
Abstract
Background:
The aim of this study was to investigate trends in the incidence, diagnostics, treatment and survival of thyroid cancer in Tampere University Hospital (TAUH) region in recent decades.
Material and Methods:
New thyroid cancer cases from 1981 to 2002 were ascertained from the Finnish Cancer Registry. Follow-up data was collected from medical records of TAUH. Differentiated thyroid cancer (DTC; consisting of papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC)) patients' data was analyzed and divided into two equal time periods (1981–1991 and 1992–2002).
Results:
The total amount of thyroid cancer cases was 553, of which 427 (77%) were papillary and 72 (13%) follicular. Thyroid cancer was four times more common in females than in males and the median age at the time of diagnosis was 52 years.
The incidence of DTC was 4.5/100 000 in the earlier group and 6.0/100 000 in the later group (IRR 1.33, CI 1.11–1.60). The proportion of papillary thyroid cancer rose from 81% to 89% (p = 0.02) in two study periods. Median tumour size became smaller, from 25 mm to 15 mm (p < 0.001). Surgery became more radical as total thyroidectomies were performed almost exclusively on the later group (p < 0.001). Median cumulative dose of radioiodine (I131) therapy was higher in the later group (p = 0.04). There was no difference in number of cancer recurrences (p = 0.54). The prognosis of DTC was good; 10-year disease-specific survival was 92% in the earlier group and 94% in the later group (p = 0.43).
Conclusions:
The incidence of thyroid cancer has risen and proportion of papillary cancer has increased, however, median size of tumour has decreased. No difference was seen in either all-cause or disease-specific survival.
Keywords
INTRODUCTION
Thyroid cancer is the most frequent endocrine gland malignancy accounting for 0.5% to 1.5% of all malignancies. Incidence of thyroid cancer has increased worldwide in recent years (1, 2). The Finnish Cancer Registry reported 359 new cases of thyroid carcinoma in 2008. Thyroid carcinoma is almost four times more frequent in females than in males in Finland, 7.9/100 000 vs. only 2.1/100 000 in men. In Finland the 5-year survival rate in thyroid cancer is 93% for women and 90% for men (3).
Malignant tumours of the thyroid gland are of either follicular, parafollicular or stromal origin. The majority of thyroid carcinomas are differentiated papillary (PTC, 70–80%) and follicular (FTC, 10–20%) thyroid carcinomas. Highly aggressive and fatal anaplastic carcinoma (ATC) accounts for 5–10% of thyroid malignancies (4–6). Medullary carcinoma (MTC, 5–10%) derives from the parafollicular cells (7).
Recent studies have reported a steady increase in thyroid cancer incidence over time (8, 9). This increase has been accompanied by a change in the distribution of histological types with a notable increase in PTCs (10–12). One of the factors considered to be responsible for the increase of PTC appears to be an increase in the supply of iodine in the general population (13). Additionally, genetic factors have also been proposed as a contributory factor (14–16), between 5 and 10% of PTCs are known to be familial (17). Furthermore, increased awareness for thyroid cancer risks after the Chernobyl nuclear accident may be an additional factor. Finally, the wider availability of diagnostic tools may have also been important (18).
Despite the generally good prognosis for most patients, approximately 8–10% will eventually die of thyroid cancer (19). The primary treatment modalities used for thyroid carcinoma (i.e., surgery, radioiodine, and thyroid hormone) have been used for over 50 years, yet controversy persists regarding the most appropriate choice of therapies for different groups of patients (20).
Objective of this study was to evaluate the incidence, diagnostics, treatment and survival of thyroid cancer patients in TAUH region.
MATERIAL AND METHODS
The material consists of 553 unselected consecutive patients with thyroid cancer in Tampere University Hospital (TAUH) diagnosed 1981–2002 and followed up until 2007. The total population of the area was approximately 0.48 million in 2008 and has been stable over past decades. (Statistics Finland, www.stat.fi). Thyroid cancer cases from TAUH region were obtained from the Finnish Cancer Registry. All patient data was obtained from the medical records in TAUH. Surgery was mainly performed in TAUH and a few patients with occult carcinomas were operated on in regional hospitals. The pathological diagnosis was performed in TAUH pathology unit. Patients were followed up in the TAUH Department of Oncology with the exception of some occult cancers that were followed up at the TAUH Department of Endocrinology. Permission to use cancer registry databases was obtained from the Ministry of Social Affairs and Health.
The following epidemiological and tumour data were collected: pre-operative symptoms, fine-needle aspiration cytology, age at diagnosis, gender, type and number of surgical interventions, histological type and size of tumour, lymph node metastasis and distant metastasis, number and dose of I131 ablation therapy, chemotherapy or external radiotherapy, follow-up time and number of hospital visits, cancer recurrences, all-cause and cancer-specific deaths.
