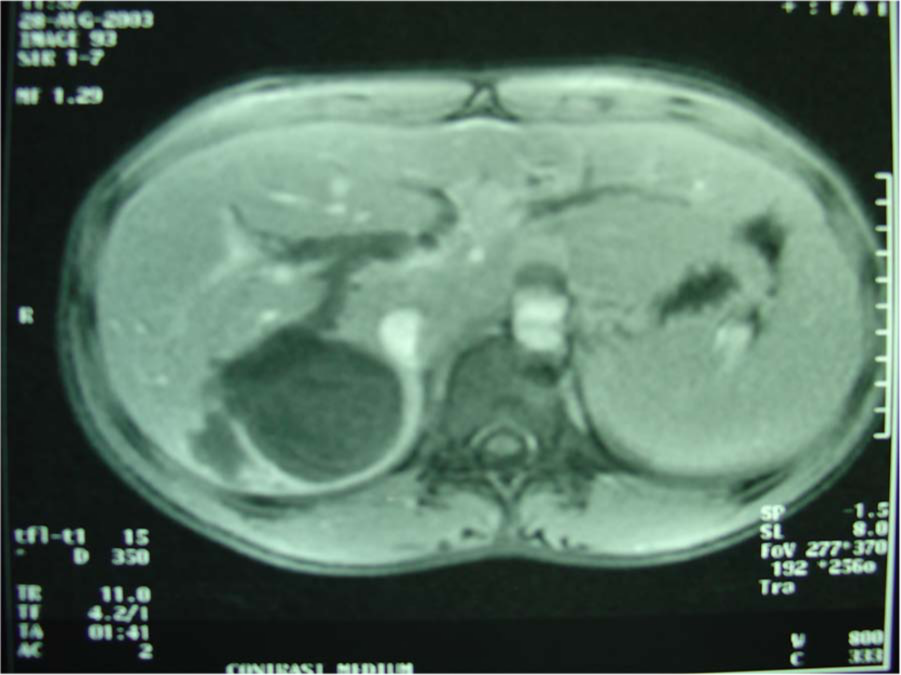
MRI showing communication of the hydatid cyst with the biliary tree.
The patients were divided into two groups, those with complicated disease (CLE) (53.7%) and those with noncomplicated disease (NCLE) (46.3%). Patients were included in the CLE group if presented with the following symptoms: (a) preoperative diagnosis of intrabiliary rupture with jaundice and possibly cholangitis, (b) preoperative diagnosis of intrabronchial rupture, (c) intraoperative diagnosis of peritoneal perforation, and (d) intraoperative cyst aspiration demonstrating bile-stained or purulent content. The remaining patients were assigned to the NCLE group.
Once identified, liver hydatid cysts were indicated for surgery except uncomplicated multiple cysts, smaller than 4 cm in diameter, located deep in the liver parenchyma, which were managed with chemotherapy and regular imaging studies. Fully calcified cysts were managed with observation alone. Patients with liver hydatid disease presenting preoperatively with biliary tree obstruction were either investigated with magnetic resonance cholangiopancreatography (MRCP), which was available during the last years of the study, or subjected to endoscopic retrograde cholangiopancreatography (ERCP) for identification of the cystobiliary tree communication and bile duct drainage. The choice of operative approach between conservative and radical procedures (Figs 3, 4) depended on the location of the cyst and the preference of the surgeon. Intraoperatively, the operative field was carefully isolated by gauge packs soaked with scolicidal agent (10% hypertonic solution) in order to prevent any inadvertent spillage to the peritoneal cavity during the procedure. When a drainage procedure was selected, the cyst contents were aspirated, and if bile-stained or purulent content was found, the cyst was then classified as complicated. The cavity was carefully examined for sites of bile leakage that were sutured if found. Whenever a larger communication was suspected, intraoperative cholangiography was performed followed by additional biliary manipulation. Management of the residual cavity following conservative surgical approach was performed with either external drainage or omentoplasty. Omentoplasty was performed by constructing an omental flap followed by packing and fixation of the flap in the residual cavity.
