
Abstract
Background and Aims:
Chronic presacral sinus (CPS) following anastomose leakage is one of the most serious complications after restorative colorectal surgery. CPS is associated with long course of treatments and can prevent stoma closure. We present our experience with endoscopic stapled marsupialisation (ESM) of CPS.
Materials and Methods:
Seven patients underwent ESM. All patients had developed a CPS after clinical anastomotic leakage following low anterior resection with diverting ileostomy. Initially the patients were treated conservatively and with endoscopic vacuum-assisted closure (Endo-VAC).
Results and Conclusion:
ESM procedure was successful for six patients, resulted in good healing in four patients and no sinus recurrence of the CPS. In two patients the stoma was reversed. Two patients were treated with neo-adjuvant chemoradiotherapy, who also developed small bowel fistulae. ESM is a simple treatment for CPS and can accelerate healing of chronic presacral cavity, reduce complications and enable to reverse the stoma in selected cases.
Keywords
INTRODUCTION
Clinical anastomose leakage following restorative rectal surgery has serious consequences with considerable morbidity and mortality. Despite improvements in anastomotic technique, anastomotic leak rates are still considerable high (1% to 24%). Much depends on the author's definition of leakage when it comes to calculating leak rates (1–3). The most common complication after anastomotic leakage is the development of a pelvic abscess, which often can be treated conservatively, including antibiotics and percutaneous/transanal drainage. Often a defunctioning stoma is required. When the acute sinus does not heal, especially if there has been a history of neoadjuvant chemoradiotherapy, there is a high risk of persisting chronic presacral sinus (CPS). Most CPS will resolve in time. However failure to diagnose the sinus, before the restoration of intestinal continuity, may result in a localised pelvic inflammation or pelvic sepsis. Symptomatic patients show evidence of localised pelvic inflammation or sepsis. Clinical presentation of a CPS is variable and sometimes asymptomatic sinuses are identified by contrast enemas or by endoscopy before restoration of intestinal continuity in patients with temporary stoma. These patients are usually followed by repeated contrast studies or endoscopic examinations to access the sinus prior to restoration of intestinal continuity. A CPS is associated with several ambulatory visits and long courses of treatments with complications which delays or may even prevent stoma closure.
There are several methods to manage CPS, among these; endoscopic vacuum assisted closure (Endo-VAC), mucosal advancement flaps, use of fibrin glue, endoscopic advancement flap, redo-surgery and recently endoscopic stapled marsupialisation (ESM) (2, 4–7). Although Pagni et al (8) had originally described the technique of ESM for opening constricted colorectal anastomoses in two patients; the same method has been utilized to treat a case of CPS (2). The aim of this report is to present our experience with ESM in the treatment of CPS.
MATERIAL AND METHODS
