
Abstract
Despite major developments in the field of revision surgery in recent decades, the management of severe acetabular deficiency at revision arthroplasty, complex primary total hip replacement or after pelvic tumour resection remains a complex problem. The options available for the management of severe bone loss include the use of uncemented press-fit cups with or without metal augments, impaction allografts, allograft-prosthesis composites, custom-made triflange cups, hip transposition, reconstruction prostheses or various combinations of these. This paper describes defect classification, various treatment options, clinical outcomes, survival of reconstruction, and typical complications in relation to treatment.
Keywords
INTRODUCTION
The gold standard in the treatment of advanced osteoarthritis is hip joint replacement (5), which has restored the impaired functionality and provided pain relief to millions of patients with end-stage degenerative joint disease. According to the Swedish, Danish, Norwegian and Finnish arthroplasty registers, approximately 40,000 primary hip prostheses are implanted annually in the Nordic countries. Concurrently, more than one million arthroplasties are done every year worldwide, and this number is expected to double within the next two decades (22). Modern arthroplasty techniques and implant designs have served to unprecedentedly improve the long-term outcomes of the primary hip replacement surgery better than ever before. Given the vast increase in the total number of arthroplasties performed, the annual burden of reoperations also increases. The wear on the implanted joint in any type of bearing material releases particles into the surrounding tissue, which may cause tissue reactions and further osteolysis of the periprosthetic bone, aseptic loosening of the component and, if not treated within the optimal time, may ultimately lead to major bone defects (12). High-energy periacetabular fractures, the treatment of bone tumours and periprosthetic infections may also lead to major pelvic bone deficiency. Acetabular bone loss encountered at the time of revision arthroplasty can vary from mild to severe. Deficient acetabular bone stock poses a technical challenge for revision surgery because of reduced support from the anterior and posterior columns and varying degrees of medial wall and dome deficiency. In addition, as acetabular bone loss progresses, locating adequate bone for the placement of uncemented cup and fixation screws is increasingly difficult. Finally, limited contact between the host bone and the acetabular shell may impede osseointegration and long-term biologic fixation. The currently