
Abstract
Background and Aims:
The objective was to determine the sensitivity and specificity of Focused Assessment with Sonography for Trauma (FAST) in patients with confirmed liver lesions and also to compare results from surgeons trained in FAST with results from radiologists trained in general abdominal ultrasound as part of the specialist training. Explorative laparotomy or CT served as gold standard.
Materials and Methods:
This retrospective study included all patients admitted to our institution from 2003 to 2010 registered with the diagnosis “Injury of the liver or gallbladder”. Of 405 patients, 135 patients were eligible for analysis. Seventy-two patients were examined by radiologists and 63 by surgeons.
Results:
We found FAST to have a sensitivity, specificity, PPV, and NPV of 79.6%, 100%, 100%, and 68.9%. There was no statistically significant difference between FAST performed by radiologists and surgeons trained in FAST.
Conclusion:
FAST remains an important screening tool in abdominal trauma including liver lesions, and can be performed at a satisfactory level by surgeons trained in the FAST procedure only.
Keywords
INTRODUCTION
Focused Assessment with Sonography for Trauma (FAST) is a well-evaluated method for detection of intraperitoneal free fluid. The FAST method used today was introduced by Rozycki et al. (1) for blunt and penetrating abdominal traumas. Today FAST is used as a screening tool in many trauma centres to exclude intraperitoneal, intrathoracic, and pericardial bleeding, especially in haemodynamically unstable patients suffering from blunt abdominal trauma as recommended in the “European Guidelines for Management of Bleeding Following Major Trauma” and the “Advanced Trauma Life Support” (ATLS) guidelines (2–4). A rapid and accurate triage is crucial for the unstable trauma patient, as increased time to diagnosis and treatment is associated with increased morbidity and mortality (5).
Other studies have focused on evaluating FAST in populations of mixed trauma patients (6) or in populations of patients with blunt abdominal trauma (7–9). To study a population with a higher probability of haemoperitoneum, we selected a group of patients with confirmed liver lesions, where the incidence of intraperitoneal free fluid would be higher than in other trauma patients.
When FAST was introduced in our centre, it was performed by radiologists trained in general abdominal ultrasound; all trained according to the guidelines to the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) with a training level 2 or 3 (mid or highest level). Since there could be a delay caused by the radiologists not necessarily being in house on duty, surgeons took over the FAST procedure, after a limited training program previously described in detail (10). Our institution is the only level I trauma centre (11) in Denmark and handles the treatment of severe liver injuries in a region of 2.5 million inhabitants (2010).
The objective of this retrospective study was to determine the sensitivity and specificity of FAST in patients with confirmed liver lesions and also to compare the results of radiologists trained in general abdominal ultrasound (EFSUMB level 2–3 (12)) with the results of surgeons trained in the FAST procedure (EFSUMB level < 2). Explorative laparotomy or CT served as gold standard.
MATERIALS AND METHODS
PATIENTS
This retrospective study included all patients admitted to our institution from January 1st 2003 to December 31st 2010 registered with the ICD10 code S36.1 “Injury of the liver or gallbladder” as defined by the WHO. The search revealed 405 patients, of these 108 were excluded, mainly due to being patients with iatrogenic lesions of the biliary system. Among the remaining 297 patients, the main part were patients transferred to our institution with a FAST and a CT, as we are a tertiary referral centre, but in 135 patients FAST was performed at our institution before CT or explorative laparotomy. The 135 cases included both patients with isolated liver traumas and with multiple injuries. In 38 (28.1%) patients, an explorative laparotomy was performed and in 114 (84.4%) patients a CT was performed following FAST. In 17 patients (12.6%) a CT as well as an explorative laparotomy were performed. Of the 135 patients, 77 (57.0%) were male and 58 (43.0%) were female. The mean age was 29.9 years (SD 16.0 years). The majority, 118 patients (87.4%), had suffered from blunt abdominal trauma and 17 (12.6%) had suffered from penetrating abdominal trauma. Twenty-four (17.8%) were hypotensive at arrival (defined as systolic blood pressure ≤ 90 mm Hg), and 111 patients (82.2%) were normotensive at arrival (defined as systolic blood pressure > 90 mm Hg). Seventy-two patients (53.3%) were examined by radiologists trained in general abdominal ultrasound, and 63 (46.7%) were examined by surgeons trained in FAST.
