
Abstract
Aim:
To study factors that influenced healing and survival after attempted closure of enterocutaneous fistula.
Material and Methods:
Retrospective analysis of prospective data concerning 101 patients operated on 132 instances for 110 enterocutaneous fistulae at two hospitals.
Results:
In all, 96 (87%) of the 110 fistulae healed and 92 (91%) patients survived. A total of 9 patients with unhealed fistula died. Multivariate analysis revealed jaundice as an independent factor for both death and failed closure and operation without anastomosis as an independent positive factor for healing. Failure rate was lower after an operation with stoma without anastomosis (6 of 43, 14%) than after an operation with anastomosis (30 of 89, 34%) p = 0.0213. Of the 36 instances with unhealed fistula, 13 (36%) could be ascribed to inadvertent bowel lesions at the reconstructive operation. In addition, univariate analysis revealed that patients with previous multiple laparotomies or with multiple operations for enterocutaneous fistula healed less likely and had higher mortality. A low serum albumin, high white blood cell count, high C-reactive protein concentration, high fistula output, total parenteral nutrition, and operation for recurrent fistula were associated with death together with long operation time and operative bleeding, both indicators of surgical complexity. Over time, staged surgery avoiding anastomosis increased from 27% to 57%. Mortality decreased from 12% to 6%, and healing increased from 73% to 94%.
Conclusions:
Chronic inflammation, malnutrition, and liver failure causing an impaired healing capacity are important reasons for failure. Staged operation without primary anastomosis may allow the patient to reverse this condition and improve outcome. The high surgical complexity is a negative factor that requires careful planning of the operation.
Introduction
Enterocutaneous fistula is one of the most demand-ing conditions encountered in surgical practice. Reconstructive operations are accompanied by high failure rate and mortality of 10% or more (1–4). The evidence base for the treatment is scarce, and the principles consist largely of expert opinions. The condition is heterogeneous, and even in specialized referral centers, the heterogeneity and relatively fewer patients limit the conduct of controlled studies. The present knowledge has evolved from retrospective analysis of case series (1–23). Most published studies are concerned with prognostic factors for spontaneous healing or closure after surgery. There are few studies on surgical strategy and technique, and so far, no one has studied the choice of primary anastomosis or stoma in reconstructive operations.
We studied 101 patients who had 132 reconstructive operations for enterocutaneous fistula at one primary and one secondary referral center over a 16-year period. The study aimed at identifying factors for healing and survival. In particular, we assessed outcome after an anastomosis or stoma at the reconstructive operation.
Patients and Methods
Patients
The study included 101 patients, 52 men, with 110 episodes of enterocutaneous or colocutaneous fistula. They had 132 reconstructive operations at the Linköping University Hospital or at the Falun County Hospital from January 1988 to December 2003. Median age at their first fistula operation was 52 years (range: 14–83 years). In all, 21 patients (14 men) were operated at the Falun County Hospital and 80 patients (38 men) at the Linköping University Hospital. All the patients operated at the Falun County Hospital came from its primary catchment area, whereas 52 (65%) of the 80 patients operated at the Linköping University Hospital were referred from other hospitals, and 9 had had prior attempts of reconstructive surgery of the fistula at their local hospital. During the study, 8 patients who were operated to healing developed a new fistula after 33 months (range: 11–109 months) with 1 patient experiencing two episodes. All had a new reconstructive operation. There were 81 enterocutaneous fistulae, 20 colocutaneous fistulae, and 9 fistulae that were a combination of both. During the study period, another 3 patients had operations because of enterocutaneous fistula: 1 patient had exploratory laparotomy and 2 patients had proximal diverting stoma without repair. These 3 patients were not included in the study.
Postoperative Fistula
There were 74 fistulae secondary to abdominal surgery, defined as a fistula appearing within 6 months after a laparotomy. The patients had a mean of 4 (range: 1–30) previous abdominal operations. In all, 17 patients had Crohn’s disease and 15 had ulcerative colitis with 12 fistulae developing after pouch surgery. A total of 14 patients developed fistula after operation for colorectal carcinoma, and 4 patients developed fistula after operations for diverticulitis. A total of 8 patients developed fistula after operation for intestinal obstruction with adhesiolysis, and 16 developed fistula after surgery for various other reasons.
