
Abstract
Background and Aims:
The insertion of prophylactic ureteral stents in traditional colorectal surgery has been debated for a long time. The aim of this study is to investigate the results of ureteric stent insertion in elective laparoscopic colorectal surgery in terms of complications and costs.
Material and Methods:
From June 2009 to June 2011 one or two prophylactic ureteral stents were placed in all patients undergoing elective laparoscopic resection of their colon or rectum.
Results:
A total of 89 patients took part in this study, 61% had a benign disease and 39% malignant. The mean time for ureteral stent insertion was 16 min if one-sided and 21 min if bilateral. Incidental findings were found in the bladder in four (4.5%) patients. In all, 13 (26%) male patients had a benign prostatic adenoma, and 3 (6%) male patients had a significant stenosis of the urethral meatus and required bouginage. Complications due to ureteral stent insertion were transient hematuria in 11 (12.3%) cases, postoperative urinary tract infections in 2 (2.2%) cases, and hydronephrosis in 2 (2.2%) cases. One patient suffered an accidental damage of the right ureter despite the presence of a stent; this was recognized intraoperatively. The total cost for a one-sided ureteral stent insertion is calculated at around €360, and for a bilateral ureteral stent insertion, it is around €410.
Conclusions:
The prophylactic use of a ureteral stent in laparoscopic colorectal surgery leads to minor complications and may be cost-effective.
Keywords
Introduction
The insertion of prophylactic ureteral stents in traditional colorectal surgery has been debated extensively without showing convincing advantages. In recent years, minimally invasive surgery has expanded its indications to include more complex colorectal procedures, which obviously increase the risk of damaging the ureter. The incidence of this complication associated with open abdominal and pelvic surgery ranges between 0.2% and 4.5% (1). To our knowledge, there are no reports in the literature of the incidence of this complication in laparoscopic colorectal surgery. There are obviously concerns about potential complications, for example, the risks of urinary tract infections (UTI) associated with the procedure, of postoperative hematuria and of the direct damage of the ureter by insertion of the stent itself, extra costs, and increase of the operation time (OT). Moreover, the cost of equipment and extra personnel may not be justified by the rarity of the complication.
The aim of this study is to investigate the results of ureteric stent insertion in elective laparoscopic colorectal surgery in terms of complications and costs.
Material and Methods
From June 2009 to June 2011, one or two prophylactic ureteral stents (Ureterschiene, Polyamid, Coloplast GmbH) were placed in all patients undergoing elective laparoscopic resection of colon or rectum. This was independent of the underlying pathology or past medical history. In the case of a low rectal or abdominal–perineal resection, the cannulation of both ureters was planned, and in all other cases only of the left one. A separate consent form for the ureteral stent was filled in and signed by all patients. The stent was inserted by one urologist after the induction of general anesthesia using a cystoscope with the patient in lithotomy position, before starting the surgical procedure.
The urology service is available in our hospital only for elective surgery as there is no 24-h prospective cover. We have a central computerized system (ORBIS EchtsystemPC) that allows us to book the urologist in theater and to inform them of the requested procedures.
The stent was routinely removed at the end of surgery, and only a bladder catheter was left in situ. All patients received a prophylactic single shot of cefuroxime or ceftriaxone and metronidazole at induction. Patients with covered diverticular perforation had a therapeutic dose of antibiotics for at least 3 days.
Data were collected retrospectively until December 2010 and prospectively afterward, using the hospital computerized data bank. Incurred expenses for equipment, personnel and operating room were evaluated according to price listing and personal communications.
Statistical Analysis
Continuous data are presented as mean (range) unless otherwise specified.