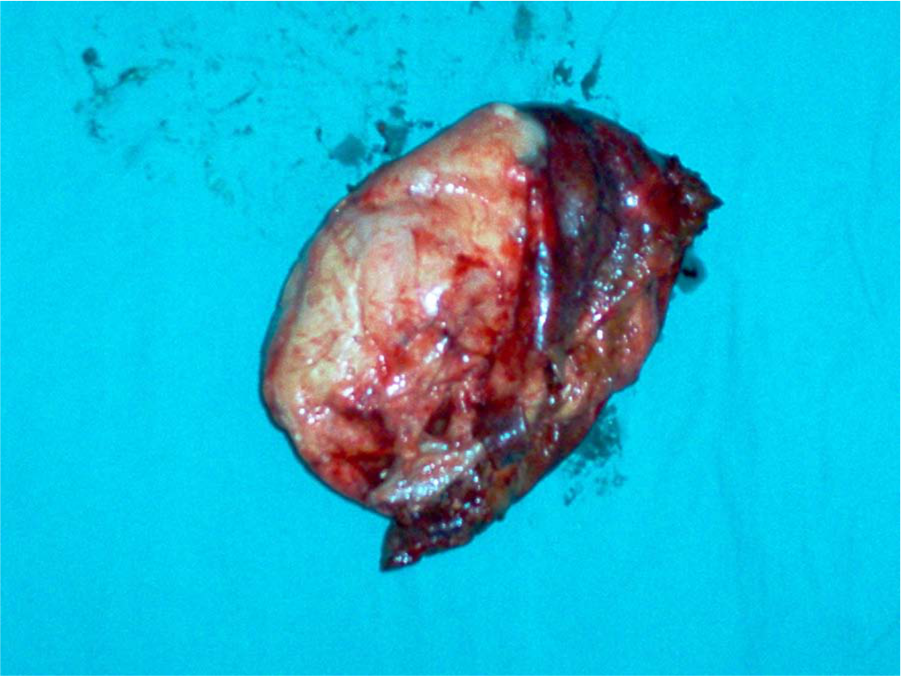
Intact resected liver hydatid cyst.
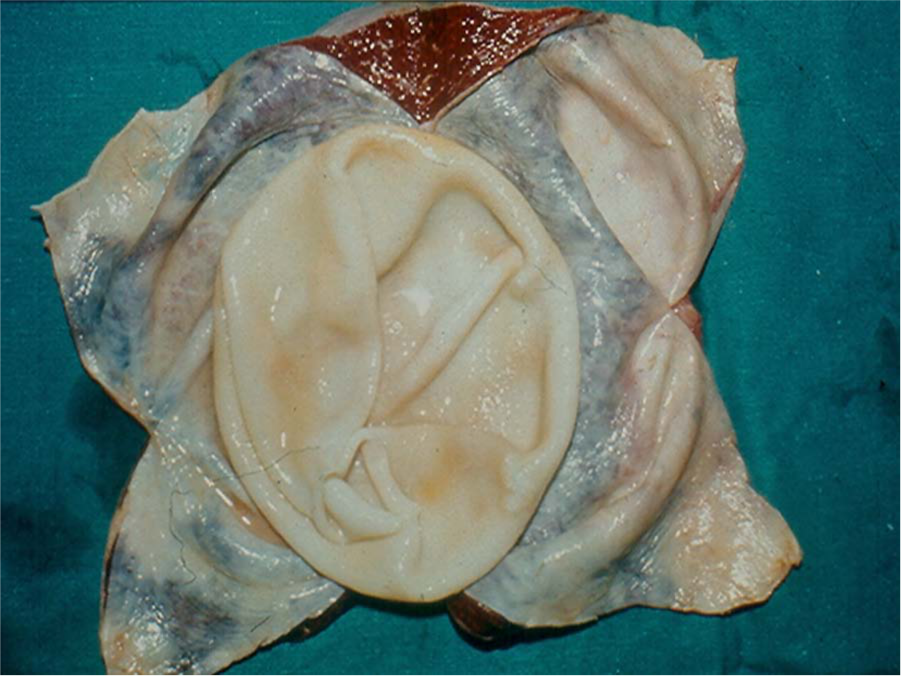
Opened cyst showing the inner parasite-derived layer (germinal membrane) and the outer fibrous layer.
Medical treatment for hydatidosis was administered for a brief preoperative period (7 days) and was prescribed postoperatively to all patients undergoing conservative surgical management and generally for those with suspected residual disease or peritoneal spillage in order to prevent postoperative recurrence. Albendazole 15 mg/kg/day was administered postoperatively in 28-day cycle followed by a 14-day albendazole-free interval for a total of 3 cycles. Liver function tests were scheduled regularly.