Inadvertent bowel lesion was the cause of postoperative fistula if there was no anastomosis or intestinal suture line at the primary operation, or if the fistula did not arise from an anastomosis or suture line as evident from preoperative investigation or the reconstructive operation. In all, 15 (21%) of the postoperative fistulae were judged to be caused by inadvertent bowel lesion.
Spontaneous Fistula
Any fistula that appeared later than 6 months after previous surgery was judged as a spontaneous fistula. There were 36 patients with spontaneous fistula, 21 with Crohn’s disease, 5 with ulcerative colitis, and 2 with malignant disease. A total of 3 patients developed fistula from a ventral hernia. Two patients operated for colorectal carcinoma developed fistula without any sign of recurrent disease, and both were small bowel perineal fistula after Hartmann’s resection. Two developed fistula after diverticulitis. One developed fistula 13 years after removal of a continent ileostomy for hereditary polyposis.
Methods
Operations
The 101 patients had 132 reconstructive operations of 110 fistulae (Fig. 1). There were also 31 stoma closures. A reconstructive operation with subsequent stoma closure was regarded as one operation for the purpose of this study. A further 33 attempts to close a fistula in an open abdomen by simple suture were not included in the analysis as it always failed.
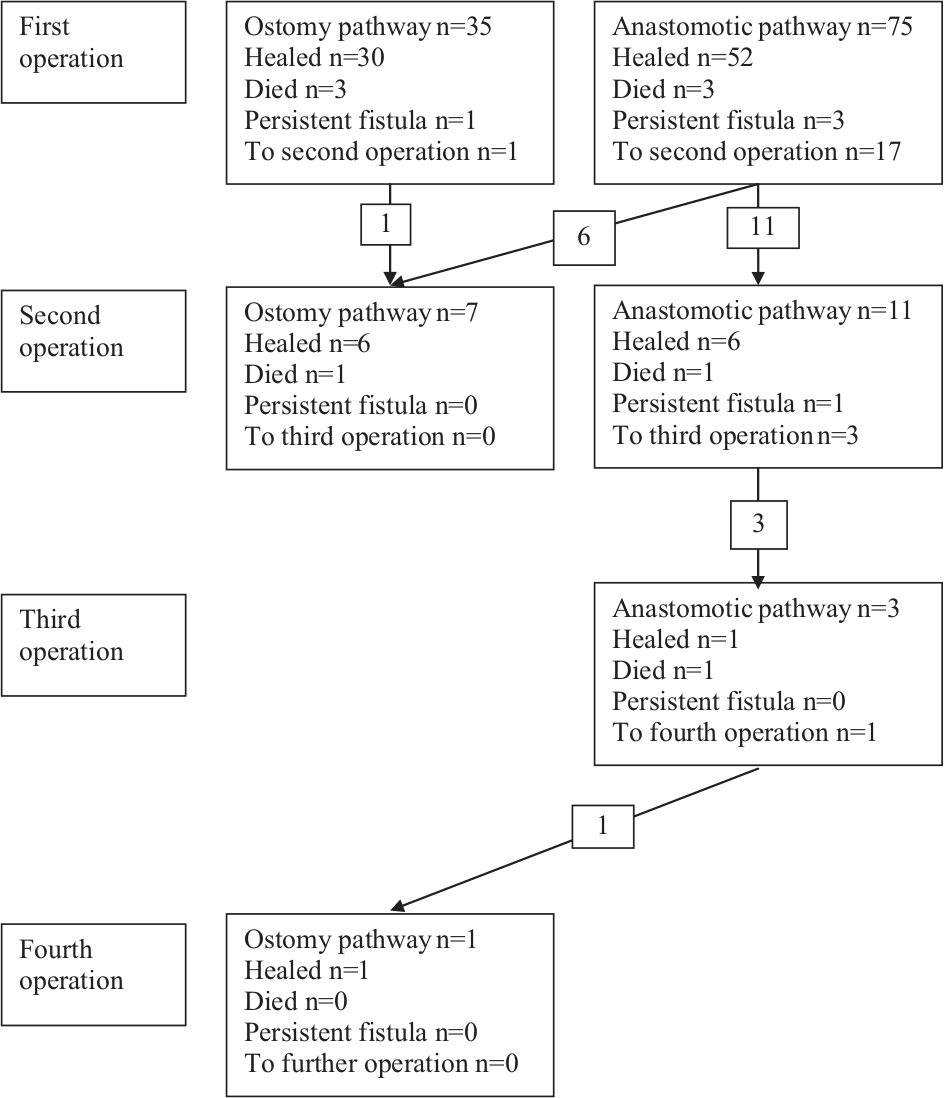
Flow chart of the study. The denominators are 132 operations for 110 fistulae in 101 patients.