available treatment options for pelvic bone defects are numerous but often associated with inconsistent clinical results and substantial complication rates. To provide a comprehensive understanding of pelvic reconstruction in the setting of acetabular bone deficiency, we review the classification of bone defects, the present surgical treatment options, satisfactory postoperative appearance, and some complications encountered in the various procedures.
CLASSIFICATION OF PELVIC BONE DEFECTS
PAPROSKY CLASSIFICATION
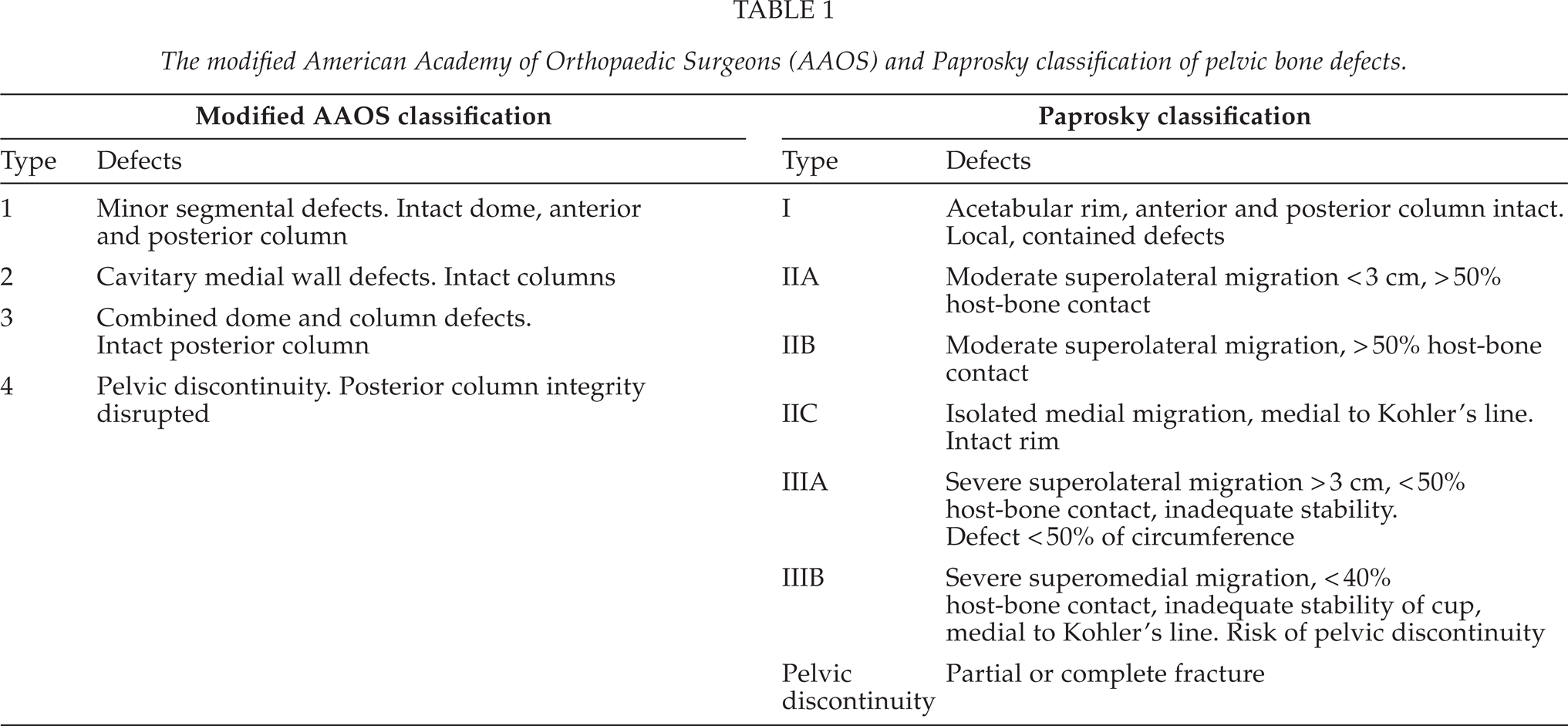
In the Paprosky classification, the evaluations are made using both radiologic findings and intraoperative views at the time of surgery. Pelvic defects are graded into three categories (Table 1). A type I defect has an intact acetabular rim with neither osteolysis nor migration of the component. Type II defect has a distorted intact rim with adequate remaining bone to support a hemispheric uncemented implant, and a type III defect has a non-supportive rim (20). Patients with type IIIB defect are considered to have a high risk for occult pelvic discontinuity (PD), which may influence their treatment, as they may need an additional posterior pelvic plate.
Periprosthetic PD describes the loss of structural bone between the superior and inferior aspects of the hemipelvis, resulting from bone loss or fracture through the acetabulum. The mechanism of PD is by either major segmental bone loss or a transverse acetabular fracture and it often occurs with type III defects. However, sometimes it may also be found with less severe bone loss.
AAOS CLASSIFICATION
The American Academy of Orthopaedic Surgeons (AAOS) originally developed its acetabular defect classification system to improve standardization in the reporting of acetabular revisions. It simplifies the Paprosky classification of the acetabular defects into four progressively graded types (Table 1). Type 1 defects are segmental and type 2 cavitary acetabular defects. In type 3 these two types are combined, whereas type IV defect includes PD.
BONE DEFECTS AFTER TUMOUR RESECTION
Various benign and malignant bone tumours and carcinoma metastases may also affect the bone in the pelvic area. The treatment depends on the tumour type; its histology, grade, and stage, and the location of the tumour. Curative surgical treatment requires wide or marginal margins. Whenever negative margins are possible, it often generates bone loss of various degrees in the pelvic area. The periacetabular area, especially if the resection includes regions P2 as classified by Enneking (Fig. 1) causes major demands in surgery as the hip joint needs to be reconstructed (27).