Statistical analysis was done using the χ2 test and the Fisher’s exact test when a value lower than 5 was expected. Mann–Whitney test was used for the comparison of ranked categorical data. A p value of <0.05 was considered statistically significant.
Results
Patient demographics were analyzed in order to detect possible differences between CLE and NCLE (Table 1). Female patients outnumber males in all groups, but the sex ratio was not statistically different between the two groups. Patients having CLE had lower mean age (47.3 ± 15.5) than the patients with NCLE (53 ± 15.9), but without statistical significance. Most of the patients from both groups were operated on for the first time, but 13.3% of the patients with CLE and 16.4% with NCLE had previous surgery for echinococcal disease. Surgery for multiple (2–4) hydatid cysts was performed in 38.8% of all patients without statistical difference between the two groups. A total of 322 cysts were surgically treated, 177 in patients with CLE and 145 with NCLE. The right lobe of the liver was the most common cyst location (66.1%) in both groups. Cysts in the left lobe were found in 21.1% of all patients, and 12.8% had bilateral cysts.
Patient demographics according to group.
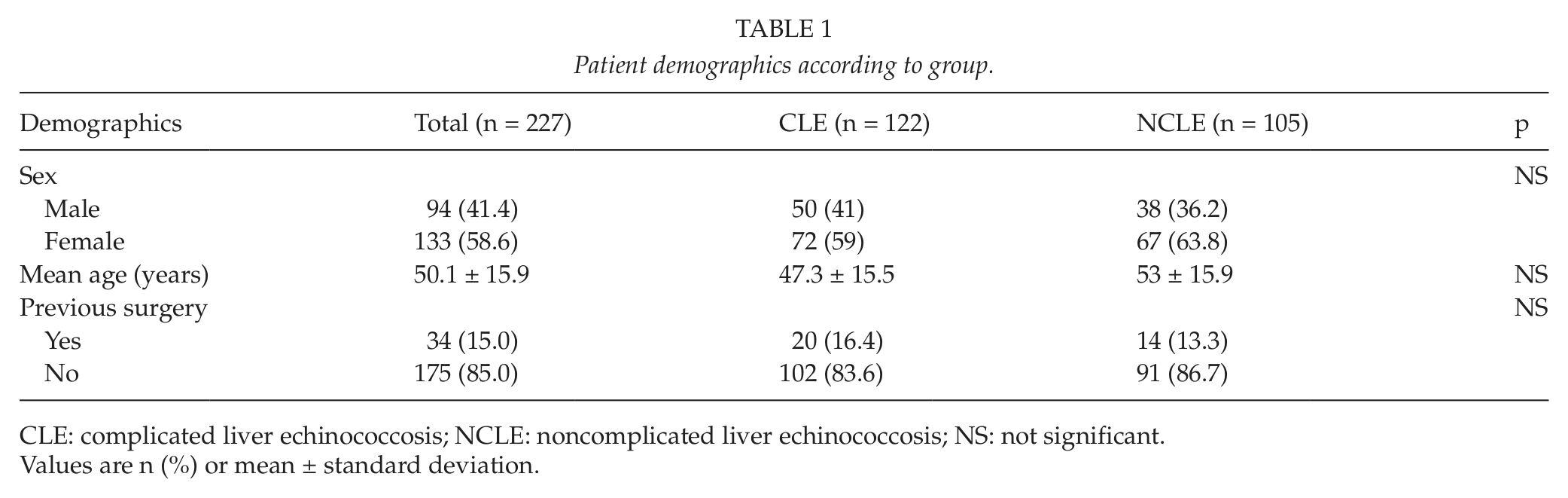
CLE: complicated liver echinococcosis; NCLE: noncomplicated liver echinococcosis; NS: not significant.
Values are n (%) or mean ± standard deviation.
Significant differences in the clinical manifestations of the two forms of the disease were discovered with fever, jaundice, and allergic reactions more common in patients with CLE and incidental discovery of the disease in more patients of the NCLE group. Presenting signs and symptoms are demonstrated in Table 2.
Presenting signs and symptoms.