DATA
Patients' medical records, radiology reports, surgical laparotomy reports, the register from the trauma centre, and electronic discharging summaries were retrieved and scrutinized. The following data were registered: Age, gender, time and date of admission, hospital of primary admission, trauma mechanism, blood pressure and pulse at arrival to the primary hospital or alternatively the first blood pressure and pulse registered in the medical records, results of FAST and specialty of the examining physician, signs of intraperitoneal free fluid on CT, and results of surgery.
FAST
We recorded findings of intraperitoneal free fluid (if possible in four different areas: Morrison's pouch in the right upper quadrant, the perisplenic space in the left upper quadrant, the pericardium of the epigastric region, and the pelvis). Only written reports have been available to the authors.
The results were divided into two groups, based on the training of the physician performing FAST.
STATISTICAL ANALYSIS
The statistical analysis was performed using PASW Statistics 18.0. For all groups sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated including 95% confidence intervals (95% CI).
RESULTS
GENERAL RESULTS
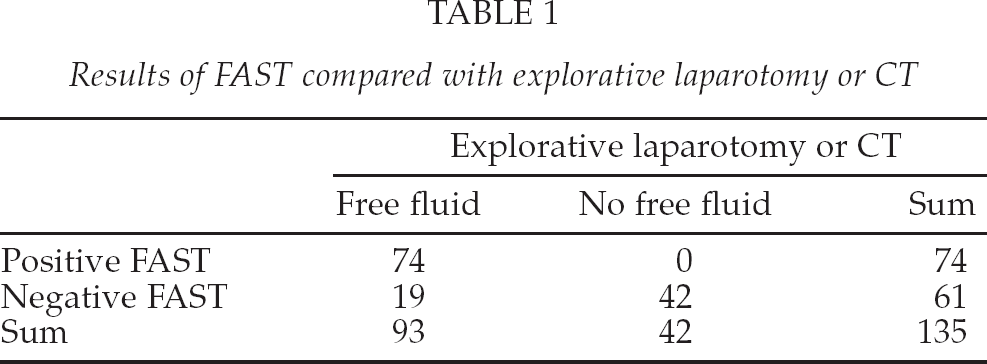
Table 1 shows the results of all 135 FASTs compared either explorative laparotomy or CT (if both were performed, FAST was compared with explorative laparotomy). The sensitivity was 79.6% (95% CI 69.7%–87.0%) and the specificity was 100% (95% CI 89.6%–100%). Positive predictive value was 100% (95% CI 93.9%–100%) and negative predictive value was 68.9% (95% CI 55.6%–79.8%).
Results of FAST compared with explorative laparotomy or CT
When FAST was compared with intraperitoneal bleeding at explorative laparotomy, the sensitivity was 75.8% (95% CI 57.4%–88.3%) and the specificity was 100% (95% CI 46.3%–100%). Positive predictive value was 100% (95% CI 83.4%–100%) and negative predictive value was 38.5% (95% CI 15.1%–67.7%). (Data not shown.)
When FAST was compared with presence of intraperitoneal free fluid on CT, the sensitivity was 74.3% (95% CI 62.6%–83.5%) and the specificity was 98.0% (95% CI 85.3%–99.9%). Positive predictive value was 98.2% (95% CI 89.2%–99.9%) and negative predictive value was 67.2% (95% CI 53.5%–78.6%). (Data not shown.)
There were no false positive FASTs in this study. One patient with a positive FAST had no free intraperitoneal fluid on CT, but bleeding was confirmed at explorative laparotomy.