RECONSTRUCTION OF PELVIC BONE DEFECTS
UNCEMENTED REVISION CUPS WITH OR WITHOUT METAL AUGMENTS
An uncemented acetabular implant is usually suitable in Paprosky type I and II bone defects (type 1 and 2 in AAOS classification), where satisfactory outcomes have been reported (6). However, an uncemented component alone may not be sufficient in type III defects. In type IIIA defects, durable biologic conditions for bone ingrowth can only be achieved if the contact of the component with the remaining host bone is more than 40–60% (6). Implantation of an uncemented component is feasible but often requires the use of a structural augments or buttress plate to provide initial stability, allowing secondary bone growth and osseointegration to occur (19).
In type IIIB, the migration of the acetabular cup is superior and medial. Less than 40% of the host bone is in contact with the component, and the bone ingrowth required for the durable fixation of an uncemented component is compromised. Therefore, type IIIB defect frequently requires the use of additional allograft fused to the ilium, protected with an acetabular cage and a cemented polyethylene liner. Another reported option is the placement of an acetabular component on the host bone in a superior position (a high hip centre). However, this technique alters the lever arms of the abductor and adductor muscles and may expose the patient to hip dislocations. Moreover, patients with type IIIB defect are at high risk for occult pelvic discontinuity that may need additionally posterior column plating.
The modified American Academy of Orthopaedic Surgeons (AAOS) and Paprosky classification of pelvic bone defects.
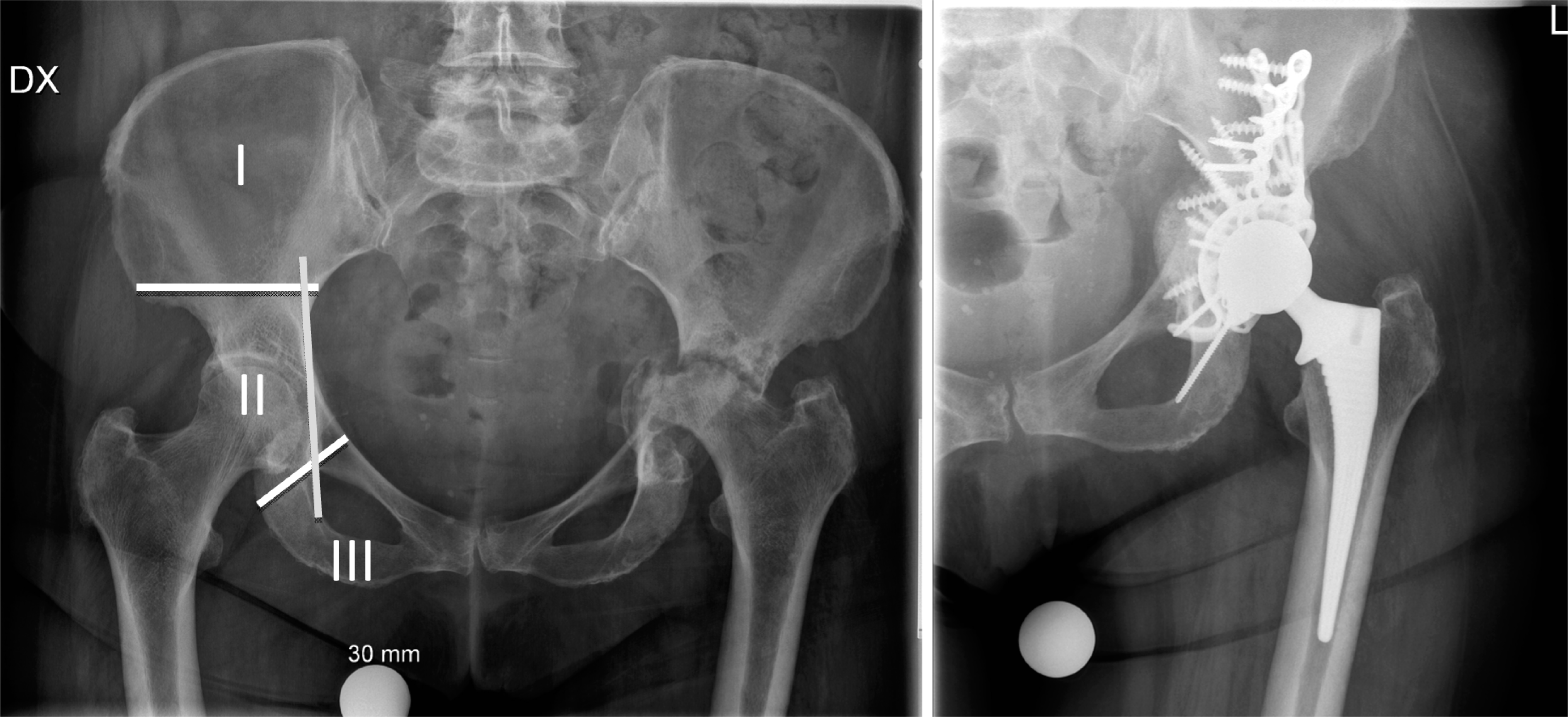
The pelvic defect of the left hip is classified as Paprosky IIIB and AAOS grade 4 including transverse fracture of both columns (pelvic discontinuity). The reconstruction was made using allograft impaction-grafting, reinforcement cup and posterior column plating (right). On the left picture the right hip illustrates the classification system for pelvic tumour resections according to Enneking. The localization is divided into three groups (white lines); region I (iliosacral), region II (periacetabular), and region III (ischiopubic). Kohler's line (ileoischial) is indicated by a vertical line. Severe medial protrusion is indicated, if the femoral head or cup component breaks this line (left hip).
REINFORCEMENT RINGS OR CAGES AND BONE PACKING