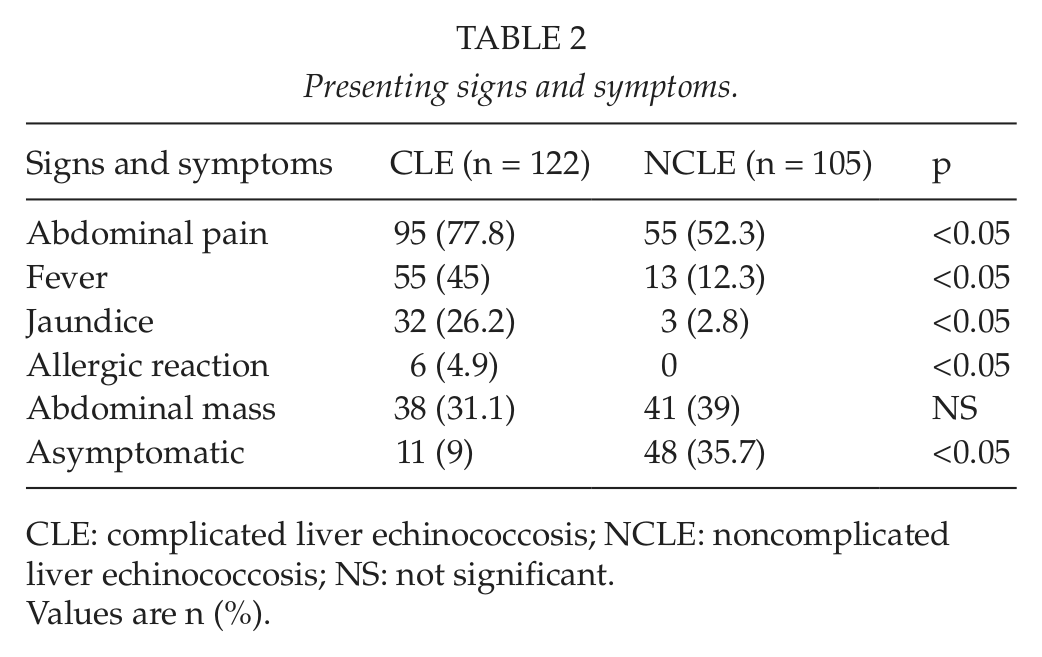
CLE: complicated liver echinococcosis; NCLE: noncomplicated liver echinococcosis; NS: not significant.
Values are n (%).
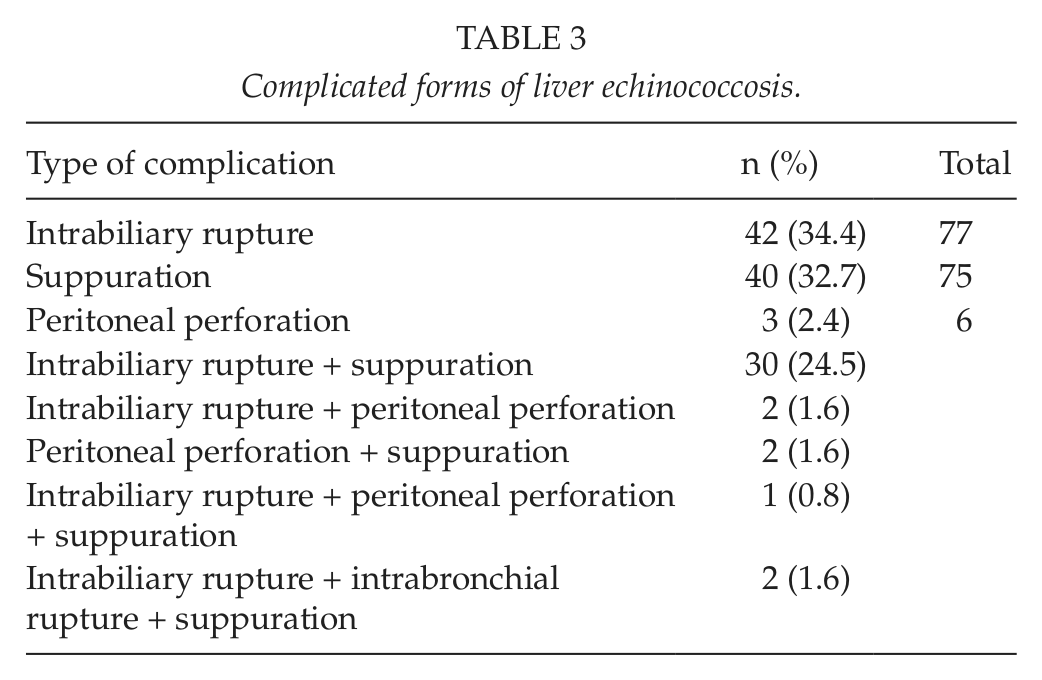
Specific complication types are demonstrated in Table 3. The most frequent type was intrabiliary rupture, presenting in 77 patients with CLE (either alone or combined with other complications). Suppuration was encountered in slightly fewer cases (n = 75), while the combination of intrabiliary rupture and suppuration was present in 30 patients. Hydatid disease presented with peritoneal perforation only in 6 cases, combined with other forms of complications in 3 of them. The rare combination of intrabiliary rupture, intrabronchial rupture, and suppuration was present in 2 patients.