The study was initiated after the approval from the departmental review board was obtained. Informed written consent was obtained from all patients.
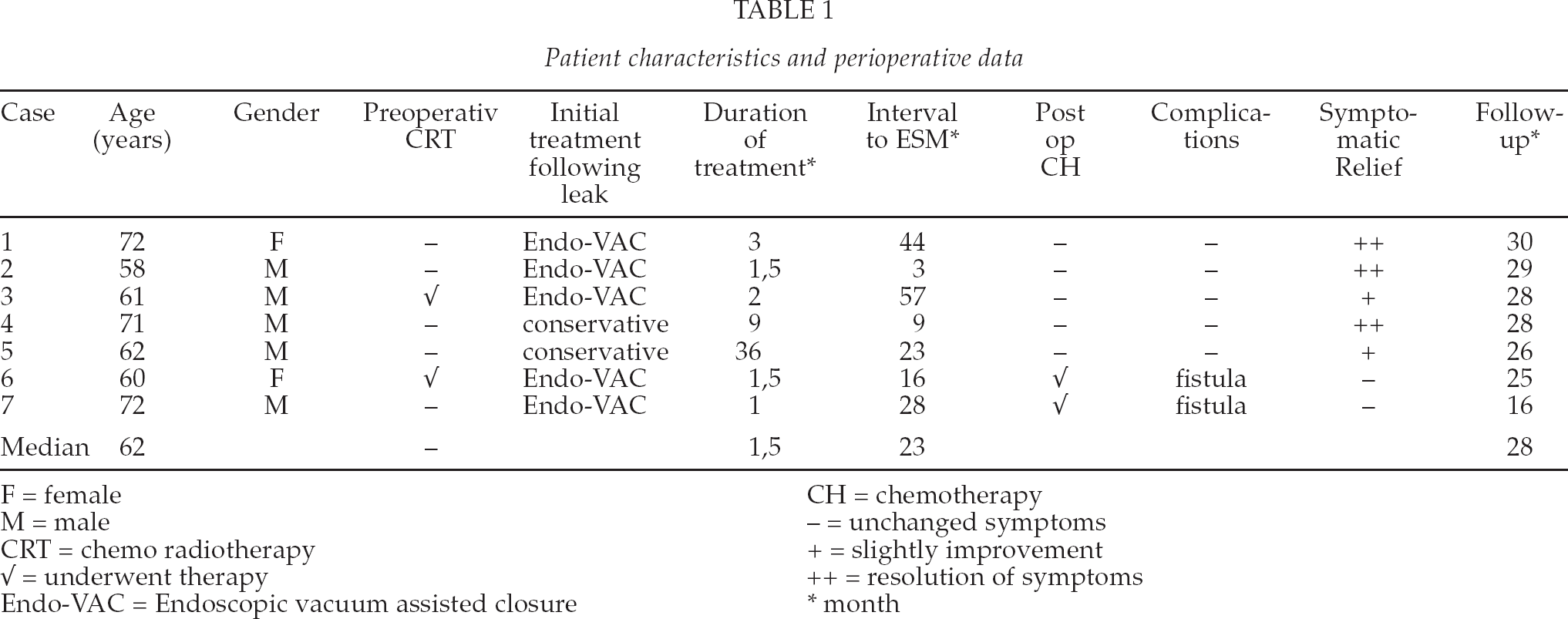
Seven patients who had CPS following low anterior resection (LAR) with diverting loop ileostomy were attempted to be treated by the technique of ESM between August 2009 and November 2010. The data was registered prospectively. The study included five males and two females with a median age 62 years (range 58–72) (Table 1).
Patient characteristics and perioperative data
F = female
M = male
CRT = chemo radiotherapy
√ = underwent therapy
Endo-VAC = Endoscopic vacuum assisted closure
CH = chemotherapy
= unchanged symptoms
= slightly improvement
= resolution of symptoms
month
Two patients had received preoperative long course neoadjuvant chemoradiotherapy and two were treated with adjuvant chemotherapy. All patients had a clinical anastomotic leakage, without the sign of peritonitis between 5–23 days (median 10 days) following LAR. Anastomotic leak was confirmed by contrast enema, endoscopy or computer tomography (CT). All patients were initially treated conservatively by intravenous antibiotic and transanal drainage. These patients, except two, underwent endoscopic vacuum-assisted closure (Endo-VAC). The duration of Endo-VAC treatment had a median of 1,5 months (range 1–3). One of the remaining two patients had poor anal function. He was referred from another hospital and treated with irrigation of saline. The other patient had denied the treatment with Endo-VAC and preferred conventionally rectal irrigation. All patients were evaluated with endoscopy, contrast enemas and CT or MRI prior to ESM. The reduction of wound size and the formation of granulation tissue were confirmed and measured by endoscopy. All seven patients underwent ESM procedure due to either unsatisfying effect of Endo-VAC treatment and continuous symptoms of perianal pain or discharge of pus per anus. The ESM procedure was successful in 6 out of seven patients. In one patient with poor anal function, the procedure failed due to insufficient exposure and difficulties to assemble of the Endo-GIA12 mm Universal (US Surgical Corp., Norwalk, CT, USA).
The surgical procedure was performed under general anaesthesia in the lithotomy position. After suitable dilatation of the anal canal, the sinus opening and anastomosis was identified using the Parcs anal retractor. The Endo-GIA 45 mm with green cartridge, was placed with one branch in the lumen of the rectum and the other branch in the sinus. The stapler was assembled and the common wall between the rectum and the sinus was divided using Endo-GIA 45mm (Fig. A). In long sinuses, more than one cartridge was used to staple the rectal wall. A preoperative prophylactic dose of broad-spectrum antibiotic was given. The patients were discharged in the afternoon or the following day. All patients were re-examined with endoscopy two and three weeks after the operation to determine healing of the sinus (Fig. B). Hereafter they were controlled regularly in every three month for the first year and then every six month or more depending on clinical condition of the patient.

Shows the presacral sinus (lower cavity) after ESM.

Presents the almost healed sinus 1, 5 month after ESM.