Impacted morsellized allografts provide an effective and widely accepted method to restore bone stock, and have yielded good clinical and radiological results (21). On the other hand, several reports have been published about the neurovascular injuries occurring with the placement of acetabular cages (16). In revisions with large acetabular bone defects or pelvic discontinuity, the impaction grafting technique carries an increased risk of complications (26). The thickness of the bone graft should be less than 15 millimetres, because the incorporation of the host bone may be insufficient to provide mechanical integrity for the allograft/bone composite. The rigid placement of the dome screws in the use of the reinforcement cages is of crucial importance to prevent micromotion of the cage and subsequent defragmentation or resorption of the graft (26). Mechanically, the reinforcement ring should be considered as an internal fixation plate for the acetabulum, into which the anterior and posterior columns are secured. In the absence of adequate mechanical integrity, the reconstruction is doomed to fail. In case of PD, an additional posterior column plate should be added as bridging-type fashion (Fig. 1).
CUSTOM-MADE TRIFLANGE CUPS
One of the modern options for treatment of extensive periacetabular bone defect is the use of custom-made triflange component (Fig. 2A). This is individually recreated by the data from a thin-cut computed tomography scan of the pelvis. This construct is designed to contain a central dome that fits tightly into the periacetabular defect, contacting the ilium superiorly. Three additional flanges arise from the central dome and provide three-point fixation on the remaining ilium, ischium, and pubis. The short-term outcomes using this method have been reported satisfactory (11). However, if osseointegration of the implant is incomplete, this method is prone to mechanical complications. This is true, particularly when the cranial support is deficient or especially in case of PD, when additional posterior column plating may be needed.
Disadvantages of the triflange implant include increased cost and limited availability of the construct. Waiting time for implant manufacture delays usually the surgery by 4–6 weeks. Furthermore, accurate placement of the iliac flange requires substantial exposure of the ilium, which increases the risk of nerve and vascular injury. The superior gluteal nerve and vessels are especially susceptible to damage.