Overall, 92 fistulae had one reconstructive operation, 15 fistulae had two operations, 2 fistulae had three operations, and 1 fistula had four reconstructive operations (Fig. 1).
The outcomes of interest were fistula healing and mortality. Healing was defined as absence of fistula 6 months after the reconstructive operation. In case of reconstruction with stoma, healing of the fistula was ascertained 6 months after stoma closure. Fistula-related mortality was recorded up to 6 months after reconstructive surgery.
Investigated variables
The analysis included the following variables obtained at the time of reconstructive surgery: age; gender; referral from other hospital; recurrent fistula after previous operation; spontaneous or postoperative fistula; time until reconstructive surgery after previous laparotomy; fistula output > 1000 mL a day, which was considered as high-output fistula; enterocutaneous, colocutaneous, or combined fistula; number of previous laparotomies; number of previous laparotomies for fistula; operation time; blood loss at operation; an open abdomen or not after reconstructive surgery; type of intestinal reconstruction; stoma; and anastomosis with or without proximal diverting stoma. Intestinal wedge resection and suture of the fistula tract are recorded as anastomosis for the purpose of this study. Laboratory values, namely, serum albumin, white blood cell count (WBC), C-reactive protein (CRP), and bilirubin were also included in the analysis. Systemic inflammation was defined as any of WBC more than 12, CRP more than 30, and serum albumin 30 or less. Jaundice was defined as serum bilirubin above 50 µmol/L.
Additional investigated variables were current smoking, preoperative use of enteral tube nutrition, total parenteral nutrition (TPN), previous irradiation to the abdomen or pelvis, corticosteroid treatment, immunosuppressive treatment (azathioprine, 6-mercaptopurine, methotrexate), and insulin treatment. In patients who had more than one reconstructive operation, the analysis on mortality was performed using the status at the first operation (index operation).
Follow-up
Patients were identified from registries of diagnoses and operation logs, and the medical records were reviewed. Referring hospitals were contacted to obtain information about patients who were discharged after reconstructive surgery. The follow-up extended on average for 23 months (median = 11 months, range: 8–132 months) after the reconstructive operation.
Statistics
Results are presented as median and range. Differences were analyzed with Mann–Whitney U-test or Fisher exact test, as appropriate, for nominal and categorical data. Multivariate analysis by means of logistic regression used healing and postoperative death as dependent variables. A p-value less than 0.05 determined statistical significance.
Results
Healing of Fistula After ReconstructiveOperation
In all, 96 (87%) of the fistulae were surgically treated to healing, 21 of 22 treated at the Falun County Hospital and 75 of 88 treated at the Linköping University Hospital. A total of 5 patients survived with unhealed fistula. Two patients had Crohn’s disease, both with low-producing fistula, of whom one healed after medical treatment and one remained at the end of the study period. One patient with ulcerative colitis healed after a new operation in another hospital but was unhealed in this analysis. One patient with disseminated malignant disease developed a low-producing new fistula and died more than 6 months later due to the malignancy. One patient with fistula after adhesiolysis failed to heal after the reconstructive surgery, but healed spontaneously 9 months later.