For further analysis, patients with PTC or FTC (n = 498) were classified into two time period groups according to year of diagnosis: earlier group 1981–1991 (n = 207); later group, 1992–2002 (n = 291). WHO criteria for histopathology have changed during past decades mainly regarding criteria for FTC. FTC cases were re-evaluated in order to assimilate the groups for the histopathological diagnosis. (21)
Primary thyroid lymphomas (n = 17) and squamous cell carcinomas of the thyroid (n = 3) were excluded from the final analysis. Patients whose diagnosis was established post mortem (n = 17), were also excluded from further analysis. In most of these cases, thyroid cancer was an occult finding in autopsy, but in five of these cases thyroid cancer was a cause of death (papillary carcinoma, follicular carcinoma, medullary carcinoma, one each of them and two anaplastic carcinomas).
Continuous variables are represented as medians with quartiles (Q1, Q3). T-test or Mann-Whitney U-test was used when appropriate. Nominal variables are presented as numbers of patients (%) and were compared using Fisher's exact test. Survival results were analysed using the Kaplan-Meier method. Survival curves were compared using the log-rank test. The incidence of thyroid cancer was analysed by Poisson regression analysis. Results are given as incidence rate ratios (IRR) with 95% confidence intervals. The differences were considered to be statistically significant if p-values were less than 0.05. The statistical analyses were conducted with the SPSS 14.0 software (SPSS Inc., Chicago, IL, USA) and Stata 8.2 (StataCorp, College Station, TX, USA).
RESULTS
Basic characteristics of the whole study group are summarized in Table 1. The only histological type without female predominance was medullary carcinoma.
Basic characteristics of the whole study group according to histological type.
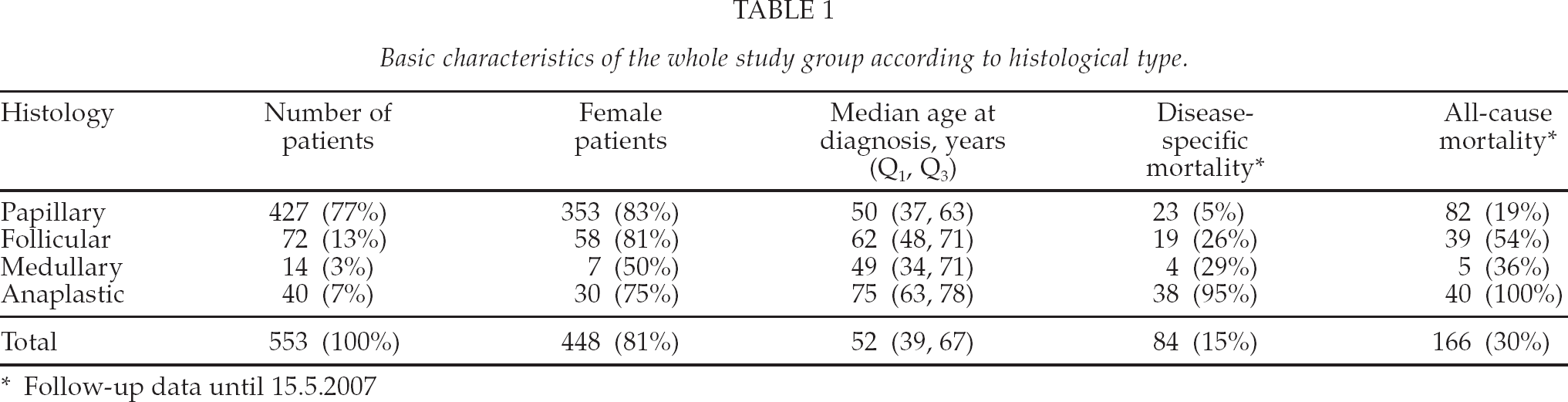
Follow-up data until 15.5.2007
We scoped in the analysis on patients with DTC (n = 498) as the other cancer histological cases are less common. Patients with DTC were divided into two groups according to the year of diagnosis. The earlier group consisted of cases diagnosed between 1.1.1981 and 31.12.1991 and the later group of cases diagnosed between 1.1.1992 and 31.12.2002. Incidence of DTC was 4.5/100 000 in earlier group and 6.0/100 000 in the later group. The incidence rate ratio was 1.33 (1.11–1.60) between groups. Incidence was on a steady increase as seen in Fig. 1. Two slight peaks in incidence were observed around the periods 1986–87 and 1997–98.