USE OF STRUCTURAL ALLOGRAFTS, BONE SUBSTITUTES AND GROWTH FACTORS
Over the past 10 years, the use of structural allograft to compensate major bone loss has dramatically decreased. With the invention of newer implant designs, indications for these older techniques have become limited. The availability of structural human allograft bone has become limited by tightened legal restrictions. Additional concerns relate to the cost of harvesting, processing and storing allografts, immunogenicity and the risk of viral contamination.
One of the major advantages of bone allografts is that the bone can be shaped and customized in order to exactly match the pelvic defect (Fig. 2B). The complex osseous architecture can be fully restored for locomotion, avoiding a flail hip or an arthrodesis. However, little is known about the outcome of pelvic allograft procedures (3). Even though the early functional results of structural pelvic allografts have been promising, this method entails several problems. Structural pelvic allografts are associated with mechanical failure due to resorption and fragmentation of the allograft usually within 5–10 years after implantation (Fig. 2B), high infection rate and a total complication rate of 30% to 90% (3).
The use of bone substitutes is seldom a solution to the treatment of complex bone defects of the pelvic ring, because the defect size is usually too large to use bone substitutes alone. These may have a role in addition with morsellized bone allograft and growth factors. However, appropriately designed randomized controlled trials are required to compare the use of existing and new bone graft substitutes with established practice.
CONE AND SADDLE PROSTHESIS
McMinn et al. reported the fact that the posteromedial iliopubic part of the pelvis often remains intact even in the severely deficient acetabulum (17). The stemmed, uncemented acetabular component may provide conditions for initial stability and osseointegration without structural bone grafts and facilitate reconstruction of the centre of rotation (4). However, the initial good results reported by McMinn could not be reproduced by other institutions. Newer designs based on the McMinn prosthesis are currently in the market. While the long-term results of those implants are not known, the procedure is considered to be experimental.
The saddle prosthesis was developed in the late 70's for the reconstruction of large periacetabular tumour resections. The saddle shaped implant is typically supported by the remnant of the iliac bone at or above the level of the sciatic notch. The modular saddle prosthesis has a connection with the regular femoral component. However, reconstruction with saddle prostheses after major pelvic defect has a high risk of complications and poor long-term functional outcome with limited hip flexion. Superior migration of the reconstruction in osteoporotic or metastatic bone is frequently reported (13).
HARRINGTON'S PROCEDURE
Surgical reconstruction of periacetabular pelvic lesions is complex and presents a great reconstructive challenge. Lytic lesions in the periacetabular area are also caused by tumours or more often bone metastasis. The treatment of bone metastasis entails a different surgical ideology from that of PD caused by fractures or periprosthetic failures. Patients with bone metastases have a limited life expectancy together with a need of full motion and weight bearing postoperatively. Harrington's procedure was first described by KD Harrington in 1981 to meet these challenges (9). Later, numerous modifications have been introduced, but the idea of transferring the weight load from the acetabular joint into the intact bone in the ileum over the lytic lesion in the periacetabular area via threaded screws or pins and reinforcement ring has remained the same (Fig. 2C) (2, 14, 18, 25). The results of Harrington's procedure in this specific group of patients with bone metastasis are good as the durability of the reconstruction exceeds the patient's expected lifetime. Using Harrington's procedure among healthy patients with pelvic bone defects due to other causes has not been investigated and it is therefore not recommended so far.