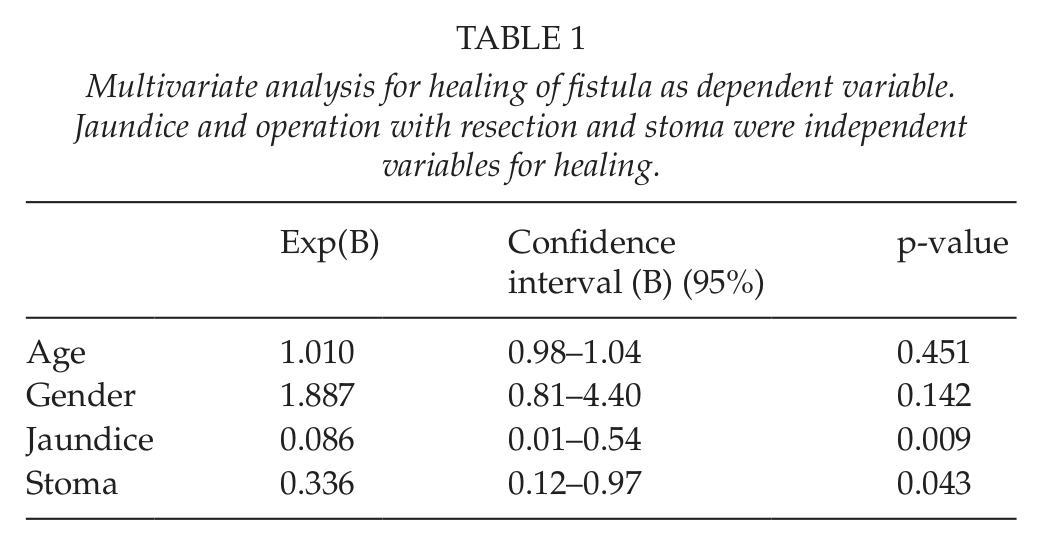
Table 1 shows the results of the multivariate analysis. A primary anastomosis and jaundice were independent variables of failed healing. Table 2 shows the results of the univariate analysis with respect to fistula healing. Healing was safer after resection with stoma than after primary anastomosis, 86% healed compared to 66% with an anastomosis. Healing rate did not differ whether or not patients with an anastomosis had a diverting stoma: healing was observed in 11 of 17 (65%) patients with diverting stoma and 48 of 72 (65%) without diverting stoma. Only 2 of 7 patients operated on when having jaundice healed.
Multivariate analysis for healing of fistula as dependent variable. Jaundice and operation with resection and stoma were independent variables for healing.
Univariate analysis of variables related to healing after reconstructive surgery in 101 patients with 132 operations for enterocutaneous or colocutaneous fistula.
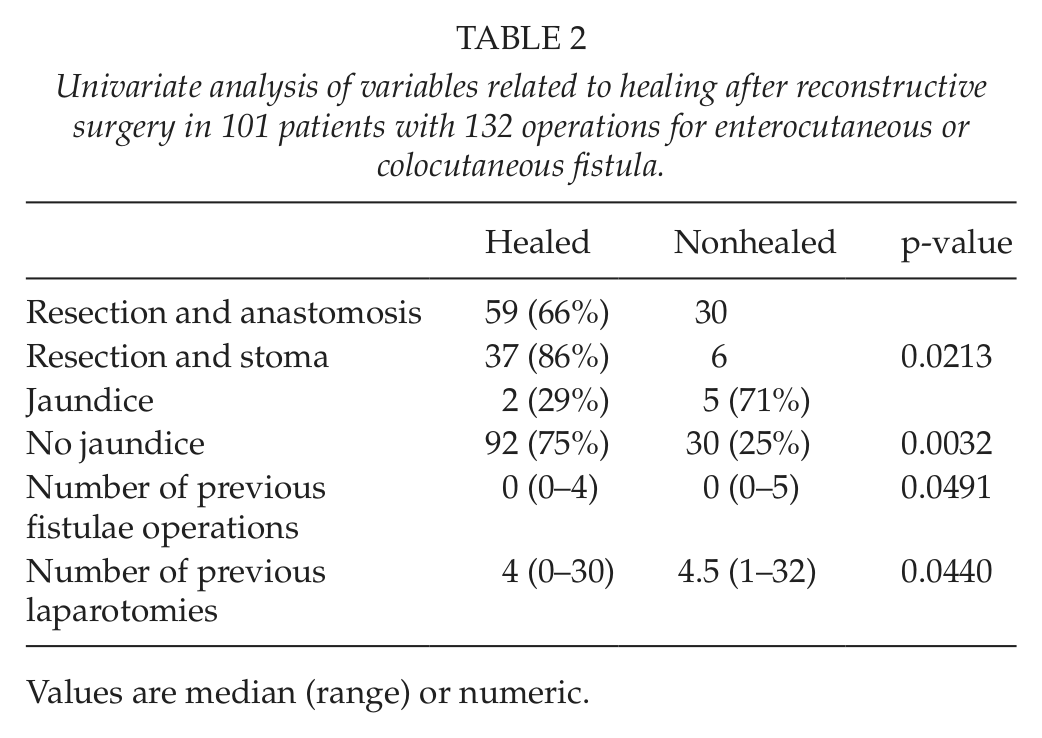
Values are median (range) or numeric.