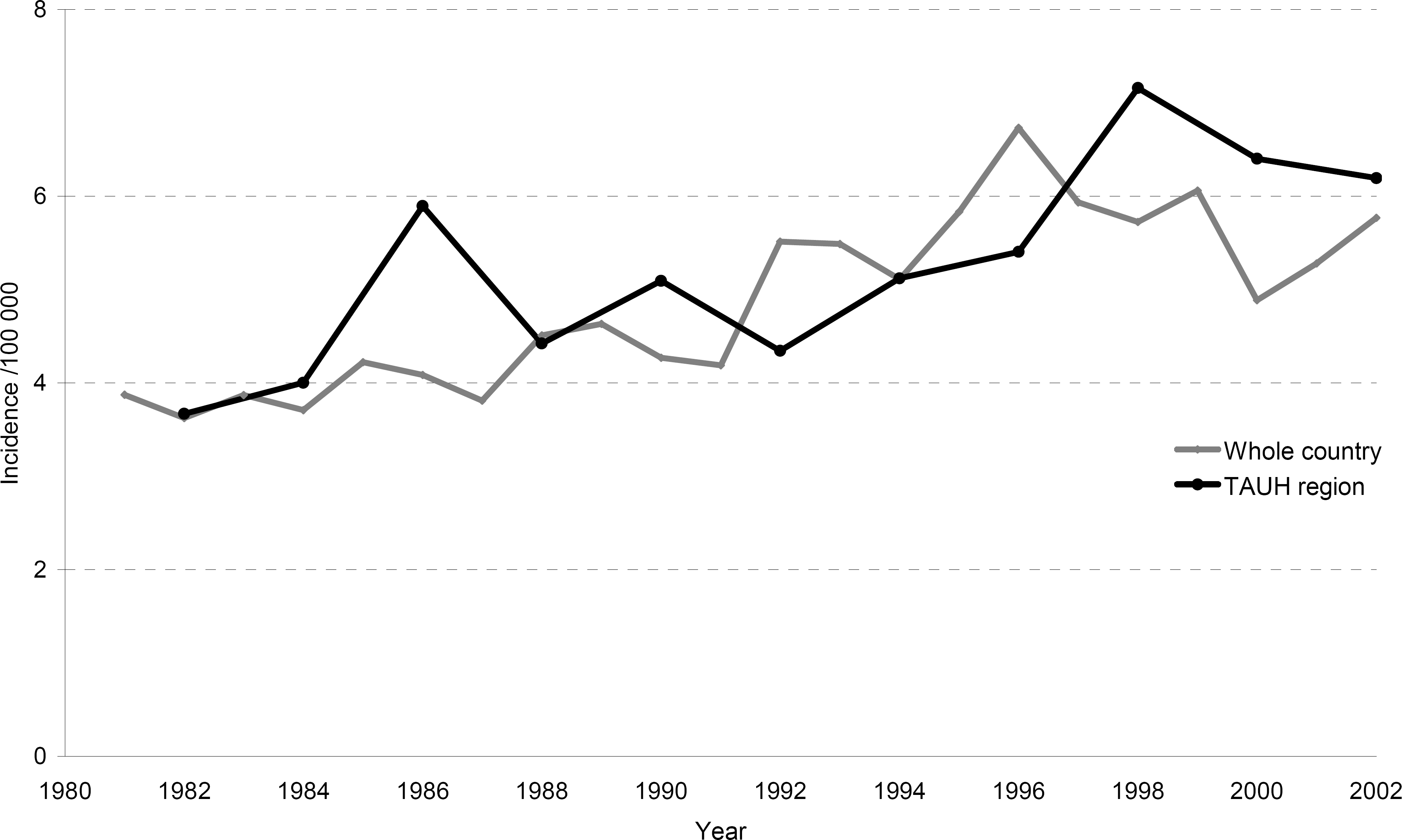
Increased incidence of DTC in TAUH region, 1981–2002 (black line). Incidence rate ratio = 1.33, CI (1.11–1.60) for time periods 1981–1991 and 1992–2002. For comparison incidence of DTC in Finland (grey line, data acquired from the Finnish Cancer Registry).