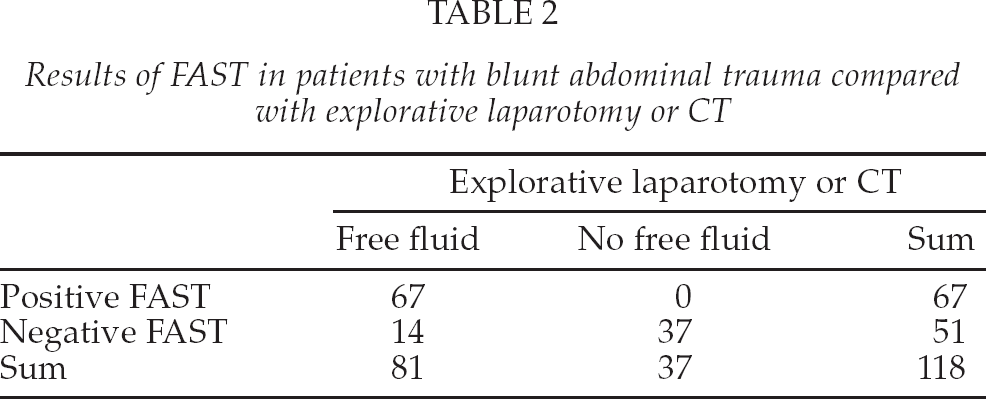
Among the patients suffering from blunt abdominal trauma, as shown in Table 2, the sensitivity was 82.7% (95% CI 72.4%–89.9%) and the specificity was 100% (95% CI 88.3%–100%) when FAST was compared either to explorative laparotomy or CT. The positive predictive value was 100% (95% CI 93.2%–100%) and the negative predictive value was 72.5% (95% CI 58.0%–83.7%).
Results of FAST in patients with blunt abdominal trauma compared with explorative laparotomy or CT
Among the 17 patients suffering from penetrating abdominal trauma, 7 FASTs were true positive, none was false positive, 5 were true negative, and 5 were false negative when compared with explorative laparotomy or CT. The sensitivity was 58.3% (95% CI 28.6%–83.5%) and the specificity was 100% (95% CI 46.3%–100%). The positive predictive value was 100% (95% CI 56.1%–100%) and the negative predictive value was 50.0% (95% CI 20.1%–79.9%). (Data not shown).
FAST AND THE TRAINING OF THE PHYSICIAN
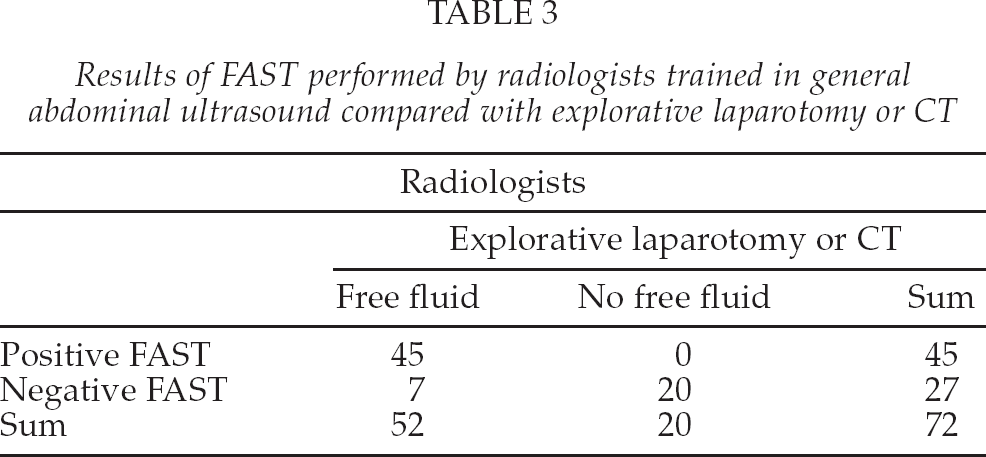
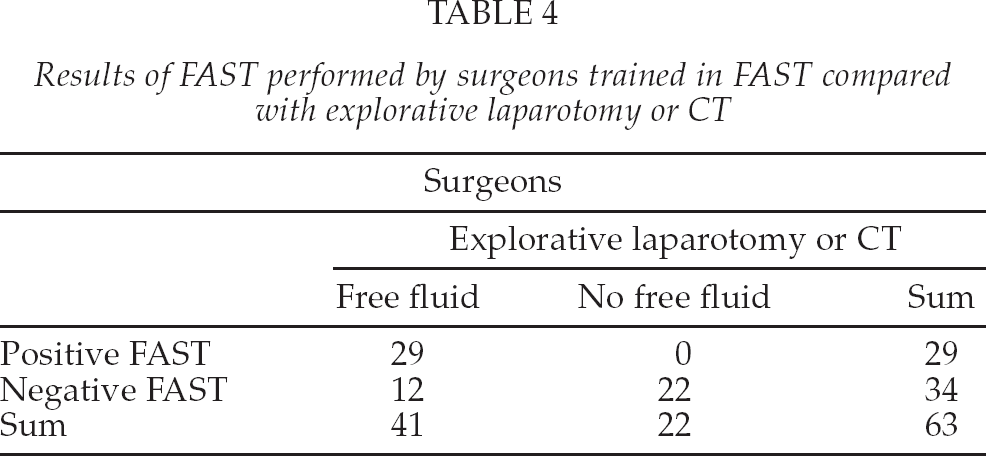
The results of FAST in the group examined by radiologists trained in general abdominal ultrasound are shown in table 3 and the results in the group examined by surgeons trained in FAST are shown in table 4. Both groups were compared with either explorative laparotomy or CT.
Results of FAST performed by radiologists trained in general abdominal ultrasound compared with explorative laparotomy or CT
Results of FAST performed by surgeons trained in FAST compared with explorative laparotomy or CT
When FAST was performed by radiologists trained in general abdominal ultrasound, the sensitivity was 86.5% (95% CI 73.6%–94.0%) and the specificity was 100% (95% CI 80.0%–100%). The positive predictive value was 100% (95% CI 90.2%–100%) and the negative predictive value was 74.1% (95% CI 53.4%–88.1%).
When FAST was performed by surgeons trained in FAST, the sensitivity was 70.7% (95% CI 54.3%–83.4%) and the specificity was 100% (95% CI 81.5%–100%). The positive predictive value was 100% (95% CI 85.4%–100%) and the negative predictive value was 64.7% (95% CI 46.5%–79.7%).
