
Abstract
Background and Aims:
This study assessed the timing of reversal of defunctioning stoma following low anterior resection of the rectum for cancer and risk factors for a defunctioning stoma becoming permanent in patients who were not reversed.
Material and Methods:
Patients who underwent low anterior resection with defunctioning stoma during a 12-year period were assessed with regard to timing of stoma reversal. Delayed reversal was defined as >4 months after low anterior resection. Patients with a defunctioning stoma that was never reversed were assessed regarding risk factors for permanent stoma.
Results:
A total of 134 patients were analyzed. Of 106 stoma reversals, 19% were reversed within 4 months of low anterior resection, while 81% were reversed later than 4 months. In 58% of these patients, the delay was to due to low medical priority given to this procedure. The other main reasons for delayed stoma reversal were nonsurgical complications (20%), symptomatic anastomotic leakage following low anterior resection (12%), and postoperative adjuvant chemotherapy (10%). Of all patients, 21% (28/134) ended up with a permanent stoma. Risk factors for a defunctioning stoma becoming permanent were stage IV cancer (P < 0.001) and symptomatic anastomotic leakage following low anterior resection (P < 0.001).
Conclusion:
Four in five patients experienced a delayed stoma reversal, in a majority because of the low priority given to this surgical procedure.
Keywords
Introduction
Symptomatic anastomotic leakage following low anterior resection (LAR) of the rectum for cancer is a major complication with regard to morbidity and mortality, and it has a considerable impact on quality of life and health economy. The use of a defunctioning stoma (DS) has been shown to reduce the rate of anastomotic leakage after LAR (1–3). However, the DS itself contributes to morbidity, and reversal should therefore not be delayed. Moreover, reversal of the DS is associated with increased risk for morbidity and even mortality (4–10).
Stoma reversal is sometimes performed later than planned, and some studies have pointed out that stoma reversals may be given low priority in routine surgical practice (11–14). The primary aim of this study was to determine the proportion of patients with delayed stoma reversal following LAR and to assess reasons for delayed reversal. A secondary aim was to identify patients with a DS deemed permanent following LAR and to evaluate potential risk factors for a DS being deemed as permanent.
Material and Methods
Study Design
The present study included all patients operated with LAR of the rectum for cancer with a DS at the initial operation between June 1995 and December 2007 at the Department of Surgery, Örebro University Hospital, Sweden, and who hereafter had their DS reversed. Patients undergoing LAR without a DS at the index operation, or who later had an unplanned DS constructed, were not included. Patients who underwent additional abdominal procedures at stoma reversal were not included. Patients who never had their loop stoma reversed were excluded from the primary analysis but formed part of the secondary analysis.
The study was approved by the local ethics committee of the Uppsala-Örebro health care region. Patients who were alive in September 2010 were asked for written consent. Refusal of written consent was an exclusion criterion. Patient data were retrieved from the patient files of the Department of Surgery, Örebro University Hospital.
Planning of Stoma Reversal
An outpatient follow-up visit was planned to take place 1 month after hospital discharge following rectal resection. At this visit, stoma reversal was discussed with the intention to be performed within 4 months after LAR if the patient was deemed fit for surgery. Additional preoperative radiological examination of the neo-rectum was at the discretion of the examining surgeon and not mandatory. Stoma reversal performed more than 4 months after LAR was defined as delayed.
Variables Analyzed
Patient-related variables analyzed were age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, preoperative radiotherapy, and tumor-node-metastases (TNM) cancer stage. Surgery-related variables were operation time, intraoperative bleeding, hospital stay, frequency of readmission and reoperation within 30 days following stoma reversal, and time interval between initial LAR and stoma reversal.
Statistical Analysis
Categorical variables were analyzed using Chi-square test and Fisher’s exact test. Continuous variables were analyzed using Mann–Whitney U test. A P-value of <5% was considered significant. All statistical calculations were performed using Statistix® version 9 (Analytical Software, Tallahassee, FL, USA) and SPSS® version 17 (SPSS, Chicago, IL, USA).
Results
Patient Demography
Between June 1995 and December 2007, a total of 260 patients underwent LAR for rectal cancer at our institution. Of these patients, 140 (54%) had a planned DS and 120 (46%) did not, and these latter 120 patients were excluded from further analysis. A large majority of the patients had a loop ileostomy (n = 136), while loop transverse colostomy was infrequent (n = 4).