Complicated forms of liver echinococcosis.
Right subcostal incision was the most prevalent incision performed (86%), followed by bilateral subcostal (7%) and rarely midline or thoracoabdominal incision. Surgical procedures selected to manage complicated and noncomplicated cysts are demonstrated in Table 4. Radical procedures were chosen in 83 cysts (45 complicated and 38 noncomplicated). The majority of them were managed with total pericystectomy and only 7 with hepatectomy. On the contrary, conservative procedures were used in the remaining 239 cysts. Partial pericystectomy with external drainage was the preferred option in both groups, followed by unroofing and drainage or partial pericystectomy and omentoplasty in fewer cases. Additionally, 8 patients underwent choledochotomy due to intrabiliary rupture involving the common bile duct, followed by subsequent management of the duct with choledochoduodenostomy, primary closure, T-tube placement, or sphincteroplasty.
Types of surgical procedures according to group.
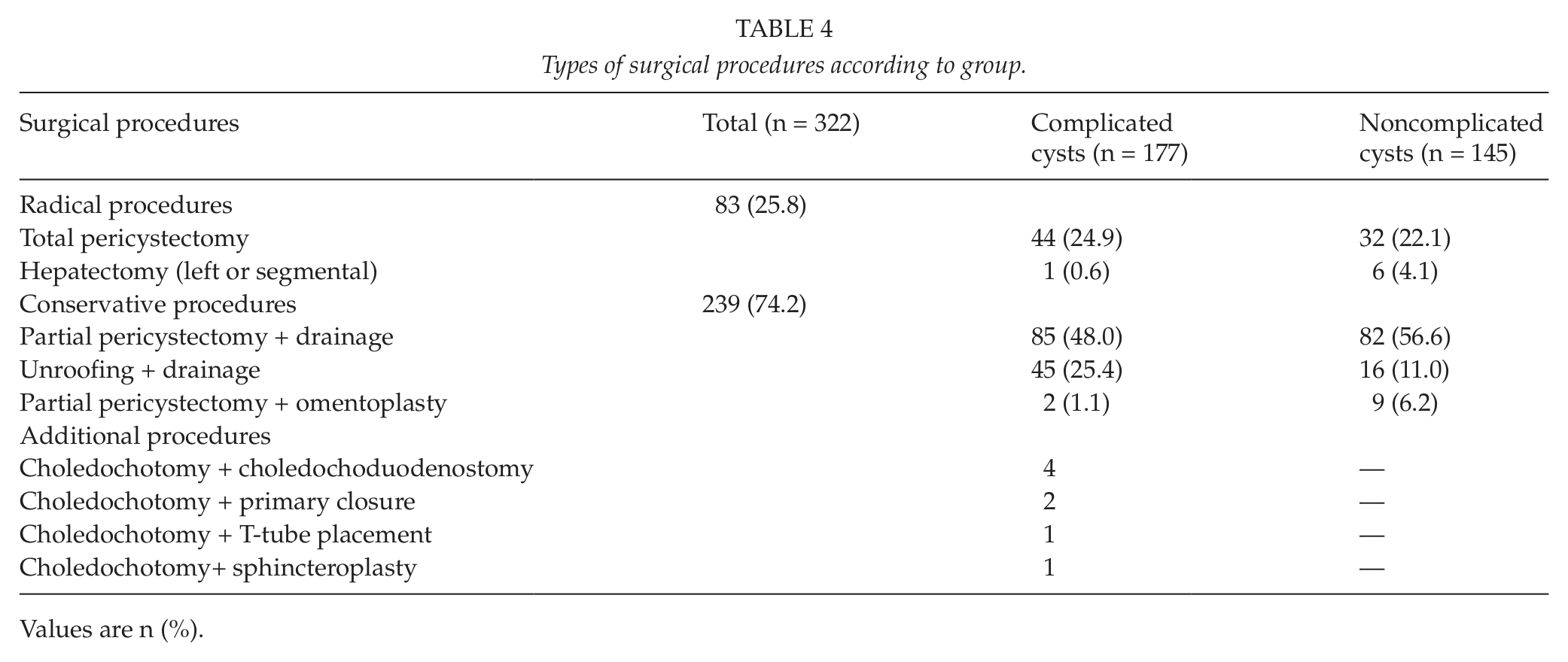
Values are n (%).