There was no statistically significant difference between the results of the two groups of physicians, but there seemed to be a trend towards the sensitivity being higher in the group of radiologists trained in general abdominal ultrasound.
DISCUSSION
To our knowledge, this is the first study evaluating FAST in a selected group of patients with confirmed liver lesions. This selected patient material had a higher prevalence of haemoperitoneum than an average trauma population. We found FAST in patients with confirmed liver lesions to have a low sensitivity of 79.6%, a high specificity of 100%, a positive predictive value of 100%, and a negative predictive value of 68.9% when compared to either explorative laparotomy or CT. There was no statistically significant difference between FAST performed by surgeons trained in FAST only (10) and FAST performed by radiologists trained in general abdominal ultrasound. The latter has never been reported before in patients with confirmed liver lesions.
Our results about the overall performance of FAST are in accordance with the literature. Stengel et al. (13) found FAST to have a sensitivity of 77.8% (95% CI 72.1%–83.5%) and a specificity of 99.4% (95% CI 99.2%–99.6%) in a metaanalysis from 2005 of 62 trials and 18,167 patients. In 1998, Rozycki et al. (14) published a sensitivity of 83.3% and a specificity of 99.7% in surgeon-performed FAST in 1,540 patients. She found FAST to be even more sensitive, 100%, in patients with either precordial or transthoracic wounds or in hypotensive patients with blunt abdominal trauma. In 2001, Brown et al. (7) found FAST to have a sensitivity of 84%, a specificity of 96%, and an overall accuracy of 96% in 2,693 patients with blunt abdominal trauma. The sensitivity was higher, 89%, in patients requiring explorative laparotomy. In 2005, Farahmand et al. (9) reported that in hypotensive patients, the sensitivity of FAST increased with the severity of the injury.