HIP TRANSPOSITION
Pelvic tumours in the periacetabular area may grow very large before becoming evident. The surgical challenge is to achieve wide margins but to have adequate soft tissue left over to cover the reconstruction chosen. These reconstructions include endoprosthetic replacement, composite reconstruction with massive allografts and suitable endoprosthesis. Limited soft tissue coverage with these substantially sized reconstructions frequently leads to drawbacks and complications (1, 10, 15, 23). Hip transposition was developed to reduce this high rate of complications seen with other reconstructions. In hip transposition the reconstruction is done with a ‘;neo joint’ formed by the remaining femoral head together with the iliac wing or sacrum (Fig. 2B). Stability and remaining musculature attachment of the ‘neo joint’ are secured by using an artificial polyethylene tube (8). The primary disadvantage of this procedure is shortening of the leg, which on the other hand opens up opportunities for adequate soft tissue coverage and fewer complications. The functional results do not differ from those of other reconstructions and, therefore, hip transposition is a good to excellent surgical procedure in the treatment of periacetabular tumours (7).
TREATMENT OF PELVIC DISCONTINUITY
When pelvic discontinuity is identified, the decision should be made as to whether the discontinuity appears to be acute or chronic (24). An acute pelvic discontinuity has higher potential for primary healing and will have a small gap between the superior and inferior hemipelvis and therefore normal fracture reduction is possible with compression technique. A chronic discontinuity, on the other hand, has poorer potential for fracture healing, may have a large amount of fibrous tissue between the hemipelvis and sclerotic or non-vascularized bone or may even have had prior radiation therapy. If healing is possible, then the bone graft is inserted into the meticulously cleaned fracture gap and the pelvis is compressed with the inserted reinforcement ring and screws. If the healing potential is compromised, then modified Harrington's procedure may be recommended.

A: Disintegration of the reconstruction and large IIIA (AAOS grade 4) defect after semiarthroplasty of the left hip after high-energy trauma (left) was treated with a custom-made triflange cup (right). B: Left X-ray shows pelvic reconstruction using structural allograft and prosthesis composite after P1–3 resection of Ewing's sarcoma. Hip transposition after P1–2 resection of high-grade chondrosarcoma (right). The shortening of the limb is compensated with prosthetic reconstruction. C: Modified Harrington's procedure after embolization and intralesional resection of periacetabular metastasis. The primary tumour was renal cell carcinoma. The tumour cavity was filled with methacrylate bone cement. The reconstruction divides the weight bearing forces for the entire hemipelvis and prevents further protrusion of the cup.
Regardless of age of the PD, posterior column plating is recommended to prevent further separation of the superior and inferior hemipelvis, and subsequent collapse of the reconstruction.
SUMMARY
Many options are available in revision hip arthroplasty for the treatment of complex periacetabular defects. The optimal method should be selected according to the experience of the operative unit and surgeon, the extent and type of present bone loss and the patient's life expectancy. The ability to achieve a rigid, stable construct that allows for the osteointegration of the chosen implant, increases long-term predictable implant survival. In most demanding reconstructions, a combination of multiple methods may achieve the mechanically best outcome. The general principle in hip revision surgery is to increase, or at least retain, bone stock in the pelvis for future needs. This is of major importance especially in the treatment of younger patients. It should be kept in mind that only the use of morsellized allograft, if incorporated, has a remarkable additive effect on bone stock. Structural allograft, on the other hand, is substituted by the patient's own vital bone only at the edge of the graft. Similarly, the use of trabecular metal cups and augments occasions only minor net changes in bone stock.
Infection is a major surgical complication in pelvic reconstruction, regardless of the method of reconstruction. Its prevalence has ranged from 0% to 37% in series ranging in size from nine to 96 patients (3). Whenever complex reconstruction becomes infected, the consequences are catastrophic, and the whole limb is in danger. Other frequently seen complications of the reconstruction include joint dislocation, mechanical failure, and neurovascular lesions.
The overall outcome of reconstruction after complex pelvic bone defect is dependent on several different issues including patient selection, appropriate preoperative planning and templating, proper surgical technique, and good postoperative care and rehabilitation. Given that these patients are demanding to treat, it is all the more important that they are referred to treatment in specialized high-volume units to minimize complication rates.