All four operations with an open abdomen after reconstructive surgery resulted in nonhealed fistula compared to 32 of 128 with closed abdomen. All 20 operations for colocutaneous fistula resulted in healing compared to 78 of 92 operations for enterocutaneous or combined colocutaneous and enterocutaneous fistulae. None of these differences reached the level of statistical significance.
In 22 instances, patients survived with an unhealed fistula after the first reconstructive operation (Fig. 1). A total of 18 patients had further reconstructive operations; in 8 patients with resection and stoma, 7 (87%) patients healed; and in 14 instances with anastomosis, 7 (50%) healed (p = 0.167). One patient had three attempts with anastomosis, but healed after a fourth reconstructive operation with resection and stoma. He later had his stoma closed.
In all, 13 (36%) of 36 instances of unhealed fistula could be ascribed to inadvertent bowel lesion at the reconstructive operation. Overall, 22 (25%) of 92 survivors had a permanent stoma at the end of the study; 19 had an end stoma that was not possible to close. In the 28 patients operated with a stoma that was possible to close, 25 were closed while 3 remained.
Survival
In all, 92 patients survived while 9 (9%) patients died of causes related to the fistula, all treated at the Linköping University Hospital. All 9 deaths had unhealed fistula after attempted reconstructive surgery. The cause of death was uncontrolled infection with multiorgan failure. Another 2 patients died within the first 6 months of causes unrelated to the fistula: one urosepsis and one progressive malignant disease, both with healed fistula.
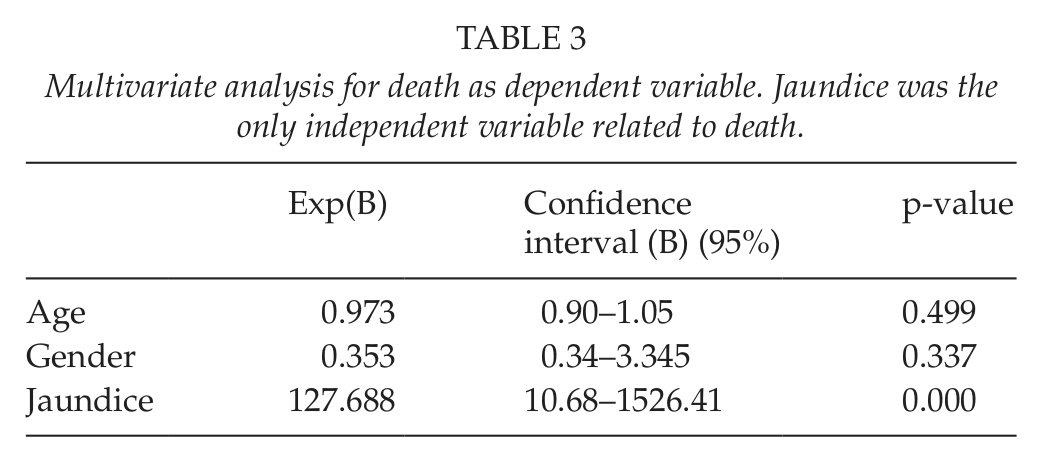
Table 3 shows the results after multivariate analysis for death as dependent variable. Jaundice was the only independent variable related to death. Table 4 shows the relation of the univariate analysis to death. In all, 5 of 7 patients with jaundice died. Patients who died had more laparotomies, more previous operations for the fistula, and more often a recurrent fistula. They had had longer operations and more operative blood loss. Their preoperative serum albumin was lower, and they had more signs of systemic inflammation. High-output fistula and preoperative treatment with TPN was more common.
Multivariate analysis for death as dependent variable. Jaundice was the only independent variable related to death.
Univariate analysis of variables related to death after reconstructive surgery in 101 patients operated for enterocutaneous or colocutaneous fistula.