The minimum training requirements of EFSUMB covers several different specialties but not the FAST procedure. For those covering abdominal ultrasound, usually 300 to 500 examinations a year covering a wide variety of pathology is required as well as supervision of several hundred examinations. Training level 1 is the lowest; in this study the trained in general abdominal ultrasound were radiologists at least at EFSUMB level 2 with more than two years of experience. The learning curve for FAST has been determined in several studies and the recommended number of supervised examinations has varied between ten and one hundred (14–17). To our knowledge there is no European training requirements for the FAST procedure. When we started an introductory course on this (10), the course participants had ten supervised examinations at a one-day course and the remaining supervision had to be at a surgical department. The need for introducing the procedure for surgeons, reflected that they were present at the hospital after office hours leading to a relatively shorter time from injury to FAST, whereas the radiologists, although trained to a higher training level, were more likely to be on call from home. The time span from injury till bleeding occurs may also play a role in the detection of free fluid, which underlines the necessity for being able to repeat FAST on demand. Although in this present study, the sensitivity was highest for the radiologists trained in general abdominal ultrasound, the difference did not reach statistically significance.
The advantages of the FAST procedure are that it can be performed pre-hospital, upon arrival at the hospital, and be readily repeated. In haemodynamically unstable patients, FAST can help diagnose the need for immediate surgery, caused by the development of intraperitoneal free fluid, thus reducing the need for CT. Suthers et al. (18) argued that the strength of surgeon-performed FAST is the combination of FAST and the physical examination both being performed by the treatment-deciding physician. In this study, we have found this to be true. Another strength is that the attending surgeon stays with the patient and will be able to repeat FAST if clinically indicated. As the sensitivity of FAST is low, it is important to combine FAST with a clinical examination to ensure proper treatment of patients having a false negative FAST. Patients undergoing explorative laparotomy were likely to have more severe traumas with higher risk of developing intraperitoneal free fluid over time. As FAST was not always repeated, this can explain the NPV of only 38.5% in this group.
It could also be hypothesized that radiologists trained in general abdominal ultrasound might have a tendency to focus on additional aspects other than intraperitoneal free fluid while performing FAST. FAST is a screening for intraperitoneal free fluid and not a method for detection of specific organ related lesions (6–8, 19), the latter being more difficult to master than FAST (20). The overall sensitivity for ultrasound in abdominal trauma may be low if organ damage is to be considered (13) and for this aspect CT in the trauma protocol is superior.
This study has several limitations being a retrospective study limited by the data available in our archives. The time delay from the trauma to the first FAST examination was not always determined, and the same applied to the time from the FAST to the CT examination or surgery, aspects that could influence the result of the FAST procedure. A strength of this study is that we chose only a group who had confirmed liver trauma.
We have not investigated the impact of screening for visceral injury along with the FAST. Furthermore we included 17 patients suffering from penetrating abdominal trauma. However, in a meta-analysis by Stengel et al. (13) there was no difference in reported accuracy neither between trials including and excluding patients with penetrating abdominal trauma nor between trials including and excluding screening for visceral injury in the FAST algorithm. Finally, this study included patients of all ages including 17 children and babies less than 15 years old, even though paediatric FAST is known to have both lower sensitivity and specificity than adult FAST (13, 20). We have not calculated how this affected our results.
In conclusion, FAST remains an important screening tool in patients with abdominal trauma including liver lesions, and can be performed at a satisfactory level by surgeons trained in the FAST procedure only.