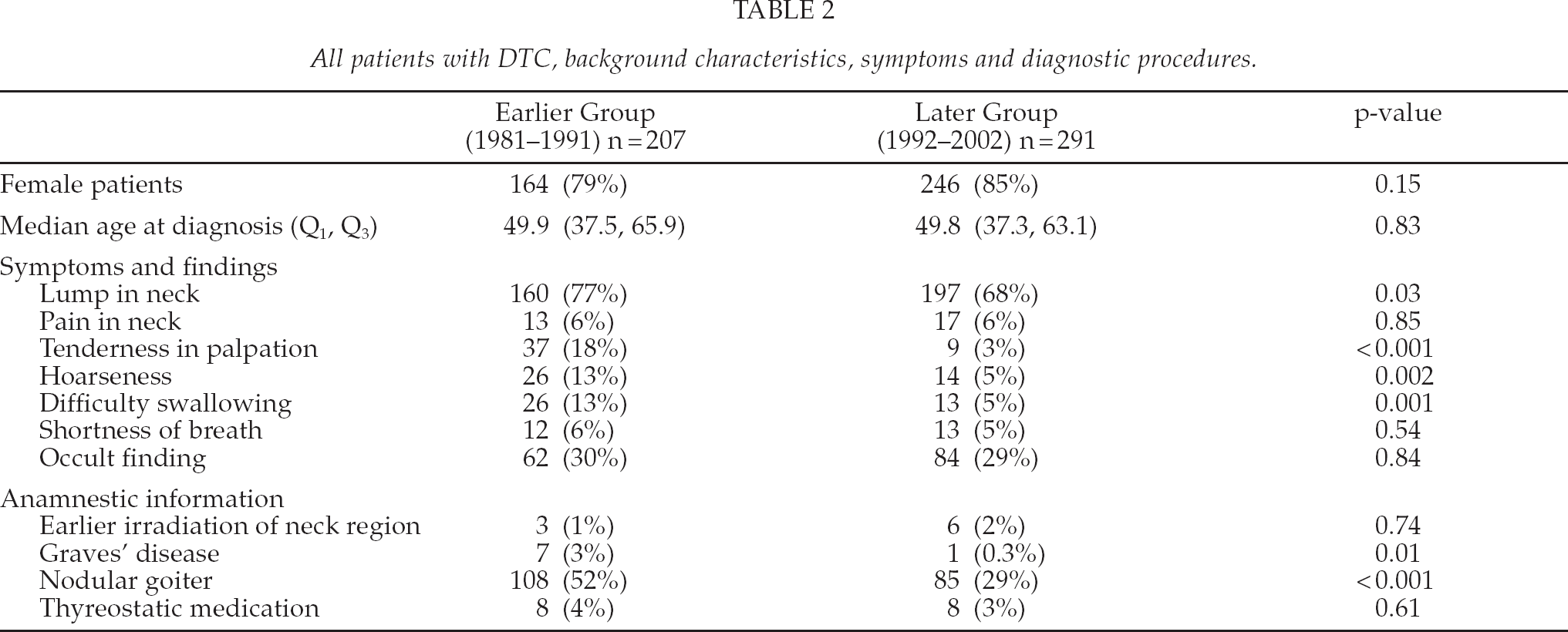
Basic characteristics of patients in both groups are summarized in Table 2. Median age at diagnosis was the same in both groups. The most common symptom of DTC was a lump in the neck. This finding was more common in the earlier group than in the later group (77% vs. 68%, p = 0.03). Tenderness in palpation, hoarseness and difficulty in swallowing were more common in the earlier group (p < 0.01). Nodular goiter was common in both groups, more in the earlier group (52% and 29%, p < 0.001). Pre-operative FNB results were obtained in 159 (77%) cases in the earlier group and in 239 (82%) in the later group (p = 0.17).
All patients with DTC, background characteristics, symptoms and diagnostic procedures.
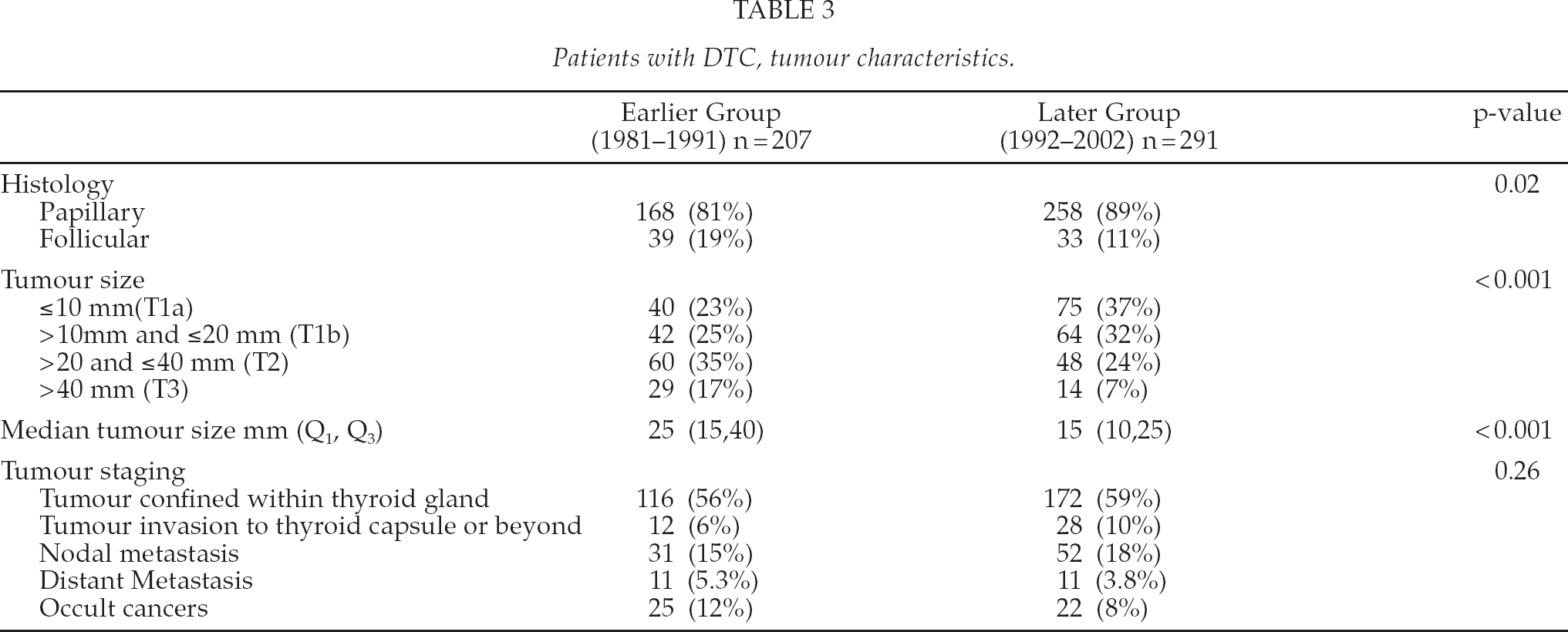
Information on tumour characteristics is summarized in Table 3. Type of cancer was papillary in 168 (81%) in the earlier group and in 258 (89%) in the later group (p = 0.02). Histology was re-evaluated in all FTC cases (n = 72). Tumour size was