RESULTS
ESM was performed in six out of seven patients. Three patients had successful healing of the CPS and the ileostomy was reversed at 2,5 and 12 months, respectively. One elderly patient with ileostomy, who had reduced renal function and other comorbidities, was satisfied with her quality of life and was not interested in ileostomy reversal due to risk of complications. Another patient with poor anal sphincter function was previously treated with sacral nerve stimulation. The symptoms diminished dramatically after ESM, but the stoma was not reversed due to the high risk of anal incontinence. Two patients, previously treated with neoadjuvant chemoradiotherapy (CRT) and adjuvant chemotherapy developed a fistula between the marsupialized sinus cavity and the distal ileum after a 0,5 and 10 months respectively. They underwent further surgery with small bowel resection and Hartmann's procedure (table I). There have been no sinus recurrences or other complications during the follw up period of 28 to 30 months (median 28,5), for the 4 patients, in whom ESM was performed successfully.
DISCUSSION
Although there have been improvements in the treatment of rectal anastomotic leakage, anastomotic leakage still represents a major complication after restorative procedures with high morbidity and mortality (8). Brehant et al reported that 8% had a symptomatic sinus, demonstrated by contrast enemas before the planned ileostomy closure in pouch surgery (2). Persisting anastomotic sinus occurs in 5% after curative TME (Total Mesorectal Excision) and there is a risk of malignant transformation (3).
Patients often recover with sequela, like fibrosis of the colorectal anastomosis and surrounding tissue leading to stenosis. Studies have shown that the chronic inflammation and fibrosis associated with the sinus reduce neorectal capacitance and lead to worse bowel function (9). Many patients will then end up with permanent stoma or poor functional results.
The treatment of CPS is dependent on the presentation and the patient's general condition, co-morbidity and age. Once the leak matures into a CPS, there are several therapeutic options reported in the literature. Mucosal advancement flaps, anastomotic revision, end ileostomy and sinus unroofing have been treatments of choice (1). In the last decade, treatment with occlusive agents, e.g. fibrin glue is described by Swain et al (4) and Endo-VAC has been introduced (5, 6). Low-vacuum suction through a sponge inserted into the presacral space may lead to gradual closure. Weidenhagen et al. presented a study where definitive healing was achieved in 28 of the 29 patients, the mean hospital stay was 31 days and the total number of endoscopic sessions per patient was 11 (5). Another study comparing Endo-VAC with transrectal lavage and drainage showed that wound healing was significantly accelerated and hospital stay was slightly shortened in the group of Endo-VAC treatment. Endo-VAC treatment was performed in a median time of 27 days and showed better results when started within six weeks of surgery compared to those who started later (6). A recent report describing ESM in 4 patients following LAR for rectal cancer without any complications showed a mean healing time of ten weeks confirmed with contrast enemas. Only one patient was incontinent to gas and complained of faecal urgency and one complained of mild difficulty of evacuation, which resolved with the use of laxative (7).
Five out of seven of our patients were previously treated with Endo-VAC without any success in this series. Treatments within all five patients were initiated within six weeks. All underwent ESM. Two had their stoma reversed and one was satisfied with her life quality after the ESM procedure and did not wish an ileostomy reversal due to risk of complications. We believe that the ESM involve less ambulant visit for the patient and do not expose the patients for inconvenience, like carrying the vacuum wound drainage system, which is fixed to the CPS. They are discharged from the hospital the day after the ESM, thereby the hospitalization are diminished dramatically compared to patients treated with Endo-VAC.
Compared to the study of Alsanea et al. (7) the complication rate was higher in our study. Two out of seven patients in our study received preoperative CRT and both of them had complications to the healing of the CPS. It is known that preoperative radiation therapy doubles the rate of total and major perianal wound complications (10).
In all patients, except two who developed small bowel fistula, MR examination of pelvis together with contrast enema was used to rule out entrapment of small bowel in the area of sinus. CT examination was primarily utilised to diagnose metastasis or local recurrences. The number of our patients is too limited to reach a robust conclusion. However, careful selection of patients to this procedure with MR, CT and contrast enemas is important. Further investigations are needed to specify which selected patients are suitable for ESM.
We recommend that ESM only is used in the treatment of a chronic sinus cavity, so the wall between the presacral sinus cavity and the colon lumen are fibrous. ESM is a good alternative when the conservative, cutaneous/transanal drainage and Endo-VAC treatment fail in the treatment of the CPS.
ESM is a relative simple treatment method for patients with chronic presacral sinus. ESM can control pelvic infection, accelerate healing of the CPS and reduces the complications and increase the patients' functional ability and enable to reverse the stoma. It is crucial to thoroughly examine the patients preoperatively with endoscopy, contrast enemas/CT and pelvic MR and select the patients could benefit from ESM.