Of the 140 patients, 111 (79%) underwent subsequent stoma reversal and 29 (21%) did not. Five reversed patients and one nonreversed patient were excluded due to refused patient consent. Thus, the present analysis was based on 106 and 28 patients, respectively.
In the 106 patients who underwent stoma reversal, median age at the time of the rectal resection was 69 years, the proportion of female patients was 39%, median BMI was 25, 76% received preoperative radiotherapy, and 88% were classified as ASA class 1 or 2 (Table 1).
Demography and operative details of patients undergoing stoma reversal following LAR with defunctioning stoma (n = 106).
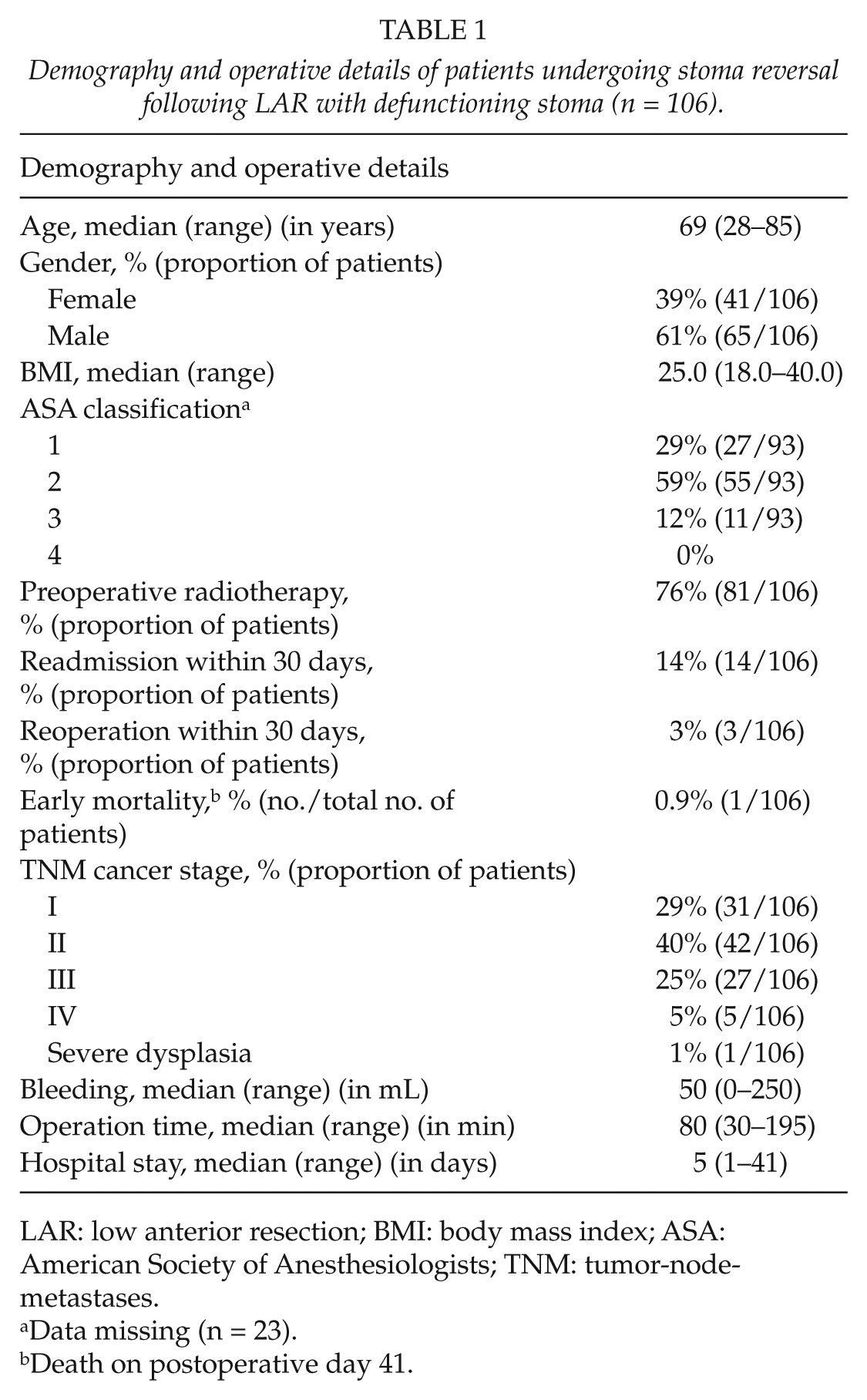
LAR: low anterior resection; BMI: body mass index; ASA: American Society of Anesthesiologists; TNM: tumor-node-metastases.