T1 (≤ 20mm) in 82 (48%) patients in the earlier group and 139 (69%) in the later group (p < 0.001). The median tumour size was significantly larger in earlier group (25 mm and 15 mm, p < 0.001). No significant differences were found in nodal metastasis, distant metastasis or rate of occult cancers. Location of tumour was right lobe in 90 (46%) and 135 (49%) cases, left lobe in 55 (28%) and 84 (30%) cases, isthmus in 12 cases in both groups (6% and 4%), bilateral in 23 (12%) and 29 (10%) and multifocal in 13 (7%) and 15 (5%) cases. Three ectopic cancers were found, one in the earlier group and two in the later group.
Patients with DTC, tumour characteristics.
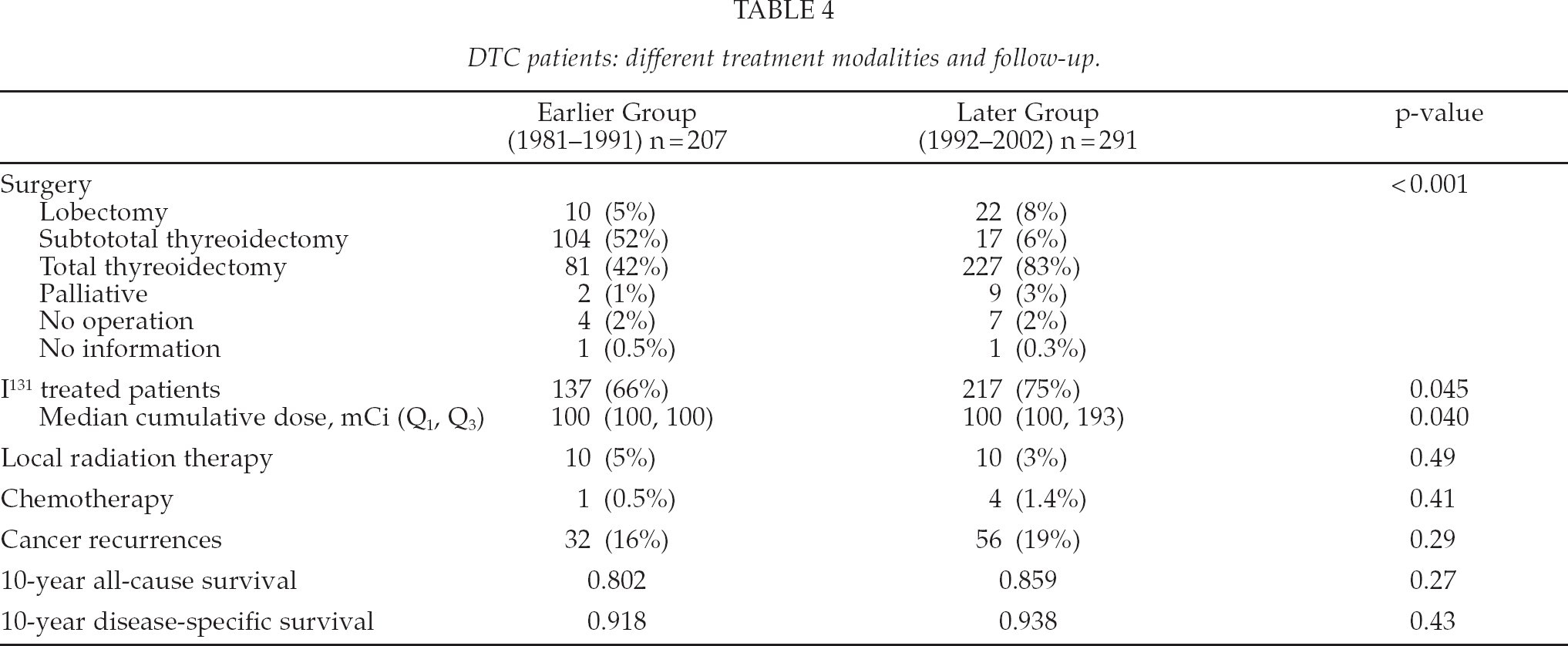
Patient's treatment modalities are summarized in Table 4. Preferred surgical procedure was subtotal thyreoidectomy in the earlier group (52% vs. 6%) and total or near total thyreoidectomy in the later group (42% vs. 83%). In the earlier group 137 (66%) patients and in the later group 217 (75%) patients received I131-treatment (p = 0.045). Most of the patients had only one I131-ablation treatment, 126 (61%) in the earlier group and 153 (53%) in the later group. Two or more ablations were given in 12 (6%) and 67 (23%) of cases. The most common dose was 100 mCi (3.7 GBq) in both groups. Median cumulative I131 dose was 100 mCi in both groups, with Q3 higher in the later group (100 and 193 respectively) (p = 0.040). Local radiotherapy was administered to 10 patients in both groups (4.9% and 3.4%). Only one patient (0.5%) in the earlier group and four patients (1.4%) in the later group received chemotherapy for differentiated thyroid cancer.
DTC patients: different treatment modalities and follow-up.
There were 32 (16%) cancer recurrences in the earlier group and 56 (19%) cancer recurrences in the later group (p = 0.29). Most recurrences were detected by increasing thyreoglobulin values. Median time for disease recurrence was 3.1 (0.3, 11) years in the earlier group and 3.7 (0.4, 12) years in the later group. The survival of the DTC patients is illustrated with Kaplan-Meier graphs in Fig. 2a and 2b. Ten-year all-cause survival was 80% for the earlier group and 86% for the later group (p = 0.27). Ten-year disease-specific survival was 92% for the earlier group and 94% for the later group (p = 0.43). Median follow-up time was 15.8 (0.1, 26) years in the earlier group and 9.0 (0, 16) years in the later group.
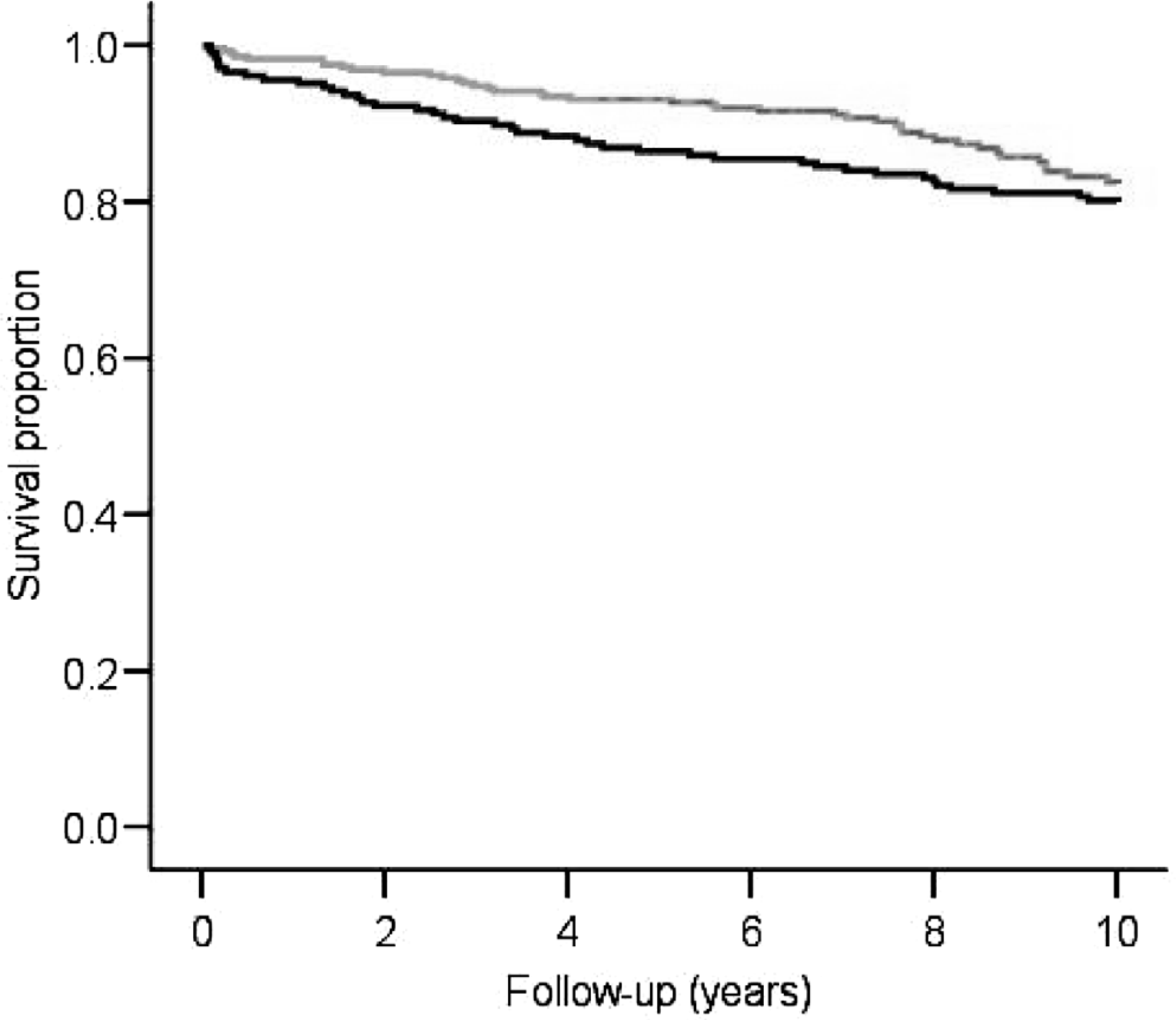
Overall survival was good throughout the study period with no difference between earlier and later group (p = 0.27). Earlier group (black line) and later group (grey line).
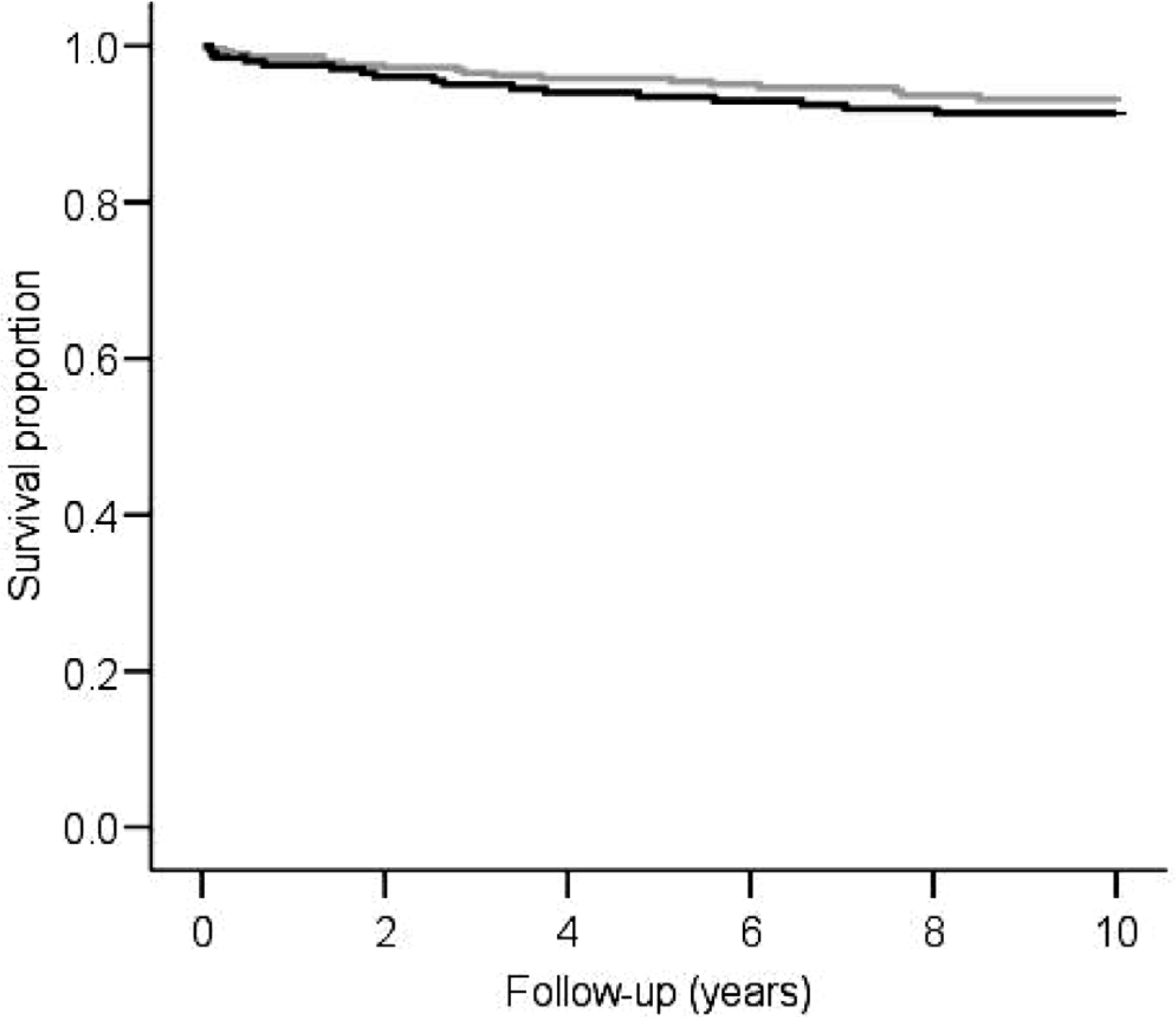
Disease-specific survival was almost identical in both groups. Earlier group (black line) and later group (grey line). p = 0.43
DISCUSSION
Significant changes have occurred in past decades in the diagnostics and treatment of thyroid cancer. Neck ultrasound started to be commonly available at the beginning of the 1990's, thus making it possible to detect and diagnose smaller subclinical thyroid nodules.