Results
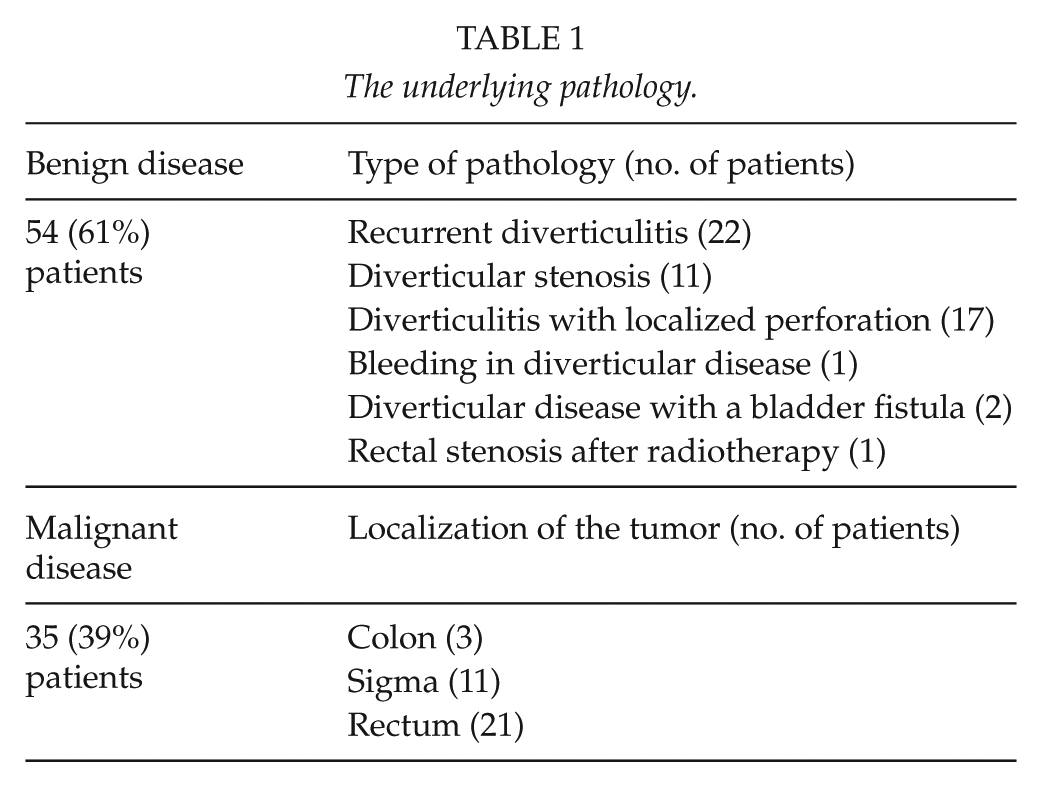
A total of 89 patients participated in this study, 39 (44%) female and 50 (56%) male, with an average age of 66 (range = 36–88) years. The underlying pathology was benign disease in 54 (61%) patients and malignant in 35 (39%) (see Table 1).
The underlying pathology.
There were 40 laparoscopic high anterior rectal resections, 27 laparoscopic sigma resections, 11 laparoscopic low anterior rectal resections, 7 laparoscopic left hemicolectomies, 3 laparoscopic assisted abdominal–perineal resection, and 1 laparoscopic assisted proctocolectomy with ileoanal pouch fashioning. Two of the laparoscopic procedures had to be converted to open (conversion rate = 2.2%). The OT was an average of 184 (range = 91–371) min. The average time for ureteral stent insertion was 16 (range = 7–35) min if only one-sided and 21 (range = 10–30) min if bilateral.
The cannulation of the ureter was abandoned in two cases due to kinking of the ureter. One patient undergoing a low anterior resection of rectum already had a left ureteral stent previously inserted for kidney stones.
Incidental findings were found in the bladder in 4 (4.5%) patients (1 urothelial carcinoma, 1 diffuse metaplasia, 1 papillary tumor, and 1 bladder steins). In all, 13 (26%) male patients had a benign prostatic adenoma, and 3 (6%) male patients had a significant stenosis of the urethral meatus and required bouginage.
Complications due to ureteral stent were transient hematuria in 11 (12.3%) cases and postoperative UTI treated with oral antibiotics in two (2.2%) cases. Two (2.2%) patients developed hydronephrosis due to edema of the mucosa: one of them was treated conservatively and the other one required a temporary reinsertion of the ureteral stent. One (1.1%) patient suffered an accidental damage of the right ureter despite the presence of a stent; this was recognized intraoperatively.
The cost of one ureteral stent is €4.09 (price listing). The other expenses included the sterilization of the cystoscope, between €45 and €50 and the extra OT (every minute of extra OT is valued in our hospital at around €10; personal communication, K. Rohde and D. Holst, 2012). We could not exactly value the cost of having an urologist in theater, although in the current German market, the locum rate for a consultant ranges between €100 and €150 per hour.