Data missing (n = 23).
Death on postoperative day 41.
DS and Reversal
A total of 106 patients underwent surgery for reversal of DS following LAR. Of these 106 patients, 19% (20/106) were reversed within 4 months of LAR according to the initial plan. The remaining 81% (86/106) were reversed more than 4 months after LAR (median = 7, range = 3–33 months) and were defined as delayed reversals (Fig. 1).
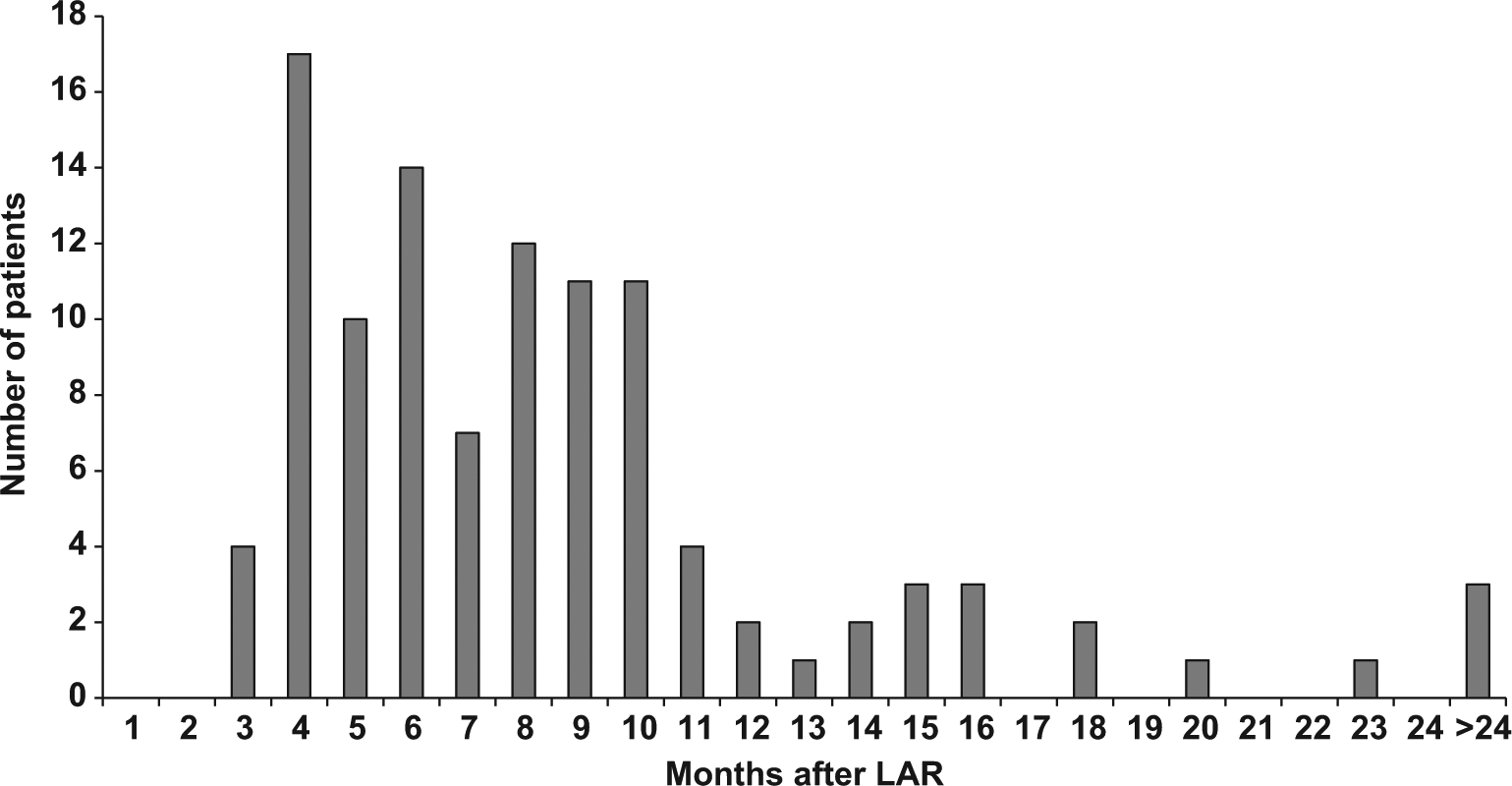
Distribution of stoma reversals over time following LAR for rectal cancer (n = 106). Stoma reversals at >24 months included reversal at 26 (n = 1), 31 (n = 1), and 33 (n = 1) months following initial LAR.