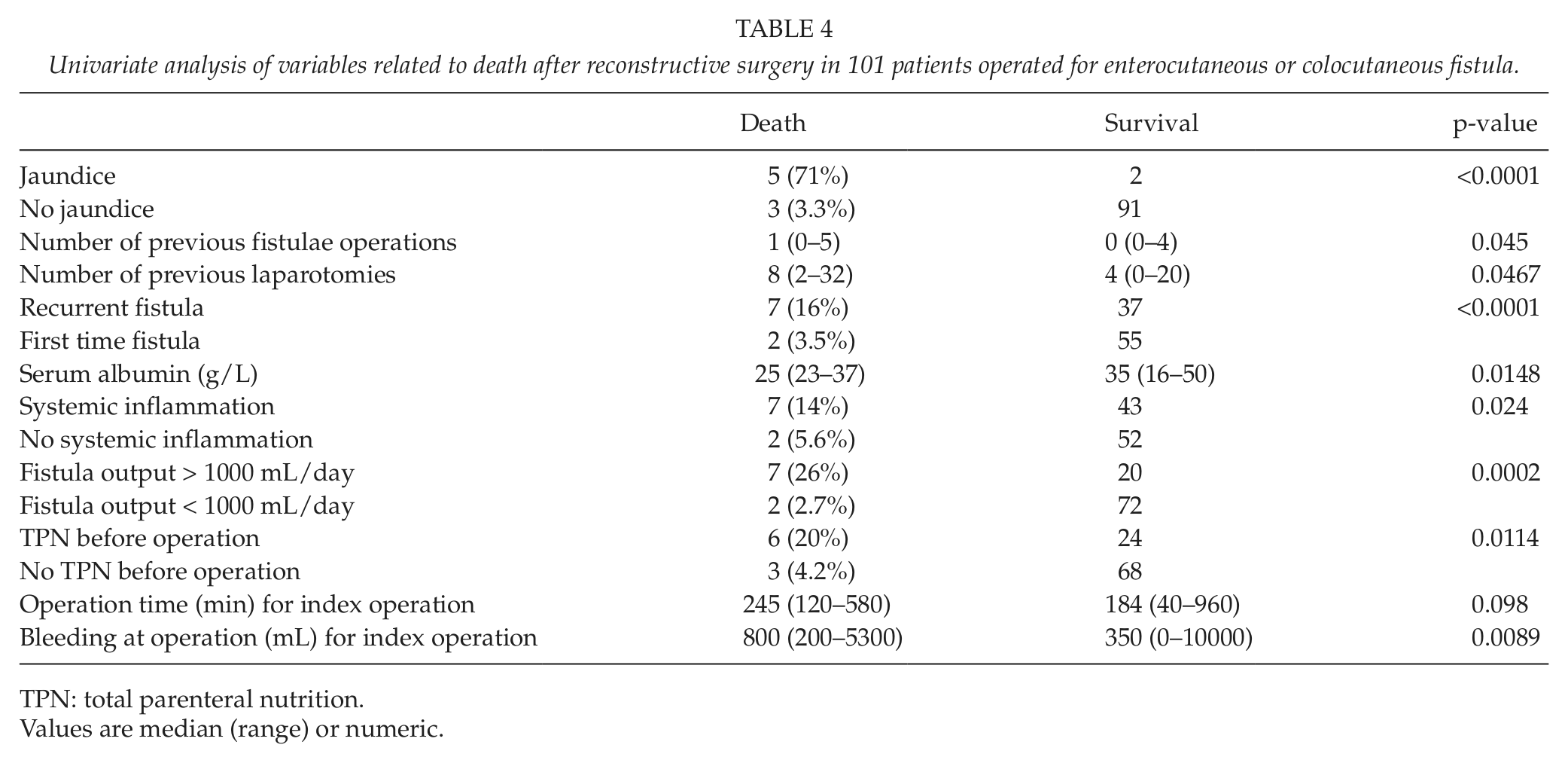
TPN: total parenteral nutrition.
Values are median (range) or numeric.
All 3 patients with an open abdomen after reconstructive surgery died compared to 6 of 91 with closed abdomen; this difference was not statistically significant.
Mortality and Healing: 1988–1999 Versus 2000–2003
The later period showed better outcome because mortality was lower and healing rate increased at the Linköping University Hospital. From the year 2000 and on, the operations and perioperative care were concentrated to one group of surgeons employing established principles for the treatment, including enteral sond nutrition largely replacing TPN, a time period of 6 months after previous laparotomy before fistula closure, and preferentially staged operations with stoma avoiding anastomosis (24–26). In this period, primary anastomosis was used in only 13 (43%) of 30 operations compared to 53 of 73 (73%) previously (p = 0.0023). Mortality decreased from 7 of 56 (12%) to 2 of 32 (6%) (p = 0.478), and healing rate increased from 41 of 56 (73%) to 30 of 32 (94%) (p = 0.0240).