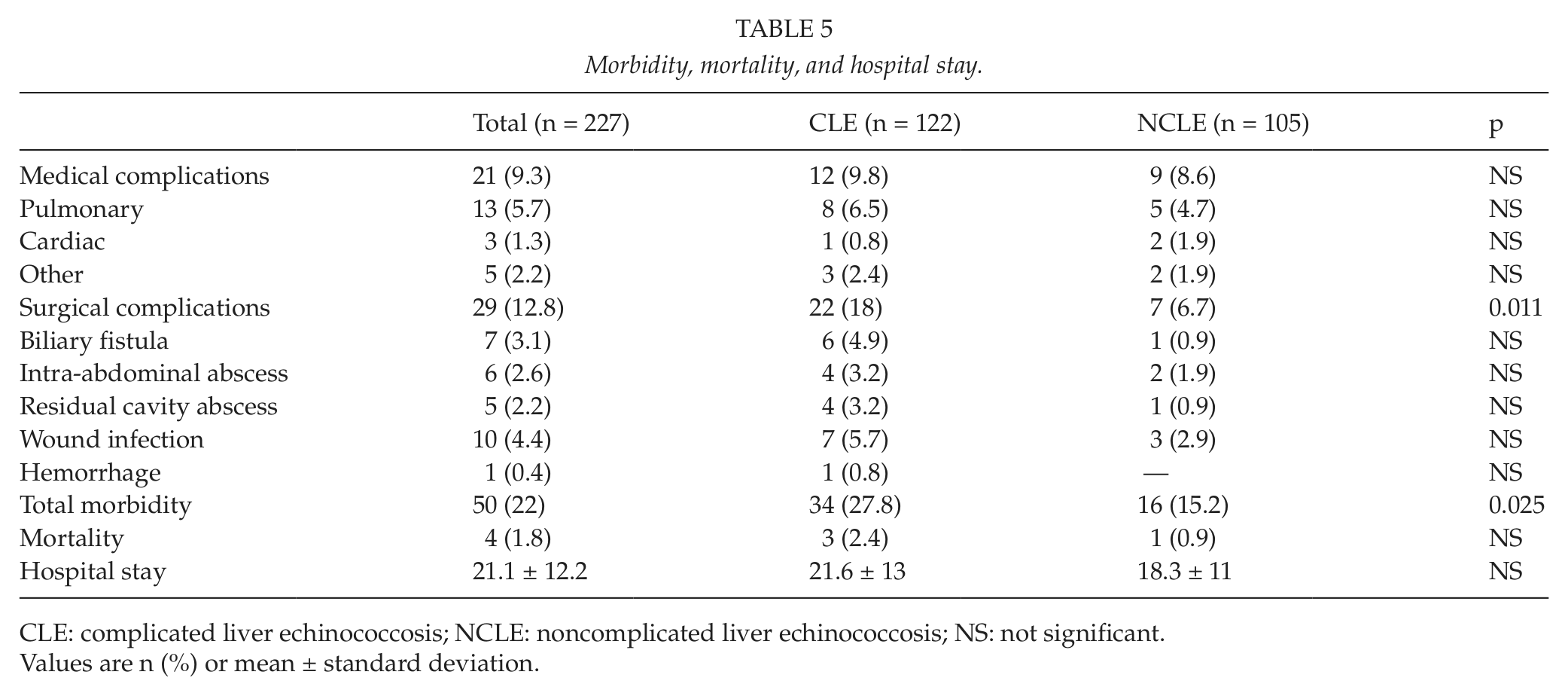
Morbidity, mortality, and hospital stay are demonstrated in Table 5. Medical complications showed no statistical difference between complicated and noncomplicated cases, but surgical complications including biliary fistula, intra-abdominal abscess, residual cavity abscess, wound infection, and hemorrhage were found significantly higher in the CLE group (p = 0.011). Overall mortality rate in our series was 1.8%, with no statistical difference between the two groups. CLE group demonstrated a mean hospital stay of 21.6 days, whereas patients of NCLE stayed at hospital for an average of 18.3 days (p = 0.141).