In our series, median age at diagnosis was 50 years in both groups. This finding is consistent with other recent studies (22, 23).
The incidence of DTC was rising from 4.5/100 000 in the earlier group to 6.0/100 000 in the later group. Slight peaks in incidence were observed around the periods 1986–87 and 1997–98. The earlier peak may be due to the increased awareness of thyroid cancer in general population due to the Chernobyl nuclear plant accident in April 1986. The later peak may also be related to the Chernobyl nuclear accident, as the fallout after the accident in TAUH region was the highest in Finland (24). The nationwide register also shows a slight peak in incidence in mid-1990s. Thus no significant difference exists with our series and nationwide register. The latent period of thyroid cancer after nuclear plant accident radiation exposure in adults is typically over 10 years, consistent with the findings (25).
There were differences in symptoms between groups. In the earlier group more patients felt a lump in the neck, had tenderness in palpation, hoarseness, and difficulty swallowing. The more frequent symptoms can most likely be explained by the fact that in the earlier group more patients had nodular goiter and the tumours were significantly bigger.
More PTCs were observed in later group. In DTCs, the proportion of PTC is increasing worldwide (10–12, 26, 27). In Elisei's study the proportion of papillary thyroid cancer increased from 80.5% to 91.0% (1). Reasons for this change are not fully understood.
Tumour size was significantly smaller in the later group. In Elisei's study the proportion of T1 tumours (< 20 mm) had increased from 43.3% to 54.5% and the increase in microcarcinomas (T1a, < 10 mm) was even more marked, from 7.9% to 28.7%. In our study, the findings were similar. The proportion of T1a microcarcinomas rose from 23% to 37% and the proportion of T1 tumours rose from 48% to 69% (p < 0.001). The availability and use of ultrasound may explain why smaller tumours were detected in the later group. Partially those tumours were also incidental findings; however incidentalomas' incidence stayed stable.
I131-treatments were more numerous in the later group and there was a statistically significant difference in cumulative median dose of I131. This may be due to more sensitive thyreoglobulin monitoring and interpretation of cancer recurrences. There was slightly more thyroid cancer recurrences in the later group, although the difference was not statistically significant. Most of the recurrences were detected by increased thyreoglobulin levels with a minority of recurrences detected by imaging studies or verified by cytology or histology. The reason for increasing trend in cancer recurrences, despite more aggressive surgical therapy and smaller primary tumours, warrants further studies.
Overall, the prognosis of thyroid cancer patients is good in TAUH region, the data are comparable to other recent studies (28, 29). No significant difference was seen in either all-cause or disease-specific survival. There was a slight difference in all-cause survival in short-term follow-up, but this could be explained with other factors, e.g. lower cardiovascular mortality during these time periods. The question arises whether more radical surgery, as seen in the later group, is justified or necessary when there is no statistical difference in disease-specific survival. Radical surgery may not benefit all patients, especially patients with low-risk DTC.
The reliability of the material in this study is good and the patients were non-selected. The study is retrospective and was conducted over long time-period.
The main findings of our study are as follows: The incidence of papillary thyroid cancer has increased, however the median tumour size has dimished. Surgery for thyroid cancer has become more radical, nevertheless no significant change in survival of thyroid cancer patients was detected.
Footnotes
ACKNOWLEDGEMENTS
We thank Dr. Tapio Salminen and Nurses Ritva Nuutinen and Anu Viitala, who participated in this study. We would also like to thank Risto Sankila from the Finnish Cancer Registry for his assistance.