Discussion
In all, 87% achieved fistula healing and 91% survived. These results are comparable to those of other recent studies (1, 3, 4). The treatment for enterocutaneous fistula exhibits failure rates and mortality that exceed many other surgical conditions. This has lead to the establishment of national centers for their treatment in several countries with the aim of concentrating the experience and improving outcome. The present results improved after the concentration of treatment to one group of surgeons with adherence to established treatment principles. The better results of the later phase were likely due to improved perioperative care, better surgical technique, and the change to staged surgery instead of primary anastomosis. This demonstrates that a referral center may achieve fistula healing in more than 90% with low mortality.
The failure rate, that is, persistence of the fistula, remains high, and a significant number of patients require repeated operations to achieve healing. Although difficult to extract from previous reports, failure rate after the first reconstructive operation seems to range from 21% to 36% (1, 4, 17). Our failure rate was 26% after the first operation and 33% after second or third reconstructive operation. There are two reasons for a persistent fistula: anastomotic dehiscence or inadvertent bowel lesion, the latter of which might be unrecognized at surgery. An anastomotic fistula is the most common cause of failure. It is remarkable that the issue of primary anastomosis or primary stoma with delayed anastomosis has not been addressed previously. The most interesting finding of this study is the improved result when patients were operated with a stoma without an anastomosis. The failure rate decreased from 34% with anastomosis to 14% with stoma. These figures are most likely biased because patients with one or several known risk factors were chosen to be operated with a stoma, following our experience of anastomotic failure in Crohn’s disease (27, 28). The failure risk of an anastomosis may be even higher than found here because the most severely ill patients were already operated without an anastomosis.
When the initial reconstruction failed followed by a new anastomosis at the second or third operation, failure rate approached 50% compared to 13% if the patient had a stoma. Anastomotic failure rates of 20% or more are rare in other conditions. The likely inability to heal an anastomosis must be included in the decision matrix when operating for fistula. Our experience shows that an operation without anastomosis is preferable whenever possible. At least one-third of our failures followed an inadvertent bowel lesion during the reconstructive procedure, which is another issue of great concern. These observations emphasize that impaired healing capacity is a common sequel of enterocutaneous fistula.
Operations for enterocutaneous fistula are technically demanding and complex. We found that blood loss, operation time, and multiple previous laparotomies were associated with failure, and all these circumstances are markers of surgical complexity. The high number of persistent fistula due to inadvertent lesions also emphasizes that these operations require certain operative skills.
All 3 patients with an open abdomen died. Abdominal closure with mesh is not an option as a study from Manchester showed refistulization in 24% and none when the abdomen could be sutured (25). If it is not possible to close the abdomen, myocutaneous flap technique may be considered.
Enterocutaneous fistula is a dangerous condition characterized by chronic systemic inflammation, intestinal losses, inability to proper oral nutrition, and subsequent malnutrition. Malnutrition is difficult to reverse in the presence of chronic systemic inflammation. TPN in these patients is associated with a risk of disordered liver function. Impaired liver function, expressed as hyperbilirubinemia, was the strongest predictor for both death and persistent fistula in our series. Preoperative TPN was associated with death, together with a low serum albumin and a raised CRP and WBC. A low serum albumin reflects not only malnutrition but also a systemic inflammation seen in these patients. These circumstances demonstrate that the preoperative care must be capable of treating infections, controlling systemic inflammation, and providing proper nutrition without endangering liver function for several months in preparation for definitive surgery. To preserve liver function, techniques for giving enteral tube nutrition are preferable and possible in many patients. In the later part of our series, enteral nutrition via nasogastric sond or percutaneous gastrostomy was introduced, thus reducing the need of parenteral nutrition. Teubner (29) demonstrated that enteral nutrition by enteroclysis via an established fistula is an option, a technique that we have attempted only in some cases.
The study identifies four major reasons for failure after surgery for fistula: malnutrition, chronic systemic inflammation, liver failure, and surgical complexity. The first three are linked together and responsible for an impaired healing capacity. Staged operations with a stoma avoiding primary anastomosis will allow the patient to reverse the state of an impaired healing capacity and improve outcome. The findings emphasize the importance of perioperative care, choice of surgical strategy, and taking into account the surgical complexity when planning for the operation.