Morbidity, mortality, and hospital stay.
CLE: complicated liver echinococcosis; NCLE: noncomplicated liver echinococcosis; NS: not significant.
Values are n (%) or mean ± standard deviation.
Discussion
Complicated forms of liver echinococcal disease are not uncommon. The incidence of CLE reported in various studies ranges between one-third to as high as 60% of the total number of patients diagnosed and treated for echinococcal disease (6–8). In the present series, more than half (53.7%) of the patients treated for echinococcal cysts had CLE. The majority (61%) of complicated cases were detected preoperatively, representing a higher rate compared with other series (30.3%–34.7%) (9, 10). The most frequently encountered complications were intrabiliary rupture and suppuration of the cyst, which is also a repeated finding in literature. Minimally invasive techniques have been proposed, such as percutaneous aspiration injection and reaspiration (PAIR) and videolaparoscopy (11). Although the laparoscopic approach has recently been applied for the treatment of uncomplicated liver hydatid cysts, in our study, no such case has been included. Open surgery was the preferred treatment modality by the surgeons in this study, especially for CLE, which demonstrates increased technical difficulties and necessity for additional procedures. Recently, many surgeons favor total pericystectomy and liver resections as the ideal treatment for cystic echinococcosis because they demonstrate lower recurrence rates (8). These more radical surgical approaches have become feasible and safe with the application of novel liver resection instrumentation, which was not available to the surgical team during the first two decades of our study. As a result, conservative surgical procedures were selected more frequently in both groups. Cyst location and size, presence and type of complications, and surgeons’ preference also influenced the choice of operative approach. The higher incidence of postoperative complications in the CLE group is a rather predictable result considering the difficulties associated with complicated disease management. Supplementary postoperative chemotherapy is indicated in complicated cases, taking into consideration that CLE is characterized by communication or rupture of the cyst into adjacent structures or the peritoneal cavity and should be regarded as disseminated disease.
Intrabiliary rupture of hepatic hydatid cysts represents the most frequent complication of liver echinococcosis having an incidence rate of 1%–25% (12–14). According to our results, 34% of the patients were either diagnosed preoperatively or bile-stained cyst content was found intraoperatively. Cystobiliary communication results from compression of bile ducts from the gradually increasing cysts, causing bile stasis. The increased intraductal pressure induces fissure formation in the duct wall, and bile is accumulated at the external side of the cyst. Local osmotic pressure changes lead to the rupture of the cyst to the eroded duct, and the communication is established (6, 15). Intrabiliary rupture may be either silent or symptomatic (16, 17). The majority of the patients with intrabiliary rupture in our series (45/77, 58.4%) did not manifest jaundice on initial presentation or preoperatively. Silent rupture involves small bile ducts, while symptomatic rupture is associated mainly with larger ducts and probably extrahepatic bile tree. Biliary colic, cholangitis, jaundice, and more rarely, the presence of germinal membranes in feces are the expected manifestations.
The management of cystobiliary communication in our series depended on the preoperative and intraoperative findings. In case of partial pericystectomy, meticulous search for the orifice of the possible fistula was attempted at first. Corrugation of the interior surface of the cyst after decompression usually impedes such an effort. A clean gauze pad impregnated with hypertonic saline was applied inside the cyst and left there for 5 min in order to detect the orifice. More interventional techniques such as infusion of methylene blue or air in the common bile duct were not utilized. In several cases, the orifice of the fistula could not be detected and no further management was attempted. This could be explained by either the obliteration of the small communicating fistula because of the parasite’s death after bile insertion inside the cyst, the transection of the fistula during the redundant pericyst excision, or the accidental obliteration of the orifice by sutures placed to the rim of the cyst. Orifices of small fistulas are suture-ligated but larger communication, associated or not associated with episodes of preoperative cholangitis, jaundice, or the finding of dilated common bile duct, requires additional procedures. Choledochotomy and Fogarty catheter clearing of the common bile duct from hydatid cysts and parasitic debris was performed in 8 cases. Further management with choledochoduodenostomy, T-tube placement, sphincteroplasty, or primary closure depended on surgeon’s preference. Intraoperative cholangiography or ultrasonography was supplementarily used in order to search for parasitic material inside the extrahepatic biliary tree or to detect the cystobiliary communication. Cholecystectomy was performed in order to facilitate manipulation of a cyst adjacent to the gallbladder or due to cholelithiasis. Other indications of cholecystectomy are the presence of a fistula between the hydatid cyst and the gallbladder (18, 19) and the primary hydatidosis of the gallbladder (20), which are both very rare entities.