Discussion
In 2009, one of our patients suffered an incidental damage of the ureter during a laparoscopic anterior resection of rectum for cancer. This was a difficult pelvic dissection, probably due to previous diverticulitis, and the left ureter was divided just before the bladder. The complication was intraoperatively recognized and repaired with an end-to-end anastomosis. A double-J stent was left in situ. The patient kept the urinary catheter for 3 weeks; the double-J stent was removed after 3 months after a normal intravenous urogram.
Since then, all our patients undergoing a laparoscopic elective colon or rectal resection have a prophylactic left or bilateral ureteral stent inserted after induction of general anesthesia.
Some authors (2–4) advocate the use of an infrared ureteral catheter as it is easily visible, especially in the learning phase of minimally invasive and complex pelvic surgery. This costs between US$205 and US$236.80 and can be left in situ if needed. But use of this catheter seems to be associated with a high incidence of postoperative hematuria (98.4%) (4), and there are concerns that they might produce a thermal damage to the ureter (3). From our experience, a normal ureteral stent is sufficient to help the surgeon identify the ureter with an incidence of postoperative hematuria in only 12.3% of our patients. The cost of this stent is less than €5.
The cost of extra OT is calculated at around €160 for one stent and €210 for a bilateral stent, which is similar to other reports (2). Some argue that the cost of extra OT is not justified by the rarity of the accidental damage of the ureter. Realistically, it would make a significant difference if this OT could be used for another surgical procedure or if the theater personnel could go home earlier. In addition, the time routinely spent to identify a ureter could range from 0 to 45 min (2), and this is theoretically reduced by the presence of a stent.
The total cost described by Bothwell et al. (5) (more than US$2000 per operation) seems expensive compared to results from our practice. The total cost, in our hospital, is about €360 for a one-sided ureteral stent (€160 for OT, €150 for the urologist’s time, €45 for sterilization of the cystoscope, and €5 for the stent) and about €410 for a bilateral ureteral stent (€210 for OT, €150 for the urologist’s time, €45 for sterilization of the cystoscope, and €5 for the stent). On the contrary, the cost of legal action as a result of a damaged ureter has been valued between US$600,000 and several million dollars (6). This obviously does not take into consideration the extra cost of prolonged hospital stay, investigations, and eventually surgery.
One of our patients (1.1%) had an iatrogenic accidental injury of the ureter despite the placement of a stent, which is in range with other reports (1, 7).
This illustrates the need for a clear and specific informed consent for the procedure and the clear documentation of any difficulty found at surgery (8). Even though a stented ureter could be damaged at surgery, the advantage of having a stent in place is that it helps in identifying the damage intraoperatively and to proceed with immediate repair (5). This reduces the long-term complications (9).
In our experience, as in other reports (2), the hematuria associated with the ureteral insertion is temporary and disappears without particular intervention. The patients may have to keep the urinary catheter for 36–48 h.
The UTI incidence was low (2.2%), and this could be explained by the fact that all our patients received at least a single shot of antibiotics and the UTI may have not been associated with the ureteral stent insertion but with the urinary catheter. The incidence of this complication in other patients undergoing colorectal procedures without a ureteral stent insertion is around 4%–5% (9, 10).
Other complications such as the laceration of the ureter by insertion of the stent have been reported (4) but are rare. The low incidence rate of complications in our experience could also reflect the expertise acquired by the entire team as the ureteral stent is routinely inserted in all elective laparoscopic colorectal procedures. Kyzer and Gordon (1) found in a review of 120 ureteral catheterizations for colorectal operations that only 27 (5%) patients benefited from the procedure, but to limit the insertion of a ureteral stent only to assumed difficult cases increases the potential complications associated with the procedure.
In seven cases, incidental findings were reported related to the urinary tract and required further investigations or treatment. A benign prostatic adenoma was reported in 13 male patients, although this could have already been reported in the past medical history.
Despite this being a monoinstitutional observational study conducted only in part prospectively where some complications may not have been recorded, the prophylactic insertion of a ureteral stent was associated with minor complications. Some (1, 5) case-controlled studies have not shown a real benefit in the insertion of a ureteral stent, but usually the prophylactic insertion of a stent is limited to patients expected to have more complications during OT (Crohn’s Disease or complicated diverticula disease). Only a multicentric randomized trial would give a definitive answer.
Footnotes
Acknowledgements
The authors would like to thank the colleagues of the urology department (Dr Fiebag, Dr Urdahl and Dr Noll) for their expertise and their help.