In 42% (36/86) of the patients with delayed stoma reversal, a medical reason for the delay was identified. The most important patient-related reasons for delayed reversal were nonsurgical complications during the postoperative period in 20% (17/86) of the patients, symptomatic anastomotic leakage following LAR in 12% (10/86) of the patients, and postoperative adjuvant chemotherapy in 10% (9/86) of the patients. The most common nonsurgical complications contributing to delayed stoma reversal were cardiovascular complications and thromboembolism (Table 2). In the remaining 58% (50/86) of the patients, no health-related reason for delayed stoma reversal was identified.
Reasons for delayed stoma reversal (>4 months) in patients operated with LAR and defunctioning stoma (n = 86).
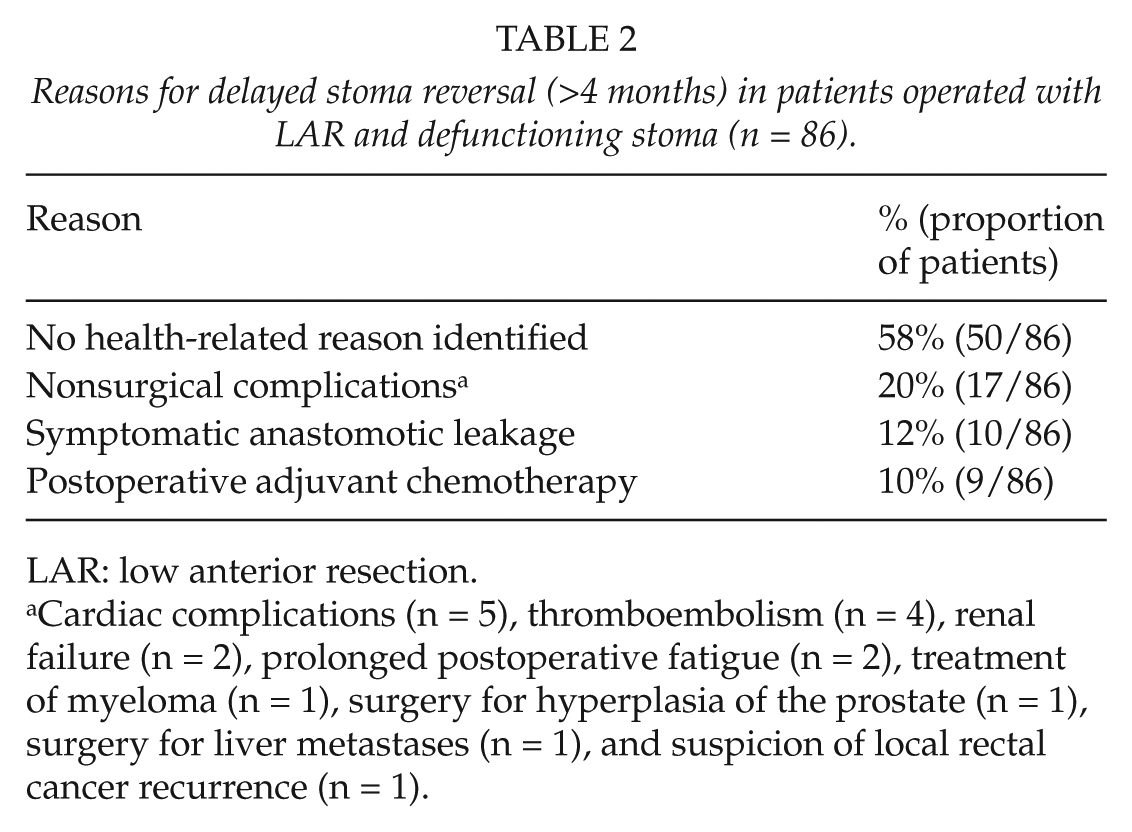
LAR: low anterior resection.
Cardiac complications (n = 5), thromboembolism (n = 4), renal failure (n = 2), prolonged postoperative fatigue (n = 2), treatment of myeloma (n = 1), surgery for hyperplasia of the prostate (n = 1), surgery for liver metastases (n = 1), and suspicion of local rectal cancer recurrence (n = 1).
DS Deemed Permanent
A total of 21% of the patients (28/134) who underwent LAR with DS stoma never had their DS reversed. The most frequent reasons for the decision to keep a DS were cancer stage IV in 50% of the patients and symptomatic anastomotic leakage following LAR in 21% of the patients (Table 3).