ERCP is a valuable adjunct in the management of CLE with symptomatic intrabiliary rupture, although MRCP is also widely used for diagnostic purposes. ERCP is indicated preoperatively when clinical symptoms of acute cholangitis are present and endoscopic papillotomy should be performed when hydatid material is detected inside the common bile duct (21). Indications for postoperative endoscopic papillotomy are the presence of a biliary fistula with persistent high output, remaining hydatid material in the common bile duct, and jaundice (22). Vignote et al. (23) reported that persisting fistulas usually close 5–7 days after papillotomy. In our series, 5 patients underwent endoscopic papillotomy, 2 preoperatively and 3 postoperatively.
Suppuration of the echinococcal cysts was encountered in 23% of cysts managed in our series, this being a very common complication (24, 25). The presence of cyst leakage is essential for bacterial contamination of the endocystic fluid, and therefore, it is believed that cystobiliary communication is the more frequent cause of infection (24, 26). The coexistence of suppuration and intrabiliary rupture in 30 of our total 75 infected cysts rather confirms the previous aspect. Clinical manifestations in acute cyst infection resemble those of liver pyogenic abscess (pyrexia, chills, sepsis, and increased pain).
Peritoneal rupture of echinococcal cysts is a more rare but hazardous complication (6 patients in our series). Abdominal trauma combined with the presence of large, superficial, thin-walled cysts in the anterior and inferior part of liver are factors predisposing in cyst rupture, although spontaneous rupture is not uncommon (6, 27). Clinical presentation includes anaphylactic shock, acute abdomen, or both. Peritoneal rupture is sometimes silent, and disseminated secondary abdominal echinococcosis is disclosed after a long asymptomatic period, unaware when the rupture occurred (28). Surgical management in either symptomatic or silent rupture aims at the removal of all the cysts and profuse peritoneal lavage with scolicidal agents to prevent recurrence. Severe hypernatremia should be suspected and treated if hypertonic sodium chloride is used.
Cysts located at the upper liver surface may involve the diaphragm and extend to the pleural cavity and lungs. The incidence of transdiaphragmatic thoracic involvement ranges from 0.6% to 16% of cases with hepatic echinococcosis (0.8% in our series) (4, 29, 30). Diaphragm erosion could lead either to a frank intrapleural rupture with empyema, which is very rare due to the presence of pleural adhesions, or to the penetration of lung parenchyma resulting in pneumonitis or lung abscess. In the case of hydatid cyst ruptures to the lumen of a bronchiole, daughter cysts may appear in the sputum. If intrabiliary rupture has already occurred, a bronchobiliary fistula is generated, and expectoration of bile appears subsequently. Surgical treatment in such cases is rather laborious involving suturing of the bronchial fistula, segmental lung resection, or lobectomy (depending on the size of the fistula), local excision and suturing of the eroded diaphragm, decortication, management of the liver cyst, and abdominal and thoracic drainage. Transthoracic approach is more appropriate when a thoracic collection is present, while transabdominal approach is selected when management of the common bile duct is necessary (31–34). Two cases with bronchobiliary fistula were treated successfully in our department by simply suturing the fistula through a transabdominal approach.
In conclusion, CLE may be regarded as a common disease entity but with several distinct characteristics when compared with NCLE. The severe clinical manifestations not only contribute to the diagnosis of the disease but also could be fulminant and fatal, contrary to the usually silent progression of NCLE. Furthermore, the involvement of adjacent structures and organs in complicated and disseminated disease leads to complex and laborious operations with increased intraoperative risk, additional procedures, and increased morbidity. ERCP and endoscopic sphincterotomy are valuable procedures either preoperatively or postoperatively in order to avoid unfavorable biliary sequela. Circumstantially, manipulation of CLE should be regarded as a demanding procedure even in experienced hands.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.