Reasons for a loop stoma deemed permanent in patients operated with LAR and defunctioning stoma for rectal cancer who never had their defunctioning stoma reversed (n = 28).
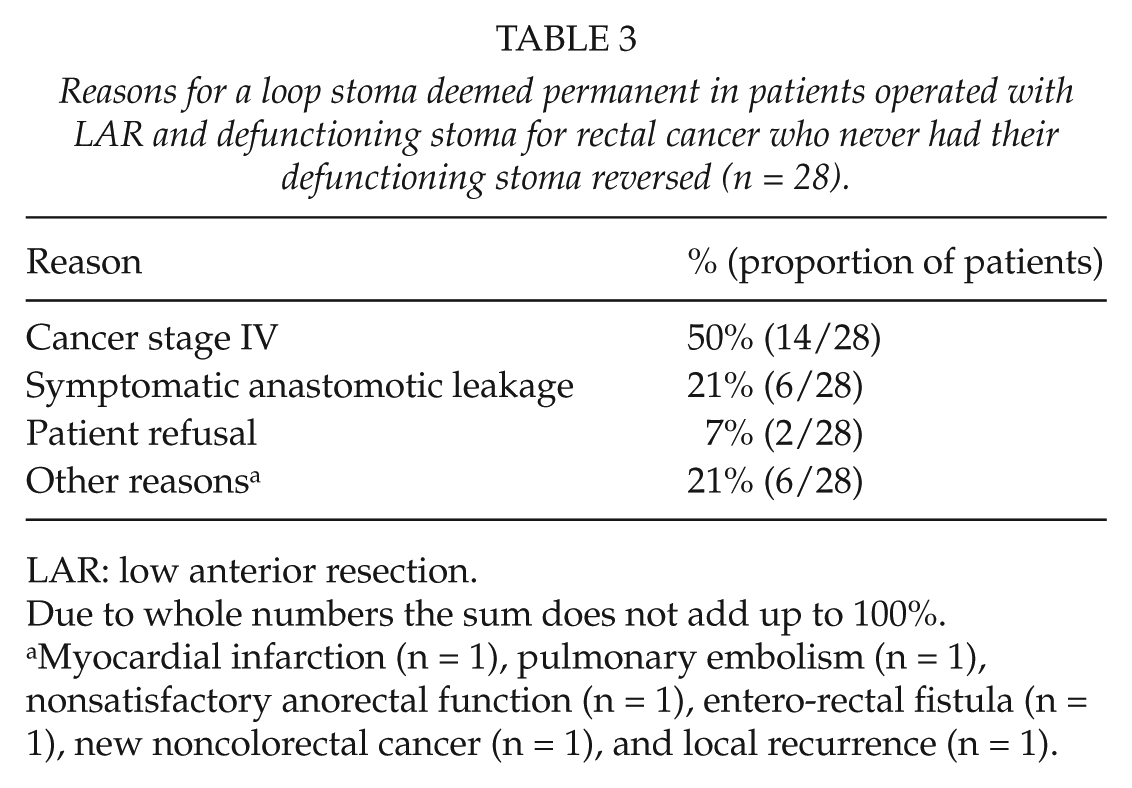
LAR: low anterior resection.
Due to whole numbers the sum does not add up to 100%.
Myocardial infarction (n = 1), pulmonary embolism (n = 1), nonsatisfactory anorectal function (n = 1), entero-rectal fistula (n = 1), new noncolorectal cancer (n = 1), and local recurrence (n = 1).
Comparison Between Patients Reversed and Not Reversed
A comparison was performed between the patients who had their stoma reversed (n = 106) and those who did not (n = 28). There were no differences between the groups with regard to age, gender, BMI, ASA classification, proportion of patients who received preoperative radiotherapy, intraoperative bleeding, operation time, hospital stay, or proportion of reoperations and readmissions following reversal of the DS. However, a significantly larger proportion of patients in the nonreversed group had stage IV cancer compared with those who had their stoma reversed: 54% (15/28) compared with 5% (5/106) (odds ratio (OR) = 23.3; 95% confidence interval (CI) = 7.3–74.7; P < 0.001). Moreover, symptomatic anastomotic leakage following LAR was more frequent in those not reversed compared with those reversed: 43% (12/28) compared with 12% (13/106) (OR = 5.4; 95% CI = 2.1–13.8; P < 0.001).
In all, 3% (3/106) of the patients developed symptomatic anastomotic leakage following stoma reversal, two of whom developed entero-cutaneous fistulas and were reoperated at a later stage. Altogether, 3% (3/106) of the patients were reoperated within 30 days following stoma reversal, due to anastomotic leakage (n = 1), abdominal abscess (n = 1), and ileus (n = 1).
There was no postoperative 30-day mortality among the patients undergoing stoma reversal. However, one patient deceased during the initial hospital stay following stoma reversal on postoperative day 41 due to postoperative rapid progression of preoperatively known extensive metastatic disease in the liver with subsequent hepatic failure. This case was considered as early mortality, although formally beyond postoperative day 30, and the early mortality in this series was thus considered to be 0.9% (1/106). Median follow-up time was 87 months (range = 33–183 months).
Discussion
The major finding in this study was that 4 out of 5 patients operated with LAR and a DS underwent stoma reversal more than 4 months after LAR and were subsequently considered delayed reversals according to the guidelines of our institution. In 42% of the patients, the delay could be explained by nonsurgical complications, symptomatic anastomotic leakage, and postoperative adjuvant chemotherapy. Adjuvant postoperative chemotherapy has been proposed as an important reason for delaying stoma reversal (12, 13); however, in the present study population, postoperative adjuvant chemotherapy contributed to a delayed stoma reversal in only one out of 10 patients.
The literature displays some uncertainty about the optimal timing for reversal of DSs, but generally reversal is recommended within 8–12 weeks following LAR. The rationale behind this recommendation is to obtain adequate healing while avoiding a prolonged presence of a DS with subsequent discomfort for the patient, risk for stoma-related complications such as dehydration, as well as higher treatment costs (4, 15). However, the actual time point for stoma reversal of DS in population-based settings is rarely described in the surgical literature, and therefore, it is not known how often DSs are reversed after 8–12 weeks in routine clinical practice. On the contrary, information on time point of stoma reversal is often specified in clinical trials (1, 16).
In contrast to some previous reports (13, 16), 58% of the patients in this study experienced a delayed stoma reversal without any evident health-related reason for the delay. We conclude that this was due to the fact that stoma reversal was given lower priority when competing with other benign conditions requiring surgery.
In a previous study, den Dulk et al. (15) showed that temporary stomas, which are not reversed within 12 months following rectal resection, have a high likelihood of becoming permanent stomas. This also holds true for the present study population, although 13% of the patients were in fact reversed after more than 12 months, and 3% even beyond 24 months.
Chand et al. (13) described the planning of stoma reversal following LAR as a contract with the patient. The aim of this contract was to schedule a date for stoma reversal together with the patient at the time of hospital discharge, a strategy that is appealing. In that context, this surgical treatment should be regarded as a two-component procedure, with LAR and formation of a DS as the first component, and the stoma reversal representing the second component (13, 16, 17). As a consequence of our findings, our institution has adopted a new policy offering patients a date for scheduled stoma reversal before hospital discharge, under the condition that postoperative radiological findings, now routinely performed, are normal.
Weaknesses of the present study are the retrospective approach and the single-center setting. However, the population-based design as well as the long follow-up time are deemed as strengths.
Of all DS in this study, 21% were never reversed and subsequently became permanent stomas. The most important reason for a DS to become permanent in the present study population was stage IV cancer. However, it may be noted that 5% of all stoma reversals were performed in patients with already diagnosed metastatic disease. Another major reason for not reversing stomas was symptomatic anastomotic leakage following LAR. Results from recently published large studies have demonstrated that there is a risk between 18% and 25% for a DS to become permanent (11, 15, 18, 19). Symptomatic anastomotic leakage (11, 15, 18, 19) and increased age (15, 19) were identified as independent risk factors for permanent stoma, and the results of the present study are in line with these findings.
Altogether, the present results underline the importance of providing patients with proper information regarding the two principal alternatives for rectal cancer surgery, namely, resection with or without anastomosis. Moreover, this information should include the panorama of possible complications as well as the risk of a DS becoming permanent.
Conclusion
In the present study, 4 in 5 patients experienced a delayed stoma reversal. The majority of the delays were due to the low priority given to this surgical procedure within the present local health-care system. In all, 1 in 5 patients undergoing LAR for rectal cancer with DS ended up with a permanent stoma.
Footnotes
Acknowledgements
This work was presented in parts at the Swedish Surgical Week, Visby, Sweden, 22–26 August 2011.
Funding
The authors thank the Research Committee, Örebro County Council, Örebro, Sweden for supporting this research with a grant.